Taking lung sounds, or auscultation, is a critical skill in medical practice, allowing healthcare professionals to assess respiratory health by listening to the breath sounds produced by the lungs. The primary location for auscultating lung sounds is the chest wall, specifically over the lung fields, which are divided into anterior, posterior, and lateral regions. Key areas include the upper, middle, and lower lobes of both lungs, with each region corresponding to specific anatomical structures. To ensure accurate assessment, patients should be in a relaxed, seated or supine position, and a stethoscope is placed lightly on the skin to detect normal sounds like vesicular breathing, as well as abnormal sounds such as wheezes, crackles, or rhonchi, which may indicate underlying respiratory conditions.
Explore related products






What You'll Learn
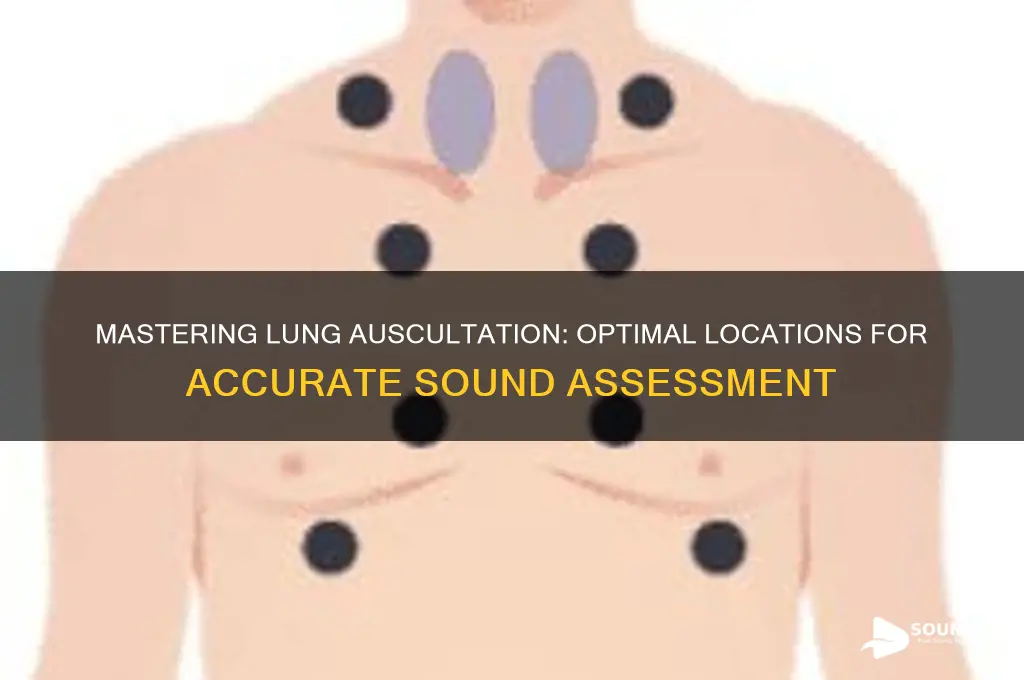
- Anterior Chest Wall: Auscultate upper/mid sternum, clavicles, and between ribs 2-6 bilaterally
- Posterior Chest Wall: Listen along scapulae, spine, and below scapular tips bilaterally
- Lateral Chest Wall: Assess axillary regions and mid-clavicular lines from ribs 6-10
- Anterior Axillary Line: Check lung sounds at 4th-5th intercostal spaces bilaterally
- Mid-Scapular Region: Focus on T4-T8 vertebrae for posterior lung field sounds
![]()
Anterior Chest Wall: Auscultate upper/mid sternum, clavicles, and between ribs 2-6 bilaterally
The anterior chest wall is a critical area for auscultation, offering a window into the upper lobes of the lungs and the central airways. Begin by placing your stethoscope at the upper and mid sternum, where you can assess airflow in the trachea and mainstem bronchi. This area is particularly useful for detecting stridor, wheezing, or abnormal breath sounds that may indicate upper airway obstruction or central lung pathology. Move laterally to the clavicles, ensuring you cover both the right and left sides, as asymmetry in breath sounds here can suggest conditions like pneumothorax or pleural effusion.
Next, focus on the intercostal spaces between ribs 2–6 bilaterally, a region rich with lung tissue. Start at the second rib, just below the clavicle, and work your way down systematically. In adults, this area corresponds to the upper and middle lung fields, making it ideal for identifying crackles, wheezes, or diminished breath sounds associated with pneumonia, COPD, or asthma. For pediatric patients, this technique remains largely the same, though the smaller chest size may require a more delicate approach and a pediatric stethoscope for optimal sound detection.
A practical tip for auscultation in this region is to ask the patient to sit upright or recline at a 30-degree angle, as this position maximizes lung expansion and improves sound clarity. Ensure the stethoscope diaphragm is firmly pressed against the skin to minimize ambient noise, and listen for at least 10–15 seconds per location to capture both inspiratory and expiratory phases. If using the bell, lightly place it on the chest to detect higher-pitched sounds like wheezes.
Comparatively, the anterior chest wall is often auscultated before the posterior regions because it provides a quick overview of central lung function. However, it’s important to note that posterior auscultation is equally vital for assessing the lower lobes. Combining both approaches ensures a comprehensive evaluation of lung health. For instance, crackles heard in the anterior upper lobes may suggest heart failure, while those in the posterior lower lobes could indicate pneumonia.
In conclusion, mastering auscultation of the anterior chest wall—from the sternum to the clavicles and intercostal spaces 2–6—is essential for diagnosing respiratory conditions. This technique, when paired with posterior auscultation, offers a holistic view of lung function. Remember, consistency in technique, patient positioning, and attention to detail are key to accurate findings. Whether you’re a novice or experienced clinician, this focused approach enhances your ability to detect subtle abnormalities and guide appropriate interventions.
Understanding the PAF Sound: A Guide to Its Origin and Impact
You may want to see also
Explore related products






![]()
Posterior Chest Wall: Listen along scapulae, spine, and below scapular tips bilaterally
The posterior chest wall is a critical area for auscultation, offering a window into lung health that complements anterior and lateral assessments. Position the patient in a seated or upright posture, ensuring comfort to facilitate deep breaths. Begin by placing the stethoscope’s diaphragm along the scapulae, tracing the spine, and extending below the scapular tips bilaterally. This region is particularly useful for detecting abnormalities in the lower lobes, such as consolidation, wheezing, or diminished breath sounds, which may indicate conditions like pneumonia or chronic obstructive pulmonary disease (COPD).
A systematic approach enhances accuracy. Divide the posterior chest wall into six zones: two along the scapulae, two below the scapular tips, and two paraspinal regions. Spend 5–10 seconds in each zone, instructing the patient to breathe deeply through the mouth. Note the symmetry of breath sounds; asymmetry may suggest obstruction or fluid accumulation. For pediatric patients, use a smaller stethoscope head and shorter auscultation times to maintain cooperation.
Comparatively, the posterior chest wall often reveals findings missed during anterior auscultation. For instance, posterior basal segments are more prone to gravity-dependent fluid accumulation in heart failure, manifesting as crackles. In contrast, anterior auscultation may appear clear. This underscores the importance of posterior assessment in differential diagnosis. Additionally, the posterior wall is ideal for detecting early signs of lung cancer or tuberculosis, which may present as localized wheezing or dullness to percussion.
Practical tips optimize efficiency. Warm the stethoscope to reduce patient discomfort, especially in colder environments. For obese patients, apply firmer pressure to ensure proper skin contact, but avoid causing pain. Document findings using anatomical landmarks (e.g., "crackles at T8 level, left side") for clarity. If using an electronic stethoscope, amplify low-frequency sounds to better detect rales or rhonchi.
In conclusion, auscultating the posterior chest wall is indispensable for comprehensive lung assessment. Its unique anatomical position allows detection of lower lobe abnormalities and gravity-dependent changes. By combining systematic technique, comparative analysis, and practical adjustments, clinicians can maximize diagnostic yield and tailor care to individual patient needs. Mastery of this skill bridges the gap between theory and practice, ensuring no pathology goes unnoticed.
Understanding Pleural Effusion: What Does It Sound Like and Why?
You may want to see also
Explore related products






![]()
Lateral Chest Wall: Assess axillary regions and mid-clavicular lines from ribs 6-10
The lateral chest wall, specifically the axillary regions and mid-clavicular lines from ribs 6-10, is a critical area for auscultating lung sounds. This region provides access to the middle and lower lung fields, where abnormalities like consolidation, wheezing, or diminished breath sounds often manifest. Proper assessment here can differentiate between conditions such as pneumonia, chronic obstructive pulmonary disease (COPD), or pleural effusion. To maximize accuracy, ensure the patient is seated or upright, as this position optimizes air distribution in the dependent lung segments.
Begin by palpating the mid-clavicular line, which serves as a reliable anatomical landmark. Place the stethoscope diaphragm lightly on the skin, starting at the 6th rib and moving downward to the 10th rib. Listen for symmetry in breath sounds between the left and right sides, noting any asymmetry, which may indicate localized pathology. In the axillary region, use the bell of the stethoscope to detect lower-pitched sounds, such as bronchial breathing or egophony, which can signal consolidation or fluid accumulation. For pediatric patients, use a smaller stethoscope head and apply gentle pressure to avoid discomfort.
A systematic approach is key to thorough assessment. Divide the lateral chest wall into quadrants, starting at the mid-clavicular line and moving laterally toward the axilla. Spend 5–10 seconds on each location, ensuring adequate time to detect subtle abnormalities. In elderly patients or those with obesity, increased subcutaneous tissue may muffle sounds, requiring firmer stethoscope application. Conversely, in children, lighter touch is essential to avoid altering respiratory patterns. Always compare findings to the opposite side for context.
Practical tips can enhance efficiency and accuracy. Warm the stethoscope to body temperature to prevent patient discomfort, which can alter breathing patterns. Instruct the patient to breathe deeply and evenly, but avoid coaching them to "take a deep breath," as this may introduce artifact. For patients with limited mobility, assess in their most comfortable position, adjusting your technique accordingly. Document findings using anatomical terms (e.g., "diminished breath sounds over the left mid-clavicular line at rib 8") to ensure clarity for other healthcare providers.
In conclusion, assessing the lateral chest wall from ribs 6-10 is a nuanced skill that combines anatomical knowledge with clinical acumen. By focusing on the mid-clavicular line and axillary regions, clinicians can detect early signs of respiratory pathology and guide targeted interventions. Mastery of this technique requires practice, attention to detail, and adaptability to patient-specific factors, making it an indispensable tool in the auscultation repertoire.
Clear Your Voice: Effective Tips to Eliminate Nasal Speech Patterns
You may want to see also
Explore related products






![]()
Anterior Axillary Line: Check lung sounds at 4th-5th intercostal spaces bilaterally
The anterior axillary line, a vertical plane running down the front of the chest, marks a critical area for auscultating lung sounds. Here, at the 4th and 5th intercostal spaces, the stethoscope encounters the transition zone between the upper and lower lobes of the lungs. This area is particularly sensitive to changes in airflow and can reveal valuable clues about respiratory health.
Unlike the dullness heard over the liver or the hyper-resonance of emphysema, normal lung sounds here should be clear and vesicular, resembling the rustling of leaves.
To effectively assess this area, position the patient in a seated or supine position. Identify the anterior axillary line by locating the nipple line and moving laterally until you reach the mid-axillary line. Then, count down to the 4th and 5th intercostal spaces, using the sternal angle as a reference point. Place the stethoscope diaphragm firmly but gently on the skin, ensuring a good seal to minimize ambient noise. Listen for symmetry between the left and right sides, noting any differences in intensity, pitch, or quality.
Remember, asymmetry doesn't always indicate pathology; factors like body habitus and underlying lung architecture can influence sound transmission.
This specific auscultation site is particularly useful for detecting conditions affecting the middle lung fields. Consolidation from pneumonia, for example, may produce bronchial breath sounds or crackles in this region. Pleural effusions can dampen sounds, while pneumothorax may lead to absent breath sounds on the affected side. Comparing findings with other auscultation sites helps localize the pathology and guide further diagnostic steps.
For instance, crackles heard only at the bases suggest dependent edema, while crackles extending to the mid-lung fields raise concern for more widespread disease.
Mastering auscultation at the anterior axillary line requires practice and a keen ear. Encourage patients to breathe deeply and slowly through their mouth, allowing for optimal sound detection. Be mindful of ambient noise and adjust your stethoscope position as needed. Remember, auscultation is just one piece of the diagnostic puzzle. Correlate your findings with the patient's history, physical exam, and other diagnostic tests for a comprehensive understanding of their respiratory status.
Understanding Amusia: How Tone-Deafness Alters Music Perception and Sound
You may want to see also
Explore related products






![]()
Mid-Scapular Region: Focus on T4-T8 vertebrae for posterior lung field sounds
The mid-scapular region, specifically the area overlying the T4-T8 vertebrae, is a critical location for auscultating posterior lung field sounds. This region corresponds to the lower lobes of the lungs, where conditions like pneumonia, atelectasis, or chronic obstructive pulmonary disease (COPD) often manifest audibly. Proper placement of the stethoscope here can reveal crackles, wheezes, or diminished breath sounds, providing essential clues to diagnose respiratory pathology. For accurate assessment, ensure the patient is seated upright or in a forward-leaning position to optimize sound transmission through the posterior lung fields.
Steps to Auscultate the Mid-Scapular Region:
- Patient Positioning: Have the patient sit upright or lean slightly forward with arms crossed to expose the back. This position flattens the scapulae, allowing better access to the T4-T8 area.
- Stethoscope Placement: Identify the T4-T8 vertebrae by palpating the spinous processes or estimating 2-3 finger widths below the scapulae. Place the stethoscope diaphragm firmly against the skin, avoiding clothing or gaps that could muffle sounds.
- Listening Technique: Begin at T4 and move downward to T8, pausing at each level to listen for at least 5-10 seconds per breath cycle. Compare findings bilaterally to detect asymmetry, which may indicate localized disease.
Cautions and Considerations:
Avoid applying excessive pressure with the stethoscope, as this can alter breath sounds. Be mindful of patient comfort, especially in elderly or frail individuals, where prolonged positioning may cause fatigue. Additionally, environmental noise can interfere with auscultation, so ensure a quiet setting. For pediatric patients, use a smaller stethoscope head and shorter auscultation times to maintain cooperation.
Practical Tips for Optimal Results:
Warm the stethoscope diaphragm before use to prevent patient discomfort, which can lead to muscle tension and altered breath sounds. Use a systematic approach, starting from the apex and moving downward, to ensure no area is overlooked. Document findings immediately, noting the location, quality, and intensity of abnormal sounds. For example, "Crackles heard at T6-T8 on the right side, worse on inspiration."
Clinical Relevance:
Focusing on the T4-T8 region is particularly valuable in diagnosing lower lobe conditions, such as right lower lobe pneumonia or left lower lobe atelectasis. This area is also crucial for monitoring patients with COPD, where expiratory wheezes or prolonged expiration may be prominent. By mastering auscultation here, clinicians can enhance diagnostic accuracy and tailor treatment plans effectively. Regular practice and familiarity with normal versus abnormal sounds in this region are key to proficiency.
Mastering the Long O Sound: Definition, Examples, and Pronunciation Tips
You may want to see also
Frequently asked questions
Lung sounds are best heard on the chest wall, specifically over the lung fields. Focus on the anterior (front), posterior (back), and lateral (sides) areas of the chest, as these regions provide the clearest auscultation of breath sounds.
Crackles are often heard at the lung bases, particularly in the posterior and lateral lower lobes. Wheezes are typically more prominent in the upper lobes and can be heard anteriorly or laterally. Always compare both sides of the chest for accurate assessment.
While lung sounds are primarily heard on the chest, faint breath sounds may occasionally be audible over the upper back or neck in certain conditions, such as severe emphysema. However, the chest remains the primary and most reliable area for auscultation.