Breath sounds, also known as lung or respiratory sounds, are crucial in assessing respiratory health and diagnosing various pulmonary conditions. To accurately listen to these sounds, healthcare professionals typically use a stethoscope, focusing on specific areas of the chest and back where the lungs are most accessible. The primary locations for auscultation include the anterior chest wall, posterior chest wall, and lateral chest wall, divided into distinct regions such as the trachea, lung fields, and areas over the bronchi. Proper placement of the stethoscope on these areas allows for the detection of normal breath sounds, such as vesicular and bronchovesicular sounds, as well as abnormal sounds like wheezes, crackles, or stridor, which can indicate underlying respiratory issues. Understanding where to take breath sounds is essential for effective patient evaluation and timely intervention.
| Characteristics | Values |
|---|---|
| Anterior Chest Wall | Upper, mid, and lower regions on the front of the chest. Key areas: 2nd rib (upper), 5th intercostal space (mid), and 7th-8th intercostal space (lower). |
| Posterior Chest Wall | Upper, mid, and lower regions on the back of the chest. Key areas: Scapular regions (upper), 7th-8th intercostal spaces (mid), and 9th-10th intercostal spaces (lower). |
| Lateral Chest Wall | Axillary regions (armpits) and mid-clavicular lines (sides of the chest). |
| Anatomic Landmarks | Sternum, clavicles, scapulae, and intercostal spaces. |
| Breath Sound Types | Vesicular (normal lung sounds), Bronchial (over trachea), Bronchovesicular (mid-lung fields). |
| Assessment Areas | Trachea (bronchial sounds), Lungs (vesicular sounds), and areas over main bronchi (bronchovesicular sounds). |
| Patient Position | Sitting or supine for optimal sound detection. |
| Equipment | Stethoscope for auscultation. |
| Common Pathologies Detected | Wheezing, crackles, rhonchi, and diminished/absent breath sounds. |
| Frequency of Sounds | Vesicular (low-pitched), Bronchial (high-pitched), Bronchovesicular (medium-pitched). |
| Duration of Sounds | Vesicular (longer during inspiration), Bronchial (equal inspiration/expiration). |
| Intensity | Vesicular (soft), Bronchial (loud), Bronchovesicular (moderate). |
Explore related products






What You'll Learn
- Anterior Chest Wall: Auscultate over the sternum, upper sternal border, and mid-clavicular lines for breath sounds
- Posterior Chest Wall: Listen along the scapulae, spine, and posterior axillary lines for lung sounds
- Lateral Chest Wall: Check mid-axillary lines, focusing on upper, mid, and lower zones for airflow
- Anterior Axillary Lines: Assess breath sounds in the anterior chest, near the armpit regions
- Tracheal Area: Auscultate over the trachea to detect normal or abnormal breath sounds centrally
![]()
Anterior Chest Wall: Auscultate over the sternum, upper sternal border, and mid-clavicular lines for breath sounds
The anterior chest wall is a critical area for auscultation, offering a direct pathway to assess lung health. By focusing on the sternum, upper sternal border, and mid-clavicular lines, clinicians can detect breath sounds that reveal vital information about airflow, lung tissue, and potential abnormalities. These anatomical landmarks serve as gateways to the upper lobes of the lungs, where conditions like pneumonia, chronic obstructive pulmonary disease (COPD), or asthma often manifest early. Proper technique here is essential, as subtle changes in sound quality or intensity can indicate localized issues before they become systemic.
To auscultate the anterior chest wall effectively, begin by positioning the patient in a seated or supine position, ensuring comfort and full chest expansion. Place the diaphragm of the stethoscope firmly over the sternum, listening for symmetrical breath sounds between the left and right sides. Move systematically to the upper sternal border, where diminished sounds may suggest conditions like pneumothorax or pleural effusion. Next, trace the mid-clavicular lines bilaterally, noting any asymmetry or adventitious sounds like wheezes, crackles, or stridor. Each location provides unique insights: the sternum reflects central airway function, while the mid-clavicular lines offer clues about peripheral lung health.
A practical tip for clinicians is to compare findings across these sites to identify patterns. For instance, unilateral crackles over the mid-clavicular line may indicate localized infection, while bilateral wheezing suggests widespread bronchoconstriction. Age-specific considerations are also crucial; children often present with higher-pitched breath sounds due to smaller airways, while elderly patients may exhibit diminished sounds from reduced lung elasticity. Consistency in technique, such as maintaining light pressure to avoid artifactual sounds, ensures accurate interpretation.
Caution must be exercised when interpreting findings, as anatomical variations or patient factors like obesity can obscure sounds. In such cases, repeating auscultation during deep inhalation or exhalation can enhance clarity. Additionally, correlating breath sounds with other clinical data, such as chest X-rays or spirometry results, strengthens diagnostic accuracy. The anterior chest wall, when auscultated meticulously, becomes a powerful tool for early detection and monitoring of respiratory conditions, bridging the gap between physical examination and advanced diagnostics.
Do Light Bulbs Make Sound? Uncovering the Truth Behind the Glow
You may want to see also
Explore related products






![]()
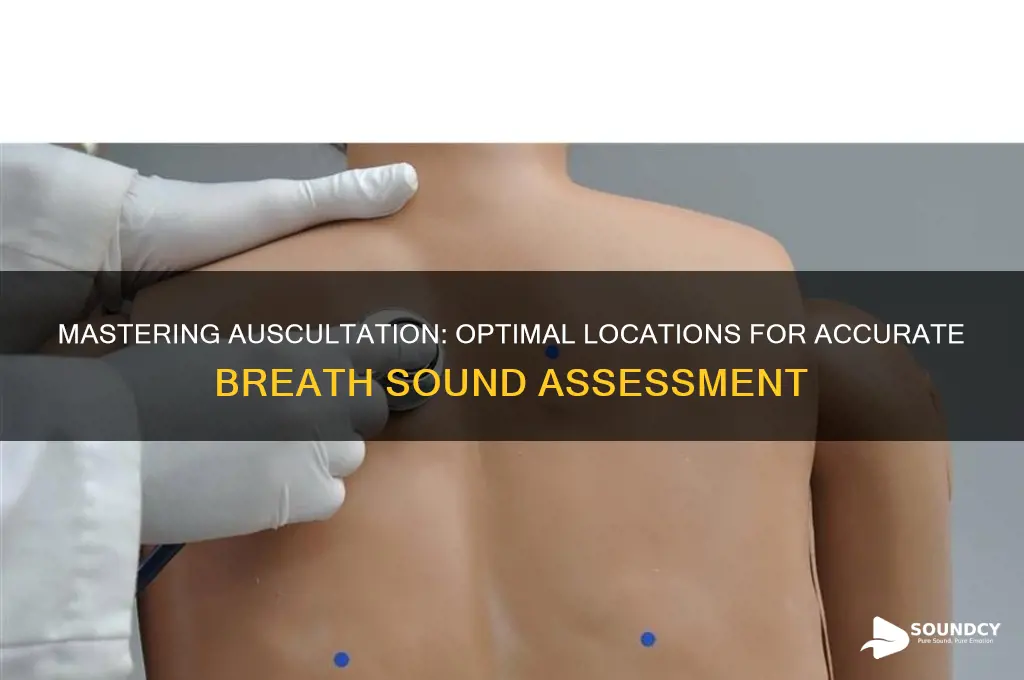
Posterior Chest Wall: Listen along the scapulae, spine, and posterior axillary lines for lung sounds
The posterior chest wall is a critical area for auscultation, offering a window into the lower lobes of the lungs, where conditions like pneumonia, atelectasis, or chronic obstructive pulmonary disease (COPD) often manifest. To effectively assess this region, begin by positioning the patient in a seated or upright posture, ensuring their arms are relaxed to expose the entire back. Use a stethoscope with a diaphragm for high-pitched sounds and a bell for low-pitched ones, alternating as needed. Start at the scapulae, moving downward along the spine, and finish along the posterior axillary lines bilaterally. This systematic approach ensures comprehensive coverage of the posterior lung fields.
Auscultation along the scapulae is particularly useful for detecting abnormalities in the apical segments of the lower lobes, as these areas are often overlooked during routine anterior exams. Place the stethoscope just medial to the scapula’s edge, listening for symmetry between the left and right sides. Wheezing, crackles, or diminished breath sounds in this area may indicate localized inflammation, fluid accumulation, or airway obstruction. For pediatric patients or individuals with scoliosis, adjust the stethoscope placement to account for anatomical variations, ensuring the diaphragm or bell is in firm contact with the skin.
The spine serves as a central landmark for assessing the posterior basal segments of the lower lobes. Move the stethoscope in a vertical line along the thoracic spine, pausing every 2–3 centimeters to listen for changes in breath sounds. In adults, this area is prone to consolidation in cases of pneumonia, especially in hospitalized or immunocompromised patients. For elderly individuals or those with chronic lung conditions, compare findings with previous auscultation records to track disease progression or response to treatment. Encourage patients to take slow, deep breaths during this process to enhance sound detection.
The posterior axillary lines are essential for evaluating the lateral basal segments of the lower lobes, a common site for pleural effusions or early-stage COPD changes. Begin at the sixth rib and move upward, maintaining consistent pressure on the stethoscope to avoid artifactual sounds. In children, this area may reveal signs of asthma or bronchiolitis, particularly during expiratory phases. For obese patients, use firmer pressure and consider using a larger stethoscope diaphragm to improve acoustic transmission through subcutaneous tissue. Document any asymmetry or abnormal sounds, as these may warrant further diagnostic imaging.
Mastering posterior chest wall auscultation requires practice and attention to detail. Combine findings with patient history, symptoms, and other physical exam observations for a holistic assessment. For healthcare providers, incorporating this technique into routine lung examinations can lead to earlier detection of respiratory conditions, particularly in populations at higher risk. Remember, the posterior chest wall is not just an extension of the anterior exam—it’s a distinct region with unique diagnostic value.
Knock, Knock: Spiritual Knocking Sounds
You may want to see also
Explore related products






![]()
Lateral Chest Wall: Check mid-axillary lines, focusing on upper, mid, and lower zones for airflow
The lateral chest wall, specifically the mid-axillary lines, offers a critical window into respiratory function, often revealing nuances missed in anterior auscultation. These lines, running vertically from the armpit to the lower rib cage, divide the chest into upper, mid, and lower zones, each corresponding to distinct lung segments. For instance, the upper zone aligns with the apices of the lungs, while the lower zone reflects the bases. This anatomical precision allows clinicians to pinpoint abnormalities like crackles in pneumonia or wheezing in asthma with greater accuracy.
To assess these zones effectively, position the patient upright or supine, ensuring relaxation to minimize muscle interference. Use a stethoscope with firm but gentle pressure to avoid artifactual sounds. Begin at the upper zone, noting symmetry with the contralateral side, then move systematically downward. In pediatric patients, particularly those under 5, this approach is invaluable due to their narrower chests and higher respiratory rates, which can mask subtle changes in airflow.
A comparative analysis of the mid-axillary zones can differentiate between localized and diffuse conditions. For example, unilateral crackles in the lower zone may suggest a lobar pneumonia, while bilateral wheezing across all zones could indicate bronchospasm. Adults with chronic obstructive pulmonary disease (COPD) often exhibit prolonged expiratory phases in these areas, a hallmark of airflow limitation. Pairing auscultation with percussion can further refine diagnosis, as dullness in a zone may indicate consolidation or effusion.
Practical tips include warming the stethoscope to avoid patient discomfort, which can alter breathing patterns. For obese patients, increased subcutaneous tissue may dampen sounds, requiring firmer pressure or extended listening time. Document findings with precision, noting the zone, character, and intensity of sounds (e.g., "moderate wheezing in mid-axillary lower zone"). This structured approach not only enhances diagnostic accuracy but also builds a baseline for monitoring progression or response to therapy.
In conclusion, the mid-axillary lines are not just anatomical landmarks but diagnostic tools that demand methodical exploration. By focusing on the upper, mid, and lower zones, clinicians can uncover vital clues about airflow dynamics, tailoring interventions to the patient’s specific needs. Mastery of this technique bridges the gap between theory and practice, transforming auscultation into a powerful clinical skill.
Dolphin Spotting in Puget Sound: Is It Possible?
You may want to see also
Explore related products






![]()
Anterior Axillary Lines: Assess breath sounds in the anterior chest, near the armpit regions
The anterior axillary lines, running vertically from the armpits to the chest, are critical landmarks for assessing breath sounds in the anterior chest. These lines divide the chest into regions that correspond to specific lung segments, making them essential for targeted auscultation. By focusing on these areas, healthcare providers can detect abnormalities like consolidation, obstruction, or reduced air entry, which may indicate conditions such as pneumonia, asthma, or pleural effusion. Understanding the anatomy and technique for auscultation in these regions is key to accurate respiratory assessment.
To assess breath sounds along the anterior axillary lines, begin by positioning the patient in a seated or supine position, ensuring comfort and proper exposure of the chest. Use a stethoscope with the diaphragm for adults and the bell for children, as higher-pitched sounds in pediatric patients require the more sensitive bell. Start at the second intercostal space and move downward, pausing at each space along the midclavicular and anterior axillary lines. Listen for symmetry between the left and right sides, noting any differences in intensity, pitch, or quality. For example, diminished sounds may suggest air trapping, while wheezing indicates airway narrowing.
One practical tip is to ask the patient to take slow, deep breaths during auscultation to amplify breath sounds and facilitate detection of abnormalities. In pediatric patients, particularly those under 5 years old, shorter attention spans may require quicker assessments or distraction techniques. For elderly patients or those with obesity, proper stethoscope placement and gentle pressure are crucial to avoid discomfort and ensure accurate readings. Always compare findings to the patient’s baseline, if known, as individual variations in breath sounds can occur.
A comparative analysis of breath sounds in the anterior axillary regions can reveal valuable insights. For instance, asymmetrical sounds may point to localized pathology, such as a pneumothorax or lobar collapse. In contrast, diffuse abnormalities across these lines could indicate systemic issues like chronic obstructive pulmonary disease (COPD) or acute respiratory distress syndrome (ARDS). By systematically evaluating these areas, clinicians can narrow down potential diagnoses and guide further diagnostic steps, such as imaging or pulmonary function tests.
In conclusion, mastering auscultation along the anterior axillary lines is a fundamental skill for respiratory assessment. It requires a blend of anatomical knowledge, technical precision, and clinical judgment. By focusing on these regions, healthcare providers can detect early signs of respiratory distress, monitor disease progression, and tailor interventions effectively. Whether in a hospital, clinic, or home setting, this targeted approach enhances diagnostic accuracy and patient outcomes.
The Mysterious Disappearance of the Sounds Program: What Went Wrong?
You may want to see also
Explore related products






![]()
Tracheal Area: Auscultate over the trachea to detect normal or abnormal breath sounds centrally
The trachea, a vital conduit for airflow, serves as a central hub for breath sounds. Auscultating over this area provides a direct line to the respiratory tract, offering insights into the integrity of the upper airways. Normal breath sounds here are typically soft and symmetric, reflecting unobstructed airflow. However, abnormalities such as stridor, wheezing, or rhonchi can signal conditions like tracheal stenosis, foreign body obstruction, or inflammation. This area is particularly critical in pediatric patients, where anatomical differences and higher susceptibility to foreign body aspiration necessitate careful evaluation.
To auscultate the tracheal area effectively, position the patient in a comfortable upright or supine position. Use the diaphragm of the stethoscope for high-pitched sounds and the bell for low-pitched ones, though the diaphragm is often sufficient for this region. Begin by placing the stethoscope directly over the trachea, midway between the cricoid cartilage and the sternal notch. Listen systematically, comparing both sides to identify asymmetry. In children, use a gentle touch and shorter duration to minimize discomfort, as their tracheas are more anterior and superficial.
Abnormal findings in the tracheal area demand immediate attention. Stridor, a high-pitched inspiratory sound, often indicates upper airway obstruction and requires urgent intervention. Wheezing, though more common in the bronchial regions, can also be detected centrally in cases of severe bronchospasm or tracheal inflammation. Rhonchi, low-pitched rattling sounds, may suggest mucus or secretions in the trachea. Documenting the characteristics of these sounds—pitch, timing (inspiratory vs. expiratory), and intensity—is crucial for accurate diagnosis and treatment planning.
Practical tips for tracheal auscultation include ensuring the patient is relaxed to avoid artifactual sounds from muscle tension. In infants and young children, auscultate during quiet breathing or sleep, as crying can distort findings. For obese patients, adjust the stethoscope pressure to ensure clear sound transmission without causing discomfort. Always correlate auscultatory findings with clinical context, such as a history of trauma, infection, or chronic respiratory conditions, to refine your differential diagnosis. Mastery of this technique enhances your ability to detect early signs of airway compromise, making it an indispensable skill in respiratory assessment.
Understanding External Diegetic Sound: Its Role and Impact in Filmmaking
You may want to see also
Frequently asked questions
The best locations are over the trachea (for central airway sounds) and bilaterally at the 2nd rib interspace (for upper lobe sounds) and 4th-5th rib interspaces (for lower lobe sounds).
Focus on the scapular regions (for lower lobe sounds) and along the 7th-10th rib interspaces (for basal lung sounds), ensuring to compare both sides for symmetry.
Yes, breath sounds can be heard over the suprasternal notch (above the clavicle), which is a normal area to assess central airway sounds. Abnormal sounds here may indicate upper airway issues.
In children, focus on the anterior chest at the 2nd and 4th rib interspaces, as their lungs are more anteriorly positioned compared to adults.