The phrase where is s4 herat sound appears to be a cryptic or incomplete query, blending elements that don't immediately align. S4 could refer to a medical heart sound, a classification in cardiology denoting a specific murmur or rhythm, while Herat is a city in Afghanistan, known for its rich history and cultural significance. The term sound might relate to auditory aspects, either medical or environmental. Without further context, the question remains ambiguous, potentially bridging medical terminology, geography, or even a coded message. Clarification on the intended meaning of s4 and its connection to Herat would be essential to provide a precise answer.
Explore related products






What You'll Learn
![]()
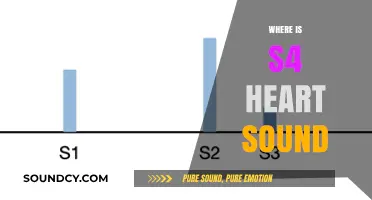
S4 Herat Sound Location
The S4 Herat sound is a critical diagnostic marker in cardiac auscultation, often indicating a specific pathology. To locate this sound effectively, begin by positioning the patient in a supine or left lateral decubitus position, as this optimizes acoustic transmission. Use a diaphragm stethoscope, placing it firmly over the mitral area, typically at the fifth intercostal space in the midclavicular line. Listen during late diastole, just before the S1 heart sound, as the S4 occurs during atrial contraction. This sound is low-pitched and best heard in states of increased left ventricular filling, such as hypertension or left ventricular hypertrophy.
Analyzing the S4 Herat sound requires distinguishing it from other low-pitched noises, such as gastrointestinal sounds or S3 gallops. The S4 is synchronous with the pulse and follows the S3 if both are present, creating a "ta-ta-ta" rhythm. Its presence often correlates with diastolic dysfunction, making it a valuable clue in diagnosing conditions like heart failure with preserved ejection fraction (HFpEF). However, its absence does not rule out pathology, as it may be masked by tachycardia or obesity.
To maximize detection, ensure the patient is relaxed and breathing normally, as deep breaths can accentuate the sound. In older adults or those with hypertension, the S4 is more prevalent, so clinicians should prioritize auscultation in these populations. If unsure, compare findings with other diagnostic tools like echocardiography, which can confirm diastolic dysfunction. Practicing on diverse patients sharpens auditory skills, as the S4’s subtlety requires a trained ear.
Instructing medical students or trainees involves emphasizing the systematic approach: position, timing, and context. For instance, teach them to correlate the S4 with risk factors like age, hypertension, or diabetes, which increase its likelihood. Encourage repeated auscultation in different scenarios to build familiarity. Caution against over-reliance on this single finding, as it is part of a broader clinical picture. Ultimately, mastering the S4 Herat sound location enhances diagnostic precision, particularly in identifying early-stage cardiac dysfunction.
Mastering the Pronunciation of 'Cuh': A Step-by-Step Guide to Sounding It Out
You may want to see also
Explore related products





![]()
Anatomical Position of S4 Sound
The S4 heart sound, often referred to as a fourth heart sound, is a low-pitched, late diastolic sound best heard at the cardiac apex with the patient in the left lateral decubitus position. This position optimizes auscultation by aligning the stethoscope with the anatomical location where the S4 sound is most prominent. The apex, situated at the fifth intercostal space in the midclavicular line, corresponds to the anatomical position of the left ventricle, the primary source of this sound. Proper patient positioning is critical, as the left lateral decubitus position reduces the dampening effect of lung tissue, allowing for clearer detection of the S4 sound.
Anatomically, the S4 sound arises from the abrupt deceleration of blood during the filling phase of the left ventricle, often indicative of a stiff or hypertrophied ventricle. This sound is typically heard just before the first heart sound (S1), marking the transition from late diastole to systole. Clinicians should instruct patients to exhale slowly and maintain a relaxed posture during auscultation to minimize artifacts and enhance sound detection. The use of a bell-type stethoscope, rather than a diaphragm, is recommended due to the low-frequency nature of the S4 sound, typically ranging between 20 to 30 Hz.
Instructive guidance for auscultation includes placing the stethoscope firmly but gently on the skin to ensure optimal acoustic transmission. Patients should be coached to breathe quietly and avoid coughing or movement, as these can obscure the subtle S4 sound. For older adults or individuals with obesity, additional pressure may be required to overcome tissue barriers and capture the sound accurately. It is also beneficial to compare findings between the apex and other locations, such as the aortic or pulmonic areas, to differentiate the S4 sound from other murmurs or artifacts.
Comparatively, the S4 sound differs from the S3 sound, which is also a low-pitched diastolic sound but occurs earlier in diastole and is associated with increased ventricular compliance. The S4, in contrast, signifies reduced compliance and is often a marker of left ventricular dysfunction. While the S3 is sometimes described as a benign finding in young individuals, the S4 is generally pathological, particularly in older adults or those with hypertension or ischemic heart disease. Recognizing this distinction is crucial for accurate diagnosis and subsequent management.
Practically, the anatomical position of the S4 sound serves as a diagnostic cornerstone for identifying underlying cardiac conditions. For instance, in patients with heart failure, the presence of an S4 sound often correlates with elevated filling pressures and reduced ejection fraction. Early detection can guide therapeutic interventions, such as diuretics or afterload reduction strategies. For healthcare providers, mastering the auscultation technique for the S4 sound is essential, as it provides valuable insights into ventricular function without reliance on advanced imaging modalities. Regular practice and familiarity with the anatomical landmarks ensure proficiency in identifying this critical cardiac marker.
Catalytic Converters: Muffling or Enhancing Your Exhaust's Roar?
You may want to see also
Explore related products






![]()
Conditions Causing Audible S4
The S4 heart sound, often described as a low-pitched "thump" following the typical "lub-dub" of the heartbeat, is a clinical sign that warrants attention. Its presence can indicate underlying cardiac conditions, particularly those affecting the left ventricle's compliance or filling dynamics. While not always pathological, an audible S4 is more common in specific scenarios, often serving as a red flag for further investigation.
Analyzing the Culprits: Several conditions can lead to an audible S4. One primary cause is left ventricular hypertrophy (LVH), where the heart muscle thickens due to increased workload, often seen in hypertension or aortic stenosis. This thickening reduces ventricular compliance, causing early and forceful contraction, thus producing the S4 sound. Ischemic heart disease is another culprit; reduced blood flow to the heart muscle can lead to similar ventricular stiffness, especially during episodes of angina or after a myocardial infarction. Interestingly, athletic heart syndrome can also present with an S4, as intense physical training may lead to physiological LVH, though this is generally benign and reversible.
Aging and Its Impact: Age-related changes in the heart can make the S4 more audible. In older adults, the left ventricle may become less compliant due to fibrosis or stiffening of the myocardial fibers, a condition known as diastolic dysfunction. This is particularly common in individuals over 65, especially those with long-standing hypertension or diabetes. For instance, a 70-year-old patient with uncontrolled hypertension is more likely to exhibit an S4 during auscultation, signaling the need for aggressive blood pressure management and further cardiac evaluation.
Practical Tips for Detection and Management: Clinicians should be vigilant during auscultation, especially in high-risk populations. The S4 is best heard at the cardiac apex with the patient in the left lateral decubitus position, using the bell of the stethoscope. If detected, further diagnostic steps such as echocardiography or BNP level assessment can help confirm the underlying cause. For patients with LVH, antihypertensive medications like ACE inhibitors or beta-blockers are often prescribed to reduce afterload and improve ventricular compliance. In cases of ischemia, addressing the underlying coronary artery disease through lifestyle changes, medications, or interventions like stenting may alleviate the S4.
Comparative Perspective: While the S4 is often associated with pathological conditions, it’s essential to differentiate it from benign findings. For example, a soft S4 in a young, asymptomatic athlete is likely physiological, whereas a loud, palpable S4 in a middle-aged individual with chest pain demands urgent attention. Understanding the context—age, symptoms, and risk factors—is crucial for accurate interpretation and management. By recognizing the conditions causing an audible S4, healthcare providers can tailor interventions to address the root cause, improving patient outcomes and preventing complications.
Do Rubber Bullets Make Sounds? Unveiling the Acoustic Truth Behind Less-Lethal Rounds
You may want to see also
Explore related products






![]()
Differentiating S4 from Other Sounds
The S4 heart sound, often referred to as a fourth heart sound, is a critical indicator of cardiac function, but its subtle nature makes it easy to confuse with other sounds. To differentiate it effectively, start by understanding its timing and quality. Unlike the more prominent S1 and S2 sounds, which mark the closure of heart valves, the S4 occurs in late diastole, just before the S1. This timing is crucial: it’s a low-pitched, brief sound, often described as a dull thud, that reflects atrial contraction forcing blood into a stiff ventricle. Recognizing this temporal and tonal signature is the first step in distinguishing it from other murmurs or sounds.
To isolate the S4, employ specific auscultation techniques. Use the bell of the stethoscope, which is more sensitive to low-frequency sounds, and focus on the cardiac apex, typically in the fifth left intercostal space. Ask the patient to exhale while you listen, as the S4 becomes more audible during expiration due to reduced intrathoracic pressure. Compare this with the S3 sound, which also occurs in early diastole but is associated with heart failure or volume overload. While both are low-pitched, the S3 is often described as a softer, distant “lub” and is not linked to atrial contraction, making the context of the patient’s condition essential for differentiation.
A common pitfall is mistaking the S4 for split heart sounds or innocent murmurs. For instance, a split S2 can mimic a diastolic sound but is actually a sign of delayed aortic valve closure. To avoid confusion, assess the patient’s age and risk factors: the S4 is more prevalent in older adults with hypertension or left ventricular hypertrophy. In children or young adults, an S4 is rare and warrants investigation for pathology. Always correlate auscultatory findings with diagnostic tools like echocardiography to confirm ventricular stiffness or dysfunction, as the S4 alone is not diagnostic but a red flag for further evaluation.
Practitioners should also consider the S4’s response to positional changes. Unlike pathological murmurs that may intensify with maneuvers like the Valsalva, the S4 often becomes more pronounced when the patient shifts to the left lateral decubitus position. This occurs because the heart is closer to the chest wall, enhancing sound transmission. Conversely, sitting upright may diminish the S4 in some cases, as blood redistributes away from the ventricles. Such nuances highlight the importance of dynamic auscultation in differentiating the S4 from static or positional sounds.
Finally, educate patients on the significance of an S4 finding. While it’s not an emergency, it signals underlying cardiac strain, often from chronic conditions like hypertension or aortic stenosis. Encourage lifestyle modifications—reducing sodium intake, managing blood pressure, and regular exercise—to mitigate ventricular stiffness. For high-risk individuals, pharmacotherapy such as ACE inhibitors or beta-blockers may be prescribed to reduce afterload and improve diastolic function. By combining clinical acumen with patient education, healthcare providers can transform the detection of an S4 from a diagnostic challenge into an opportunity for proactive cardiac care.
The Evolution of Sound in Movies
You may want to see also
Explore related products






![]()
Clinical Significance of S4 Herat Sound
The S4 heart sound, often referred to as an atrial gallop, is a low-pitched sound best heard at the cardiac apex with the patient in the left lateral decubitus position. Its presence is a critical clinical marker, signaling potential underlying cardiac dysfunction. Unlike the normal two-component heartbeat (S1 and S2), the S4 sound indicates increased atrial pressure or decreased ventricular compliance, often associated with conditions like left ventricular hypertrophy, hypertension, or aortic stenosis. Recognizing this sound during auscultation can prompt further diagnostic evaluation, making it a vital tool in early detection and management of cardiovascular diseases.
Clinically, the S4 sound is most commonly heard in patients with diastolic dysfunction, where the left ventricle becomes stiff and less compliant. This stiffness forces the atria to work harder to fill the ventricle, generating the extra sound. For instance, in hypertensive patients, chronic elevated blood pressure leads to left ventricular hypertrophy, a condition where the heart muscle thickens, reducing its ability to relax and fill properly. Auscultation in such cases may reveal an S4 sound, serving as an audible red flag for advanced cardiac remodeling. Early identification of this sound can guide treatment strategies, such as aggressive blood pressure control or the use of diuretics to reduce preload.
To effectively detect an S4 sound, clinicians should employ specific auscultation techniques. Use the bell of the stethoscope, which is more sensitive to low-frequency sounds, and ask the patient to exhale while listening, as this increases the intensity of the sound. The S4 occurs just before the first heart sound (S1), so careful timing is essential. If an S4 is suspected, further diagnostic tests like echocardiography or BNP (B-type natriuretic peptide) levels can confirm diastolic dysfunction or heart failure. This stepwise approach ensures that the clinical significance of the S4 sound is not overlooked.
The presence of an S4 sound carries prognostic implications, particularly in elderly patients or those with comorbidities. Studies show that individuals with an audible S4 have a higher risk of developing heart failure, atrial fibrillation, or cardiovascular mortality. For example, in a cohort of hypertensive patients, those with an S4 sound had a 2.5-fold increased risk of heart failure over five years compared to those without. This underscores the importance of regular cardiac auscultation in high-risk populations, such as patients with long-standing hypertension, diabetes, or a family history of cardiovascular disease.
Incorporating the S4 sound into clinical practice requires a nuanced understanding of its implications. While its presence is not diagnostic in isolation, it serves as a critical clue in the broader context of patient history and physical examination. For instance, in a 60-year-old patient with uncontrolled hypertension and an S4 sound, the clinician might prioritize initiating an ACE inhibitor or ARB to improve diastolic function and reduce afterload. By recognizing and acting on the clinical significance of the S4 sound, healthcare providers can intervene early, potentially altering the course of cardiovascular disease progression.
Master GarageBand's Signature Sound: Tips and Tricks for Authentic Production
You may want to see also
Frequently asked questions
S4 Herat sound, also known as a fourth heart sound, is an extra heart sound that occurs in late diastole, just before the normal "lub" sound (S1). It is often associated with a stiff or failing left ventricle.
S4 Herat sound is best heard at the cardiac apex, which is located in the fifth left intercostal space, mid-clavicular line. It may also be heard in other locations, but it is typically most prominent at the apex.
S4 Herat sound is commonly associated with conditions that cause left ventricular hypertrophy or stiffness, such as hypertension, aortic stenosis, or heart failure. It can also be heard in some normal individuals, particularly during exercise or in the elderly.