The S4 heart sound, often referred to as an atrial gallop, is a significant clinical finding that indicates increased pressure or volume within the left ventricle during late diastole. Typically heard just before the first heart sound (S1), it is best auscultated at the cardiac apex with the patient in the left lateral decubitus position. The presence of an S4 suggests underlying cardiac pathology, such as left ventricular hypertrophy, ischemia, or diastolic dysfunction, making it a critical diagnostic marker for clinicians evaluating heart function and identifying potential cardiovascular issues.
| Characteristics | Values |
|---|---|
| Location | Best heard at the cardiac apex (5th intercostal space, mid-clavicular line) |
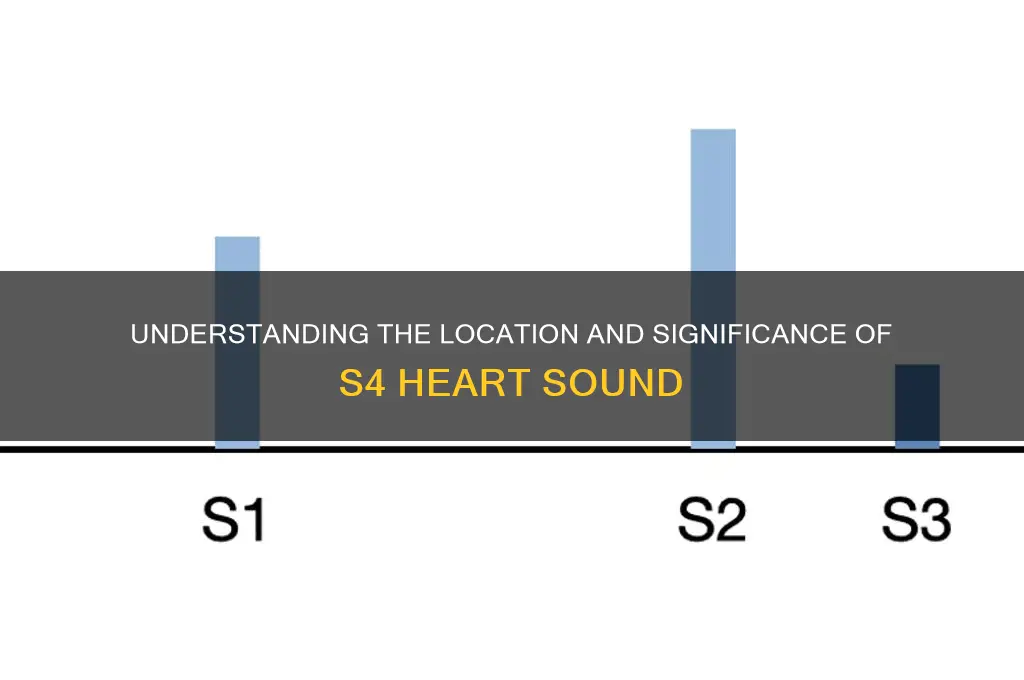
| Timing | Occurs just before the first heart sound (S1), during late diastole |
| Quality | Low-pitched, dull, and rumbling |
| Duration | Brief, often difficult to distinguish from S1 |
| Associated Conditions | Left ventricular hypertrophy, ischemia, infarction, or decreased compliance |
| Clinical Significance | Indicates increased filling pressure or decreased ventricular compliance |
| Comparison to S3 | S4 is pathological, while S3 can be physiological in some individuals |
| Auscultation Tips | Use a bell-shaped stethoscope and ask the patient to exhale during auscultation |
Explore related products






What You'll Learn
![]()
Anatomical Location of S4
The fourth heart sound, or S4, is a low-pitched sound best heard at the cardiac apex, typically with the patient in the left lateral decubitus position. This anatomical location is crucial for auscultation because S4 occurs during late diastole, just before the first heart sound (S1), and is associated with the atrioventricular valves closing as the atria contract. To maximize detection, use the bell of the stethoscope, which is more sensitive to lower frequencies, and ask the patient to hold their breath to minimize respiratory sounds. This sound is most audible in individuals with stiffened ventricles, such as those with hypertension or left ventricular hypertrophy, where the ventricle’s reduced compliance forces the atria to work harder to fill it.
Understanding the anatomical location of S4 is essential for distinguishing it from other heart sounds. Unlike S3, which is also a low-pitched sound but occurs in early diastole, S4 is a marker of late diastolic dysfunction. Clinicians should focus on the timing and quality of the sound: S4 is often described as a dull, rumbling noise that precedes S1, whereas S3 follows S2. Misidentifying S4 as S3 or vice versa can lead to incorrect diagnoses, such as confusing ventricular dilation with ventricular stiffness. Thus, precise auscultation at the apex, coupled with an awareness of the patient’s cardiac history, is critical for accurate interpretation.
For medical students and practitioners, mastering the detection of S4 requires practice and a systematic approach. Begin by positioning the patient in the left lateral decubitus position, which brings the heart closer to the chest wall, enhancing sound transmission. Place the stethoscope’s bell lightly on the apex, located in the fifth intercostal space at the midclavicular line. Instruct the patient to exhale and hold their breath to reduce interference from lung sounds. Listen carefully during late diastole, just before S1, for the characteristic low-pitched vibration of S4. If unsure, compare the sound to recorded examples or seek confirmation from a more experienced clinician.
The presence of S4 has significant clinical implications, particularly in older adults or those with cardiovascular risk factors. It often indicates reduced ventricular compliance, a common finding in conditions like systemic hypertension, aortic stenosis, or ischemic heart disease. For example, in a 60-year-old patient with long-standing hypertension, the detection of S4 at the apex could signal left ventricular hypertrophy and increased cardiovascular risk. In such cases, further evaluation with echocardiography is warranted to assess ventricular function and guide treatment, which may include antihypertensive medications or lifestyle modifications to reduce cardiac strain.
Finally, while auscultation remains a cornerstone of cardiovascular examination, the anatomical location of S4 highlights the importance of integrating clinical findings with diagnostic tools. The apex, as the primary site for detecting S4, serves as a window into ventricular health. However, reliance on auscultation alone can be limiting, especially in patients with obesity or lung disease, where heart sounds may be muffled. Combining auscultation with imaging studies, such as echocardiography or cardiac MRI, provides a more comprehensive assessment of diastolic function. By focusing on the apex during examination and understanding its role in S4 detection, clinicians can better identify and manage conditions associated with ventricular stiffness, ultimately improving patient outcomes.
Sound's Straight-Line Journey: Myth or Reality?
You may want to see also
Explore related products





![]()
Conditions Causing S4 Heart Sound
The S4 heart sound, often described as a late diastolic "atrial gallop," is a clinical marker of significant cardiac pathology. It occurs just before the first heart sound (S1) and is best heard at the cardiac apex with the patient in the left lateral decubitus position. While its presence is not diagnostic of a single condition, it strongly suggests underlying left ventricular dysfunction or increased filling pressures. Understanding the conditions that cause an S4 is critical for accurate diagnosis and targeted intervention.
Conditions Linked to S4: A Pathophysiological Perspective
An S4 arises when the left ventricle becomes stiff or hypertrophied, impairing its ability to relax during diastole. This forces the atria to contract with greater force against increased resistance, producing the audible fourth sound. Hypertensive heart disease is a primary culprit, as chronic hypertension leads to left ventricular hypertrophy (LVH), a common substrate for S4. Similarly, aortic stenosis, whether congenital or degenerative, causes pressure overload on the left ventricle, resulting in concentric hypertrophy and diastolic dysfunction. In both cases, the S4 reflects the ventricle’s struggle to accommodate blood during filling.
Ischemia and Infiltration: Less Obvious Causes
Beyond structural abnormalities, ischemic heart disease can also provoke an S4. Myocardial infarction, particularly when involving the left ventricle, may lead to scar tissue formation and reduced compliance, creating conditions for an S4. Less commonly, infiltrative disorders like cardiac amyloidosis or Fabry disease cause ventricular stiffening due to abnormal protein deposition, manifesting as an S4 despite normal wall thickness. These conditions highlight the importance of considering infiltrative cardiomyopathies in patients with an S4 and no overt hypertrophy.
Practical Tips for Clinicians
When encountering an S4, prioritize assessing blood pressure and cardiac biomarkers to rule out hypertension or ischemia. Echocardiography is essential to evaluate left ventricular thickness, ejection fraction, and valve function. In hypertensive patients, aim for a blood pressure target of <130/80 mmHg, as per ACC/AHA guidelines, to mitigate LVH progression. For aortic stenosis, consider valve replacement if the gradient exceeds 40 mmHg or symptoms develop. Infiltrative diseases may require advanced imaging, such as cardiac MRI with gadolinium, for definitive diagnosis.
Takeaway: The S4 as a Red Flag
The S4 is not merely an auscultatory curiosity but a red flag for advanced cardiac disease. Its presence demands a systematic evaluation of hemodynamic stressors, structural abnormalities, and infiltrative processes. Early recognition and intervention can halt disease progression, emphasizing the need for clinicians to listen carefully and act decisively when this sound is detected.
Effective Strategies to Manage Sound Sensitivity and Enhance Daily Comfort
You may want to see also
Explore related products






![]()
Differentiating S4 from Other Sounds
The S4 heart sound, often described as a late diastolic "atrial kick," is a subtle yet significant marker of cardiac function. Its presence can indicate conditions such as left ventricular hypertrophy or reduced compliance, making accurate identification crucial. Differentiating S4 from other heart sounds requires a keen ear and an understanding of its unique characteristics. Unlike S1 and S2, which are loud and easily audible, S4 is soft and best heard at the cardiac apex with the patient in the left lateral decubitus position. Using a diaphragm rather than a bell on the stethoscope can enhance detection, as S4 is a low-pitched sound.
One common challenge is distinguishing S4 from S3, another diastolic sound. While both occur during diastole, their timing and quality differ. S3 is an early diastolic sound, often described as a "ventricular gallop," and is heard shortly after S2. In contrast, S4 occurs late in diastole, just before S1, and is associated with atrial contraction. A useful mnemonic is "S3 is 'here' (early), S4 is 'there' (late)." Additionally, S3 is typically heard in children and young adults as a benign finding, whereas S4 is more often pathological, particularly in older adults with hypertension or cardiac disease.
Another point of confusion is mistaking S4 for split heart sounds or murmurs. Split S1 or S2 can sometimes mimic diastolic sounds, but these splits are related to electrical conduction delays, not mechanical events like S4. Murmurs, on the other hand, are continuous sounds caused by turbulent blood flow and lack the distinct timing of S4. To avoid misdiagnosis, focus on the precise timing of the sound relative to S1 and S2, and consider the patient’s clinical context. For example, a patient with long-standing hypertension is more likely to have an S4 than a split sound.
Practical tips for differentiating S4 include having the patient exhale during auscultation, as this can accentuate low-pitched sounds. If uncertainty persists, echocardiography can confirm the presence of S4 by visualizing late diastolic atrial contraction. For clinicians, mastering this distinction is essential, as S4 often signals increased afterload or decreased ventricular compliance, warranting further evaluation and management. By combining careful auscultation with clinical correlation, healthcare providers can confidently identify S4 and its implications for patient care.
Understanding Sound Symbol Association: The Link Between Speech and Writing
You may want to see also
Explore related products






![]()
Clinical Significance of S4
The S4 heart sound, often described as a late diastolic "atrial kick," is a subtle yet clinically significant marker of cardiac function. It occurs just before the first heart sound (S1) and is best heard at the cardiac apex with the patient in the left lateral decubitus position. While a soft S4 can be a normal finding in children and well-trained athletes, its presence in adults often signals increased left ventricular stiffness or volume overload. This sound is generated by the forceful contraction of the atria against a non-compliant ventricle, a phenomenon that warrants careful clinical evaluation.
From an analytical perspective, the presence of an S4 heart sound is a red flag for underlying cardiac pathology. It is commonly associated with conditions such as hypertension, left ventricular hypertrophy, and ischemic heart disease. For instance, in hypertensive patients, chronic pressure overload leads to ventricular remodeling, reducing chamber compliance and promoting the development of an S4. Similarly, in aortic stenosis, the increased afterload forces the atria to work harder, producing the audible S4. Recognizing this sound during auscultation can prompt further diagnostic workup, including echocardiography, to assess ventricular function and structure.
Clinicians should approach the detection of an S4 with a systematic strategy. Begin by ensuring optimal auscultation conditions: use a high-quality stethoscope, minimize ambient noise, and position the patient correctly. Focus on the timing of the sound, as an S4 occurs just before S1, distinguishing it from an S3 (early diastolic gallop). If an S4 is identified, correlate it with the patient’s history and risk factors. For example, in a middle-aged patient with untreated hypertension, an S4 may indicate advanced left ventricular dysfunction, necessitating aggressive blood pressure management and referral to cardiology.
Persuasively, the clinical significance of an S4 lies in its predictive value for adverse cardiovascular outcomes. Studies have shown that patients with an audible S4 are at increased risk for heart failure, arrhythmias, and mortality. This underscores the importance of early intervention. Lifestyle modifications, such as sodium restriction and regular exercise, can improve ventricular compliance and potentially reduce the prominence of an S4. Pharmacotherapy, including angiotensin-converting enzyme (ACE) inhibitors or beta-blockers, may also be beneficial in managing the underlying conditions contributing to its presence.
In comparison to other heart sounds, the S4 is unique in its association with diastolic dysfunction, a condition often overlooked in routine clinical practice. While S1 and S2 reflect systolic events, and S3 may indicate volume overload, the S4 specifically highlights impaired ventricular relaxation or increased stiffness. This distinction makes it a valuable tool for differentiating between systolic and diastolic heart failure, particularly in elderly patients where diastolic dysfunction is prevalent. By integrating S4 auscultation into routine cardiac exams, clinicians can enhance their diagnostic accuracy and tailor treatment strategies accordingly.
Is Sound a Noun? Exploring the Linguistic Nature of Auditory Phenomena
You may want to see also
Explore related products






![]()
Diagnostic Techniques for Detecting S4
The S4 heart sound, often described as a late diastolic "atrial gallop," is a subtle yet significant marker of cardiac dysfunction. Detecting it requires precision and the right diagnostic techniques. One of the most effective methods is auscultation with a high-quality stethoscope, ideally in a quiet room to minimize ambient noise. The S4 sound is best heard at the cardiac apex, typically in the left fifth intercostal space at the midclavicular line, during late diastole. Patients should be in the left lateral decubitus position, as this enhances sound transmission. Clinicians must listen carefully, as the S4 is often low-pitched and brief, easily overshadowed by louder heart sounds.
While auscultation remains the gold standard, echocardiography provides a more definitive diagnosis by visualizing cardiac structures and function. A transthoracic echocardiogram (TTE) can reveal left ventricular hypertrophy or reduced compliance, conditions often associated with an S4. For older adults or patients with obesity, where auscultation may be challenging, TTE is particularly valuable. Doppler echocardiography can further assess diastolic function, identifying abnormalities in mitral inflow patterns that correlate with the presence of an S4. This imaging technique is especially useful in patients over 60, as age-related stiffening of the ventricle increases the likelihood of an S4.
For patients with suspected heart failure or hypertension, electrocardiography (ECG) can complement auscultation by identifying underlying causes of an S4. Left ventricular hypertrophy, often seen on ECG as increased QRS voltage, is a common culprit. However, ECG alone cannot confirm an S4; it serves as a supportive tool. Combining ECG findings with auscultation and echocardiography provides a comprehensive diagnostic approach, particularly in middle-aged and older adults with cardiovascular risk factors.
In cases where non-invasive methods are inconclusive, cardiac catheterization may be necessary. This invasive procedure measures intracardiac pressures directly, offering insights into diastolic dysfunction that may produce an S4. While not routinely used for S4 detection, it is reserved for complex cases, such as patients with unexplained heart failure or discrepant findings from other tests. For example, a left ventricular end-diastolic pressure (LVEDP) above 20 mmHg strongly suggests elevated filling pressures, a common cause of S4.
Finally, patient positioning and breathing techniques can enhance S4 detection during auscultation. Instructing the patient to hold their breath in expiration or perform the Valsalva maneuver can accentuate the sound. For pediatric patients or younger adults, where S4 is less common, these techniques may help differentiate it from other diastolic murmurs. Practically, clinicians should spend at least 30 seconds listening at the apex, ensuring they capture the late diastolic phase of the cardiac cycle. Mastery of these techniques ensures accurate diagnosis, guiding timely intervention for conditions like hypertensive heart disease or ischemic cardiomyopathy.
Exploring the Soothing and Wild Symphony of Wind's Unique Sounds
You may want to see also
Frequently asked questions
The S4 heart sound, also known as the atrial gallop, is best heard at the cardiac apex (5th left intercostal space, midclavicular line) with the patient in the left lateral decubitus position.
The S4 heart sound is caused by the forceful contraction of the atria against a stiff or non-compliant ventricle, often seen in conditions like left ventricular hypertrophy, hypertension, or heart failure.
The S4 heart sound is a low-pitched sound occurring just before the first heart sound (S1), creating a "Tennessee" gallop rhythm (S1-S4-S2). It is distinguished from S3 by its timing and association with atrial contraction.























