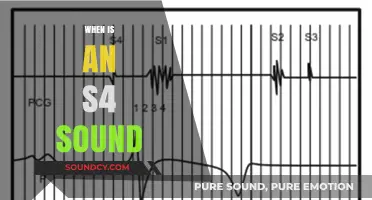
The lubb sound, a fundamental component of the cardiac cycle, refers to the characteristic lub-dub noise produced by the heart as it beats. This sound is generated by the closing of the heart valves, specifically the atrioventricular (AV) valves (mitral and tricuspid) creating the first lub, and the semilunar valves (aortic and pulmonary) producing the second dub. Understanding when the lubb sound is heard is crucial in assessing heart function and diagnosing potential cardiac issues. It is typically audible during auscultation with a stethoscope, providing valuable insights into the timing and efficiency of the heart's contractions and relaxations.
| Characteristics | Values |
|---|---|
| Sound | Lubb (dull, low-pitched) |
| Represents | Closure of the atrioventricular (AV) valves (mitral and tricuspid) |
| Occurs During | Early ventricular systole |
| Timing | Shortly after the first heart sound (S1) |
| Associated With | Blood rushing from the atria into the ventricles |
| Clinical Significance | Normal finding in a healthy heart |
Explore related products






What You'll Learn
![]()
Timing of Lubb Sound
The lubb sound, a component of the heart’s auditory cycle, occurs during systole, specifically when the mitral and tricuspid valves close. This event marks the beginning of ventricular contraction, a critical phase in the cardiac cycle. Understanding the timing of this sound is essential for clinicians and medical students, as it provides insights into heart function and potential abnormalities. For instance, a delayed lubb sound might indicate issues with valve closure or electrical conduction within the heart.
Analyzing the timing of the lubb sound requires a systematic approach. Start by auscultating the heart with a stethoscope, focusing on the mitral area (fifth intercostal space, midclavicular line). The lubb sound corresponds to the first heart sound (S1), which is best heard during this phase. Compare the timing of S1 with the carotid pulse to ensure synchronization. If the lubb sound is asynchronous with the pulse, further investigation is warranted. For example, a split S1 may suggest atrial enlargement or bundle branch block, conditions that alter the normal sequence of valve closures.
Instructing patients to hold their breath briefly during auscultation can enhance the clarity of the lubb sound. This technique minimizes respiratory artifacts and allows for better detection of subtle abnormalities. For pediatric patients, particularly those under 10 years old, the lubb sound may be softer and higher-pitched due to smaller valve structures. Clinicians should adjust their expectations and techniques accordingly, using a smaller stethoscope bell and applying lighter pressure.
Comparatively, the lubb sound contrasts with the dubb sound (S2), which occurs during diastole when the aortic and pulmonary valves close. While the lubb sound signifies the start of ventricular ejection, the dubb sound marks the end. This distinction is crucial for diagnosing conditions like aortic stenosis or mitral regurgitation, where the timing and quality of these sounds are altered. For instance, a widened splitting of S2 may indicate delayed aortic valve closure, a hallmark of aortic stenosis.
Practically, mastering the timing of the lubb sound involves repeated practice and correlation with other diagnostic tools. For medical students, recording auscultation sessions and reviewing them alongside ECG tracings can reinforce understanding. For clinicians, integrating this knowledge into routine physical exams can improve diagnostic accuracy. Remember, the lubb sound is not just a noise—it’s a window into the heart’s mechanical performance, offering clues to underlying pathology when interpreted correctly.
Unveiling the Grunts, Squeals, and Roars: What Sound Do Boars Make?
You may want to see also
Explore related products






![]()
Conditions Amplifying Lubb Sound
The lubb sound, a component of the heart’s dual-tone beat, becomes more pronounced under specific physiological and pathological conditions. Understanding these amplifying factors is crucial for both medical professionals and individuals monitoring cardiac health. Among the primary conditions that intensify the lubb sound is valvular dysfunction, particularly mitral valve prolapse or stenosis. When the mitral valve fails to close properly, the lubb (S1) sound, which corresponds to mitral valve closure, becomes louder and more distinct. This is often accompanied by a murmur, but the lubb itself stands out due to the increased force of valve impact.
Another significant amplifier of the lubb sound is increased ventricular contractility, often seen in conditions like hypertension or athletic heart syndrome. In these cases, the heart muscle contracts with greater force, causing the mitral and tricuspid valves to close more abruptly. This results in a sharper, louder lubb sound. For instance, athletes may exhibit a more pronounced lubb due to their hearts’ heightened efficiency, while hypertensive patients experience it as a consequence of the heart working harder against elevated blood pressure. Monitoring this sound can provide insights into the heart’s adaptive or pathological changes.
Chest wall characteristics also play a role in amplifying the lubb sound. Thin individuals, children, or those with reduced subcutaneous fat tend to transmit heart sounds more clearly, making the lubb sound more audible. Conversely, obesity or excessive chest wall tissue can muffle the sound, but in cases of fluid accumulation (e.g., pericardial effusion), the lubb may paradoxically become louder due to altered acoustic transmission. Clinicians often consider body habitus when interpreting heart sounds, as it directly influences their perception.
Finally, positional changes can temporarily amplify the lubb sound. For example, moving from a supine to a standing position increases venous return to the heart, leading to a more forceful contraction and a louder lubb. Similarly, the left lateral decubitus position, often used in auscultation, enhances sound transmission and can make the lubb more distinct. Patients and practitioners alike can leverage these positional adjustments to better detect and assess cardiac sounds during routine examinations.
In summary, the lubb sound is amplified by valvular dysfunction, increased ventricular contractility, chest wall characteristics, and positional changes. Recognizing these conditions not only aids in diagnosing cardiac issues but also highlights the dynamic nature of heart sounds in response to physiological and environmental factors. Practical tips, such as adjusting patient position or considering body habitus, can significantly improve auscultation accuracy.
Understanding the Distinctive Sound of a Fire Alarm: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Differences Between Lubb and Dub
The lubb and dub sounds are the iconic duo of heart auscultation, yet they differ fundamentally in origin and clinical significance. The lubb corresponds to the closure of the atrioventricular (AV) valves (mitral and tricuspid), marking the beginning of systole, while the dub represents the closure of the semilunar valves (aortic and pulmonary), signaling the end of systole. This distinction is critical for diagnosing valve disorders: a delayed or split lubb may indicate AV valve dysfunction, whereas a softened or absent dub could suggest semilunar valve issues.
To differentiate these sounds practically, consider their timing and quality. The lubb is typically lower-pitched and longer, occurring at the start of the cardiac cycle, while the dub is higher-pitched and shorter, closing the cycle. For example, in a patient with aortic stenosis, the dub may be diminished or delayed, whereas mitral regurgitation often presents with a louder, snapping lubb. Using a diaphragm stethoscope for lubb and a bell for dub can enhance detection, especially in pediatric patients or those with faint heart sounds.
Clinicians must also account for physiological variations. In children or athletes, the lubb and dub may be softer due to thinner valves or faster heart rates. Conversely, in elderly patients, calcified valves can produce louder, sharper sounds. A key takeaway is that the lubb-dub sequence should be consistent; any irregularity warrants further investigation, such as an echocardiogram or ECG.
For self-assessment, practice auscultation on diverse patients, focusing on the transition between lubb and dub. Record findings systematically: note pitch, duration, and any murmurs. For instance, a harsh, late-peaking dub could indicate aortic stenosis, while a blowing murmur between lubb and dub might suggest mitral regurgitation. Mastery of these nuances transforms auscultation from a routine task into a powerful diagnostic tool.
Exploring the Unique Interdental Sound of 'F' in Phonetics
You may want to see also
Explore related products






![]()
Lubb Sound in Heart Valves
The lubb sound, often described as the first heart sound (S1), is a critical auditory cue in cardiac auscultation. It occurs at the beginning of systole, marking the closure of the mitral and tricuspid valves. This sound is best heard at the apex of the heart, typically in the fifth intercostal space in the midclavicular line. Clinicians rely on the lubb sound to assess the timing and quality of valve function, as deviations can indicate conditions like mitral stenosis or tricuspid regurgitation. Understanding its characteristics—low-pitched, dull, and prolonged—is essential for accurate diagnosis.
To effectively auscultate the lubb sound, position the patient in the left lateral decubitus position, which optimizes sound transmission. Use the bell of the stethoscope for low-pitched sounds and apply light pressure to the chest wall. Begin at the apex and systematically move to other auscultation sites, comparing the intensity and quality of S1 across locations. For pediatric patients, particularly those under 12 years old, the lubb sound may be softer and higher-pitched due to faster heart rates and smaller valve structures. Always correlate auscultatory findings with other diagnostic tools like echocardiography for comprehensive evaluation.
A comparative analysis of the lubb sound across age groups reveals distinct patterns. In neonates and infants, S1 is often softer and less distinct due to the rapid heart rate and less calcified valves. By adolescence, the sound becomes more pronounced and resembles that of adults. In the elderly, calcification of the mitral and tricuspid valves can cause the lubb sound to become louder and more snapping. Recognizing these age-related variations is crucial for avoiding misdiagnosis, especially in differentiating physiological changes from pathological conditions like mitral valve prolapse or degenerative valve disease.
For healthcare providers, teaching patients about the lubb sound can empower them to monitor their cardiac health. Encourage patients to report any changes in the rhythm or quality of their heartbeat, particularly if they notice a new murmur or an unusually loud sound. Practical tips include maintaining a healthy lifestyle to prevent valve disease, such as managing blood pressure, avoiding smoking, and seeking prompt treatment for infections like endocarditis. For high-risk individuals, such as those with a history of rheumatic fever, annual cardiac evaluations are recommended to detect early signs of valve dysfunction.
In conclusion, the lubb sound is a cornerstone of cardiac auscultation, offering valuable insights into heart valve function. By mastering its auscultation techniques, understanding age-related variations, and educating patients, clinicians can enhance diagnostic accuracy and promote proactive cardiac care. Whether in a routine checkup or a specialized evaluation, the lubb sound remains an indispensable tool in the assessment of cardiovascular health.
Effective DIY Sound Trap Construction: A Step-by-Step Guide for Beginners
You may want to see also
Explore related products





![]()
Clinical Significance of Lubb Sound
The lubb sound, the first heart sound (S1), is a critical auscultatory marker of mitral and tricuspid valve closure. Clinically, its timing, intensity, and quality provide insights into cardiac function and pathology. For instance, a delayed lubb sound may indicate left bundle branch block or prolonged left ventricular emptying, while a split lubb suggests right or left ventricular volume overload. Recognizing these variations is essential for diagnosing conditions like mitral stenosis, where the lubb is often loud and snapping, or myocardial infarction, where it may be muffled due to papillary muscle dysfunction.
Instructively, healthcare providers should assess the lubb sound in conjunction with patient history and other physical exam findings. For example, in pediatric patients, a prominent lubb in the absence of pathology is common due to increased heart rate and thinner chest walls. In contrast, elderly patients may exhibit a softer lubb due to calcified valves or reduced ventricular compliance. Auscultation should be performed systematically, starting at the mitral area (fifth intercostal space, midclavicular line) and moving to the tricuspid area (left sternal border, third intercostal space). Using a bell chest piece for low-frequency sounds enhances detection of abnormalities.
Persuasively, the lubb sound’s clinical significance extends beyond diagnosis to monitoring treatment efficacy. For patients on inotropic therapy, such as milrinone (0.375–0.75 mcg/kg/min), an improved lubb intensity and quality may indicate enhanced myocardial contractility. Similarly, in patients with heart failure, the lubb sound can reflect response to angiotensin-converting enzyme inhibitors (e.g., lisinopril 5–40 mg/day) or beta-blockers (e.g., metoprolol succinate 25–200 mg/day). Early detection of changes in the lubb sound can prompt timely adjustments in therapy, potentially improving outcomes and reducing hospitalizations.
Comparatively, the lubb sound’s utility contrasts with that of the dubb (S2), which reflects aortic and pulmonic valve closure. While the dubb is more sensitive to pulmonary hypertension or aortic stenosis, the lubb is a direct indicator of left and right ventricular performance. For example, in athletes, a physiologically split lubb may mimic pathology, whereas in patients with atrial fibrillation, an irregularly irregular lubb rhythm is diagnostic. Understanding these distinctions ensures accurate interpretation and avoids misdiagnosis, particularly in complex cases like patent ductus arteriosus, where both S1 and S2 may be altered.
Descriptively, the lubb sound’s characteristics—pitch, duration, and loudness—offer a window into cardiac mechanics. A high-pitched lubb may suggest mitral valve prolapse, while a prolonged lubb can indicate left ventricular dilation. In emergency settings, a faint or absent lubb raises concern for cardiac tamponade or severe left ventricular failure. Practical tips include using the diaphragm chest piece for high-frequency sounds and asking the patient to exhale during auscultation to amplify S1. By mastering these nuances, clinicians can transform the lubb sound from a routine finding into a powerful diagnostic and prognostic tool.
Understanding Larynx Mechanics: How Vocal Folds Create Human Sound
You may want to see also
Frequently asked questions
The lubb sound refers to the first heart sound (S1), which is produced by the closure of the atrioventricular valves (mitral and tricuspid valves) at the beginning of ventricular contraction.
The lubb sound is heard at the start of systole, marking the beginning of ventricular contraction and the closure of the atrioventricular valves.
The lubb sound (S1) is lower in pitch and longer in duration compared to the dub sound (S2), which is caused by the closure of the semilunar valves (aortic and pulmonary valves) at the start of diastole.
Yes, an abnormal lubb sound (S1) can indicate issues such as mitral stenosis, tricuspid valve problems, or other conditions affecting the atrioventricular valves.
The lubb sound is best heard at the mitral area (5th intercostal space, mid-clavicular line) and the tricuspid area (left sternal border) using a stethoscope.