The S4 heart sound, often referred to as a fourth heart sound, is an abnormal cardiac finding that occurs during late diastole, just before the normal S1 sound. It is typically heard in individuals with certain cardiac conditions, such as left ventricular dysfunction or heart failure, where the left ventricle becomes stiff and less compliant. This additional sound is a result of the forceful atrial contraction needed to push blood into a less compliant ventricle, creating a low-pitched, rumbling noise best heard at the cardiac apex with a stethoscope. Recognizing an S4 sound is crucial for clinicians as it can indicate underlying cardiovascular issues and guide further diagnostic and therapeutic interventions.
| Characteristics | Values |
|---|---|
| Timing | Occurs during late diastole, just before the S1 heart sound (first heart sound). |
| Cause | Stiffening of the ventricle (often due to hypertrophy or ischemia) leading to a stiffened ventricle that generates an audible vibration as blood rushes in. |
| Associated Conditions | Hypertrophic cardiomyopathy, Left ventricular hypertrophy, Ischemic heart disease, Aortic stenosis, Hypertension |
| Quality | Low-pitched, rumbling, and best heard with the bell of the stethoscope (duller side). |
| Location | Apical area (5th intercostal space, mid-clavicular line) |
| Intensity | Often grade 3/6 or louder |
| Significance | Indicates ventricular stiffness and potential underlying cardiac pathology. |
Explore related products






What You'll Learn
- Normal S4 Causes: Athletic hearts, anemia, or hypertension can cause benign S4 sounds in certain individuals
- Pathological S4 Causes: Conditions like left ventricular hypertrophy or ischemia often produce abnormal S4 sounds
- S4 Timing: Occurs during late diastole, just before the first heart sound (S1)
- S4 Characteristics: Low-pitched, rumbling sound, best heard at the apex with a bell
- Diagnosing S4: Requires careful auscultation, often confirmed with echocardiography or other imaging studies
![]()
Normal S4 Causes: Athletic hearts, anemia, or hypertension can cause benign S4 sounds in certain individuals
The S4 heart sound, often described as a late diastolic "thump," is typically associated with pathological conditions like left ventricular hypertrophy or ischemia. However, it’s crucial to recognize that not all S4 sounds signal disease. In certain individuals, this sound can arise from benign, physiological adaptations or underlying conditions that don’t require intervention. Understanding these normal causes—athletic hearts, anemia, and hypertension—is essential for accurate diagnosis and avoiding unnecessary alarm.
Consider the athlete’s heart, a classic example of physiological adaptation. Prolonged endurance training leads to left ventricular remodeling, increasing chamber stiffness and enhancing filling pressures during diastole. This can produce an S4 sound, particularly in young, highly conditioned athletes. For instance, a 25-year-old marathon runner with a resting heart rate of 45 bpm and a left ventricular wall thickness of 12 mm (measured via echocardiography) might exhibit this sound without any functional impairment. The takeaway? Context matters. An S4 in an athlete, especially when asymptomatic and accompanied by normal ejection fraction (>55%), is often benign and requires no treatment beyond routine monitoring.
Anemia, another cause of benign S4 sounds, operates through a different mechanism. In anemic individuals, reduced hemoglobin levels lower oxygen-carrying capacity, prompting compensatory increases in cardiac output. This leads to higher blood volume and faster ventricular filling, which can accentuate late diastolic vibrations. For example, a patient with hemoglobin levels of 9 g/dL (normal range: 12–15 g/dL for women, 13.5–17.5 g/dL for men) may exhibit an S4 sound due to hyperdynamic circulation. Treating the anemia—through iron supplementation (e.g., 100–200 mg elemental iron daily) or addressing underlying causes like gastrointestinal bleeding—often resolves the sound. Here, the S4 serves as a clue to an unrelated condition rather than a primary cardiac issue.
Hypertension, while typically pathological, can also produce benign S4 sounds in certain scenarios. Chronic elevated blood pressure causes left ventricular hypertrophy, increasing wall stiffness and impairing relaxation. However, in early stages or well-managed cases, this hypertrophy may not yet reflect significant dysfunction. For instance, a 45-year-old with controlled hypertension (130/80 mmHg on lisinopril 10 mg daily) and mild left ventricular hypertrophy (wall thickness 11 mm) might have an S4 sound without symptoms or reduced ejection fraction. The key distinction? Absence of strain patterns on ECG or signs of heart failure. In such cases, the S4 is a marker of adaptation, not decompensation.
In practice, differentiating benign from pathological S4 sounds requires a systematic approach. Start by evaluating patient history: Is there a history of endurance training? Recent blood work indicating anemia? Long-standing hypertension? Next, correlate findings with diagnostic tests: echocardiography to assess wall thickness and ejection fraction, ECG to rule out strain patterns, and hemoglobin levels to identify anemia. If the S4 is isolated, asymptomatic, and accompanied by normal cardiac function, it’s likely benign. However, any doubt warrants further investigation, such as stress testing or advanced imaging, to exclude underlying pathology. By recognizing these normal causes, clinicians can avoid misdiagnosis and unnecessary interventions, ensuring appropriate care tailored to the individual.
Mastering Ear Care: A Step-by-Step Guide to Applying Pure Sound Wax
You may want to see also
Explore related products

$57.99 $77.99





![]()
Pathological S4 Causes: Conditions like left ventricular hypertrophy or ischemia often produce abnormal S4 sounds
The S4 heart sound, often described as a late diastolic "atrial gallop," is typically benign in children and young adults, where it reflects a compliant, healthy ventricle. However, in older individuals or those with cardiovascular disease, an S4 sound becomes pathological, signaling increased ventricular stiffness or impaired relaxation. Conditions like left ventricular hypertrophy (LVH) and ischemia are prime culprits, as they disrupt the heart’s normal filling dynamics, forcing the atria to contract against elevated resistance. This produces the audible S4, a red flag for underlying cardiac dysfunction.
Left ventricular hypertrophy, often a consequence of chronic hypertension or aortic stenosis, thickens the heart muscle, reducing ventricular compliance. As the ventricle stiffens, it resists early diastolic filling, delaying blood flow until atrial contraction. This delayed filling generates the S4 sound, which clinicians can detect using a bell chest piece at the cardiac apex. Patients with LVH may also exhibit symptoms like dyspnea, fatigue, or chest pain, but the S4 serves as a critical auscultatory marker for early detection. Managing LVH requires addressing its root cause—for instance, controlling blood pressure with medications like ACE inhibitors or beta-blockers, which can slow disease progression and potentially reduce S4 intensity.
Ischemia, another pathological S4 cause, occurs when coronary artery disease restricts blood flow to the myocardium, impairing ventricular relaxation. During ischemic episodes, the heart muscle becomes stiff and non-compliant, mimicking the effects of LVH. An S4 sound in this context often accompanies other signs of ischemia, such as ST-segment changes on ECG or angina. Treatment focuses on restoring coronary perfusion, either through medications like nitrates or interventions like angioplasty. Early recognition of the S4 in ischemic patients is vital, as it may precede more severe complications like heart failure or myocardial infarction.
Distinguishing a pathological S4 from its benign counterpart requires clinical context and additional diagnostic tools. For instance, echocardiography can confirm LVH by measuring wall thickness, while stress testing can identify ischemia. Auscultation alone is insufficient, but the S4 serves as a prompt for further investigation. Patients over 40, especially those with risk factors like hypertension, diabetes, or smoking, should undergo thorough evaluation if an S4 is detected. Ignoring this finding could delay treatment for life-threatening conditions.
In summary, a pathological S4 sound is a critical indicator of ventricular dysfunction, particularly in LVH or ischemia. Its presence demands immediate attention, as it often reflects advanced cardiac disease. Clinicians should combine auscultation with imaging and functional tests to confirm the underlying cause. For patients, recognizing associated symptoms like shortness of breath or chest discomfort can expedite diagnosis. Early intervention, whether through antihypertensive therapy, revascularization, or lifestyle changes, can mitigate progression and improve outcomes. The S4 is more than a murmur—it’s a call to action.
Building Strong: Understanding the Core of a Sound Foundation
You may want to see also
Explore related products






![]()
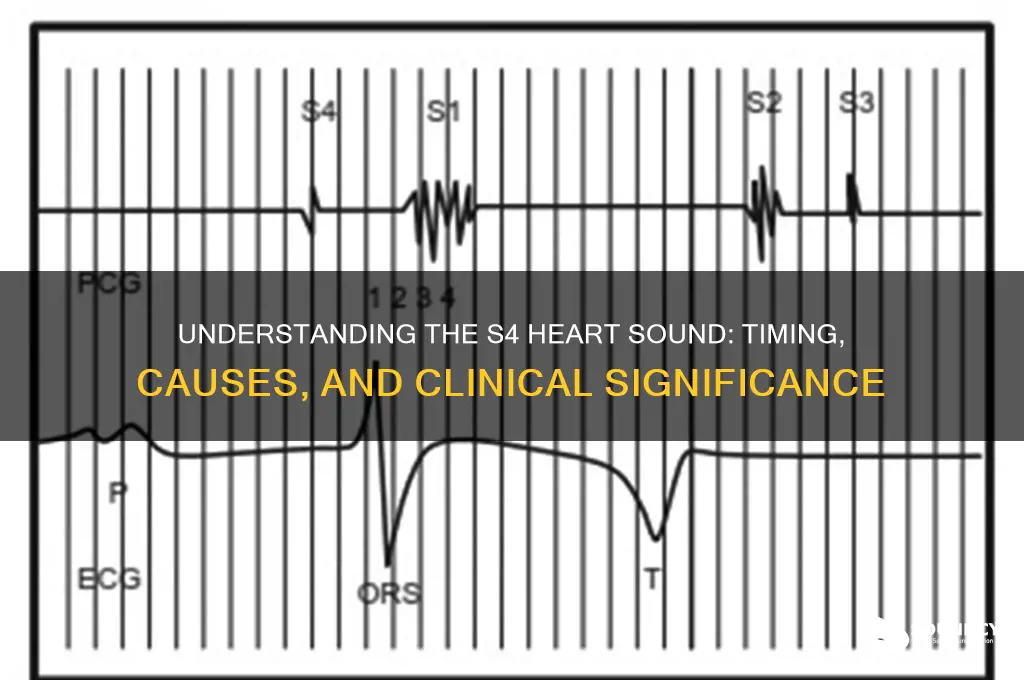
S4 Timing: Occurs during late diastole, just before the first heart sound (S1)
The S4 heart sound, often referred to as the "atrial gallop," is a subtle yet significant marker of cardiac function. Its timing is crucial for diagnosis: it occurs during late diastole, just before the first heart sound (S1). This precise moment is when the atria contract forcefully to push blood into a stiff or non-compliant ventricle, creating the low-pitched "thud" characteristic of S4. Clinicians rely on this timing to differentiate S4 from other murmurs or sounds, as it aligns with the pathophysiology of conditions like left ventricular hypertrophy or restrictive cardiomyopathy.
To detect an S4 sound, position the stethoscope at the cardiac apex with the patient in the left lateral decubitus position. The sound is best heard during expiration, as intrathoracic pressure increases, enhancing the transmission of low-frequency sounds. For older adults or patients with hypertension, S4 is more common due to increased ventricular stiffness. However, in younger individuals, its presence may indicate a more severe underlying condition, such as aortic stenosis or hypertrophic cardiomyopathy. Always correlate auscultation findings with echocardiography for confirmation.
From a comparative perspective, the S4 sound contrasts sharply with the S3 sound, which also occurs in diastole but earlier in the cycle. While S3 is often benign and heard in athletes or pregnant women, S4 is almost always pathological. The timing of S4—just before S1—is a key differentiator. For instance, in a patient with heart failure, an S4 suggests advanced disease with significant ventricular stiffness, whereas an S3 might indicate early-stage volume overload. Understanding this distinction is critical for accurate diagnosis and treatment planning.
Practically, managing conditions associated with S4 involves addressing the underlying cause. For hypertensive patients, aggressive blood pressure control with medications like ACE inhibitors or beta-blockers can reduce ventricular stiffness over time. In cases of aortic stenosis, surgical intervention may be necessary. Lifestyle modifications, such as reducing sodium intake and increasing physical activity, can also improve ventricular compliance. For clinicians, documenting the presence of S4 in patient records is essential, as it serves as a baseline for monitoring disease progression or response to therapy.
In summary, the S4 sound’s timing during late diastole, just before S1, is a diagnostic cornerstone. Its detection requires careful auscultation and an understanding of its pathophysiological implications. By recognizing this timing and its clinical significance, healthcare providers can better identify and manage conditions associated with ventricular stiffness, ultimately improving patient outcomes. Always integrate this finding with other diagnostic tools for a comprehensive cardiac assessment.
Unveiling the Unique Growls and Snarls of Tasmanian Devils
You may want to see also
Explore related products




![]()
S4 Characteristics: Low-pitched, rumbling sound, best heard at the apex with a bell
The S4 heart sound, often described as a low-pitched, rumbling noise, is a critical indicator of cardiac function, particularly in assessing ventricular filling dynamics. This sound, best auscultated at the cardiac apex using the bell of a stethoscope, is generated during the atrial contraction phase, just before the mitral valve opens. Its presence can signify increased ventricular stiffness or elevated filling pressures, making it a valuable diagnostic tool in cardiology. Clinicians should note that the S4 is typically absent in healthy individuals but may emerge in conditions like left ventricular hypertrophy, ischemic heart disease, or restrictive cardiomyopathy.
To effectively detect an S4 sound, proper technique is essential. Position the patient in the left lateral decubitus position, as this optimizes acoustic transmission at the apex. Use the bell of the stethoscope, which is more sensitive to low-frequency sounds, and apply light pressure to avoid dampening the vibration. Instruct the patient to exhale slowly while listening, as this can enhance the audibility of the S4. For pediatric patients, particularly those under 12 years old, the S4 is rarely physiological and warrants further investigation if detected.
Comparatively, the S4 sound differs from the S3 gallop rhythm, which is also low-pitched but occurs earlier in the cardiac cycle. While the S3 is associated with rapid ventricular filling, the S4 reflects atrial effort against a stiff or non-compliant ventricle. Misidentifying one for the other can lead to diagnostic errors, so clinicians should focus on timing and context. For instance, an S4 is more likely in a 60-year-old with hypertension and left ventricular hypertrophy, whereas an S3 might be observed in a 30-year-old with dilated cardiomyopathy.
Incorporating S4 auscultation into routine cardiac exams can provide early clues to underlying pathology. For example, in patients with uncontrolled hypertension, the presence of an S4 may indicate progression to heart failure with preserved ejection fraction (HFpEF). In such cases, initiating or adjusting antihypertensive therapy, such as increasing the dose of an ACE inhibitor from 10 mg to 20 mg daily, could be warranted. Always correlate auscultatory findings with imaging studies like echocardiography for a comprehensive assessment.
Finally, while the S4 sound is a valuable clinical sign, it is not infallible. Factors like obesity, emphysema, or poor acoustic windows can obscure its detection. In such scenarios, advanced diagnostic tools like tissue Doppler imaging or cardiac MRI may be necessary to confirm ventricular stiffness or elevated filling pressures. Nonetheless, mastering S4 auscultation remains a cornerstone skill for clinicians, offering immediate insights into cardiac mechanics without reliance on technology.
Effective Soundproofing Techniques for Creating a Quiet Ceiling Barrier
You may want to see also
![]()
Diagnosing S4: Requires careful auscultation, often confirmed with echocardiography or other imaging studies
The S4 heart sound, often described as a late diastolic "atrial kick," is a subtle yet critical indicator of cardiac function. Detecting it requires more than routine auscultation; it demands a focused, deliberate approach. Begin by positioning the patient in the left lateral decubitus position, using a diaphragm stethoscope, and listening intently at the cardiac apex. The S4 is low-pitched and brief, often masked by respiratory sounds or other murmurs, making it easy to miss without careful technique.
While auscultation is the first step, confirming an S4 sound often necessitates advanced imaging. Echocardiography is the gold standard, providing visual evidence of left ventricular stiffness or hypertrophy, conditions commonly associated with S4. For instance, in a 65-year-old patient with hypertension, an S4 detected during auscultation, coupled with echocardiographic findings of increased left ventricular mass, strongly suggests diastolic dysfunction. Other modalities, such as cardiac MRI or CT, may be employed in complex cases to assess myocardial structure and function further.
Misdiagnosis is a risk without proper technique and confirmation. An S4 can mimic other sounds, such as a split S1 or a mid-diastolic murmur, leading to confusion. For example, a clinician might mistake an S4 for mitral regurgitation in a patient with a history of valvular disease. To avoid this, correlate auscultation findings with patient history, risk factors, and imaging results. Additionally, consider the context: an S4 in a young athlete may reflect benign ventricular hypertrophy, whereas in an elderly patient with diabetes, it could signal heart failure with preserved ejection fraction (HFpEF).
Practical tips can enhance diagnostic accuracy. Use a systematic approach: listen for the S4 immediately before S1, during late diastole, and ask the patient to exhale slowly to reduce respiratory interference. If unsure, repeat the exam after having the patient perform a Valsalva maneuver, which can accentuate the S4. For imaging, ensure echocardiography includes tissue Doppler and strain imaging to evaluate diastolic function comprehensively. By combining meticulous auscultation with confirmatory imaging, clinicians can confidently diagnose an S4 and tailor management to the underlying cause.
Apple TV's Sound Mirroring: What You Need to Know
You may want to see also
Frequently asked questions
An S4 heart sound, also known as a fourth heart sound or atrial gallop, is an extra heart sound occurring just after the S2 (aortic valve closure) and before the S1 (mitral valve closure) in the cardiac cycle.
An S4 sound is typically heard in conditions where the left ventricle is stiff or has reduced compliance, such as in hypertension, left ventricular hypertrophy, or heart failure with preserved ejection fraction (HFpEF).
An S4 sound is distinguished by its timing (just before S1), low-pitched quality, and association with a stiff or non-compliant left ventricle. It is often described as a "presystolic" sound.
The presence of an S4 sound often indicates increased left ventricular filling pressure, reduced diastolic function, or ventricular stiffness, which can be seen in conditions like hypertension, aortic stenosis, or heart failure.
An S4 sound is rarely heard in healthy individuals, especially younger people. However, it may occasionally be present in well-trained athletes or elderly individuals due to age-related changes in ventricular compliance.