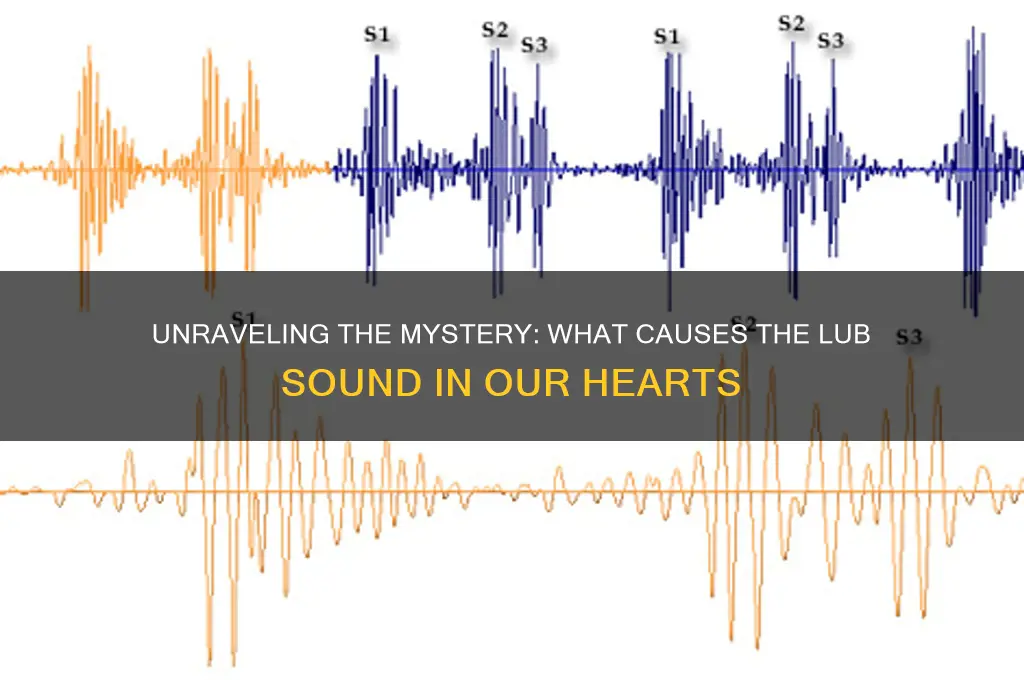
The distinctive lub sound, often associated with the heartbeat, is a fundamental aspect of cardiovascular function, arising from the mechanical processes within the heart. This sound is primarily produced by the closing of the heart’s valves during the cardiac cycle. Specifically, the lub corresponds to the closure of the atrioventricular valves—the tricuspid and mitral valves—at the beginning of systole, when the ventricles contract to pump blood. This closure prevents backflow of blood into the atria, creating the first heart sound, which is typically low-pitched and longer in duration. Understanding the origin of this sound provides valuable insights into the heart’s rhythmic activity and overall health, making it a crucial element in both medical diagnostics and the study of human physiology.
| Characteristics | Values |
|---|---|
| Source | The "lub" sound primarily originates from the closing of the atrioventricular (AV) valves (mitral and tricuspid valves) in the heart. |
| Mechanism | The sound is caused by the sudden turbulent blood flow and the snapping shut of the valves as the ventricles contract (systole). |
| Timing | Occurs at the beginning of ventricular systole, immediately after electrical depolarization of the ventricles. |
| Duration | Typically lasts for 0.1 to 0.12 seconds (100-120 milliseconds). |
| Frequency | The sound has a low-pitched frequency, usually between 20 to 60 Hz. |
| Intensity | It is generally softer compared to the "dub" sound (caused by semilunar valve closure). |
| Physiology | Reflects the normal functioning of the heart's valves and the initiation of ventricular contraction. |
| Clinical Significance | Abnormalities in the "lub" sound (e.g., splitting, muffling, or absence) can indicate valve disorders, heart block, or other cardiac conditions. |
Explore related products





What You'll Learn
- Heart Valve Mechanics: Blood flow through heart valves creates turbulence, generating the characteristic lub-dub sounds
- Systolic vs. Diastolic: Lub occurs during systole (ventricular contraction); dub during diastole (ventricular relaxation)
- Stethoscope Amplification: Stethoscopes enhance heart sounds by amplifying vibrations transmitted through the chest wall
- Murmurs and Abnormalities: Irregular blood flow can cause murmurs, altering or adding to the normal lub-dub rhythm
- Cardiac Cycle Timing: The timing and sequence of valve closures determine the precise lub and dub sounds
![]()
Heart Valve Mechanics: Blood flow through heart valves creates turbulence, generating the characteristic lub-dub sounds
The heart's rhythmic lub-dub is a symphony of fluid dynamics and anatomical precision. As blood surges through the heart, it encounters four valves—tricuspid, pulmonary, mitral, and aortic—each a masterpiece of design. When these valves snap shut, they create turbulence in the blood flow, akin to the abrupt closure of a dam gate. This turbulence generates the audible vibrations we recognize as heart sounds. The first sound, or S1 (the "lub"), occurs when the mitral and tricuspid valves close, marking the beginning of systole. The second sound, or S2 (the "dub"), follows as the aortic and pulmonary valves close, signaling the end of systole. Understanding this mechanism not only demystifies the lub-dub but also highlights the heart's efficiency in maintaining unidirectional blood flow.
To visualize this process, imagine a high-speed train passing through gates. The gates must close swiftly to ensure the train moves forward without reversing. Similarly, heart valves must close with precision to prevent backflow. The turbulence created during closure is a byproduct of this necessity, translated into sound by the surrounding tissues. Clinicians use stethoscopes to amplify these sounds, assessing their quality, timing, and intensity to diagnose valve disorders. For instance, a "murmur" indicates turbulent flow due to valve leakage or stenosis, often requiring further evaluation via echocardiography. This diagnostic approach underscores the practical significance of understanding heart valve mechanics.
From an engineering perspective, the heart’s valves are marvels of biomechanics. The mitral valve, for example, has a larger surface area to handle the high-pressure flow from the left atrium to the ventricle. Its closure generates a louder component of the S1 sound compared to the tricuspid valve. Conversely, the aortic valve’s closure produces a higher-pitched S2 due to the rapid deceleration of blood in the aorta. These differences are not arbitrary; they reflect the heart’s adaptation to varying pressures and volumes across its chambers. Engineers and medical researchers often draw inspiration from such natural systems to design prosthetics and mechanical valves that mimic this efficiency.
For those curious about their own heart sounds, a simple exercise can provide insight. Place a stethoscope or even a glass cup (as a makeshift amplifier) over the chest’s left side, where the mitral valve is closest to the surface. Listen for the lub-dub, noting its clarity and rhythm. A healthy heart produces distinct, evenly spaced sounds. Irregularities, such as a split S2 (a delayed component of the dub) in children or a prolonged S1 in athletes, are normal variants. However, persistent abnormalities warrant consultation with a healthcare provider. This self-assessment, while not a substitute for professional evaluation, fosters awareness of one’s cardiovascular health.
In conclusion, the lub-dub sounds are more than just auditory cues; they are a window into the heart’s functional integrity. By understanding the turbulence generated by valve closure, we appreciate the intricate balance between anatomy and physiology. Whether for medical diagnosis, bioengineering inspiration, or personal health awareness, this knowledge transforms the heartbeat from a mundane rhythm into a testament to biological precision. Listen closely, and you’ll hear not just a sound, but a story of life’s most vital machinery at work.
Exploring the Genetic Links Behind Speech Sound Disorders
You may want to see also
Explore related products






![]()
Systolic vs. Diastolic: Lub occurs during systole (ventricular contraction); dub during diastole (ventricular relaxation)
The heart's rhythmic dance is a symphony of sounds, each beat a testament to its intricate mechanics. Among these, the iconic "lub-dub" stands out, a duo of noises that signify the heart's vital contractions and relaxations. But what exactly makes the "lub" sound, and how does it differ from its counterpart?
The Systolic Symphony: Unraveling the Lub
Imagine a powerful squeeze, a moment of intense pressure as the heart's ventricles contract. This is systole, and it's during this phase that the "lub" sound takes center stage. As the ventricles contract, they force blood through the semilunar valves (aortic and pulmonary), creating a surge of pressure. This sudden rush of blood causes these valves to snap shut, producing the distinctive "lub" noise. It's a sound that echoes the heart's strength, a testament to its ability to pump oxygen-rich blood throughout the body.
A Matter of Timing and Force
The "lub" is not just a random noise; it's a precise indicator of the heart's performance. Its occurrence during systole is crucial, as it marks the beginning of the heart's pumping action. The force of the ventricular contraction determines the intensity of the "lub." In a healthy heart, this sound is robust and clear, indicating a strong, efficient pump. For instance, in adults, a normal systolic blood pressure (the force at which the heart pumps blood) ranges from 90 to 120 mmHg, contributing to a healthy "lub" sound.
Diastole's Silence and the Dub's Entry
In contrast, diastole is a period of relaxation, a quiet interlude where the heart's ventricles fill with blood. Here, the "dub" sound emerges, but it's not a result of ventricular action. Instead, it's the atrioventricular valves (tricuspid and mitral) closing that creates this softer noise. As the ventricles relax, blood flows from the atria into the ventricles, causing these valves to shut, producing the "dub." This sound is often less pronounced, a gentle reminder of the heart's preparation for the next powerful contraction.
Practical Insights: Listening to the Heart's Rhythms
Understanding these sounds is not just academic; it's a practical skill for healthcare professionals and enthusiasts alike. Auscultation, the act of listening to the heart using a stethoscope, allows one to differentiate between the "lub" and "dub." The "lub" is typically louder and occurs first, followed by a brief pause and then the softer "dub." This pattern repeats with each heartbeat, providing a real-time assessment of the heart's function. For instance, a muffled "lub" might indicate a problem with the semilunar valves, while an irregular rhythm could suggest arrhythmia.
In the realm of cardiology, these sounds are vital diagnostic tools, offering a non-invasive way to assess heart health. By deciphering the "lub-dub" code, medical professionals can detect issues like valve disorders, hypertension, or heart muscle problems. This simple yet powerful auditory cue is a window into the heart's complex world, where each sound tells a story of its function and well-being.
Do Bats Make a Sound? Unveiling Their Unique Communication Methods
You may want to see also
Explore related products





![]()
Stethoscope Amplification: Stethoscopes enhance heart sounds by amplifying vibrations transmitted through the chest wall
The "lub" sound, medically known as S1, is the first heart sound in the cardiac cycle, marking the closure of the atrioventricular valves (mitral and tricuspid). To hear this faint vibration, stethoscopes act as mechanical amplifiers, funneling sound waves through a hollow tube to the listener’s ears. The chest piece, typically made of metal or resin, captures vibrations transmitted through the chest wall, while the diaphragm and bell filter frequencies to isolate low-pitched (S1) and high-pitched (S2) sounds, respectively. Without this amplification, the "lub" would remain imperceptible to the unaided ear, drowned out by ambient noise or the body’s surface acoustics.
Consider the physics at play: sound waves from the heart travel through layers of skin, fat, muscle, and air, losing intensity with each medium. A stethoscope’s rigid tubing minimizes this loss by providing a direct pathway for vibration transmission. The diaphragm, a flat, disc-like component, is particularly sensitive to the 20–100 Hz frequency range of S1, ensuring the "lub" is not just louder but also clearer. For pediatric patients, whose heart rates average 70–100 beats per minute in children aged 1–10, the stethoscope’s amplification is critical for distinguishing rapid, softer sounds from background noise.
To optimize stethoscope use for S1 amplification, position the diaphragm firmly over the mitral area (fifth intercostal space, midclavicular line) or the tricuspid area (left sternal border). Apply enough pressure to create a seal but avoid excessive force, which can dampen vibrations. For electronic stethoscopes, adjust the amplification setting to +12–24x for adults or +6–12x for children, ensuring the "lub" is audible without distortion. Regularly clean the chest piece to remove debris that could interfere with sound transmission, and replace diaphragms every 1–2 years to maintain sensitivity.
While traditional stethoscopes rely on mechanical principles, digital models offer additional advantages. These devices can amplify sounds up to 24x, filter out ambient noise, and record heart sounds for later analysis. For instance, the 3M Littmann 3200 amplifies S1 by up to 24x and allows real-time visualization of sound waves via Bluetooth connectivity. However, digital stethoscopes require battery maintenance and are more expensive, making them less accessible in low-resource settings. Regardless of the model, the core function remains the same: to amplify the "lub" sound, transforming it from a faint vibration into a diagnostic tool.
In practice, stethoscope amplification is not just about hearing the "lub" but interpreting its quality. A split S1, for example, indicates a delay between mitral and tricuspid closure, often seen in right bundle branch block. Amplification allows clinicians to detect such nuances, which are crucial for accurate diagnosis. For medical students or practitioners, mastering stethoscope technique—proper placement, pressure, and listening—is as essential as the device’s amplification capabilities. Together, they bridge the gap between the heart’s silent mechanics and the audible "lub" that defines cardiac health.
Understanding High-Quality Sound: Clarity, Depth, and Immersive Audio Experience
You may want to see also
Explore related products





![]()
Murmurs and Abnormalities: Irregular blood flow can cause murmurs, altering or adding to the normal lub-dub rhythm
The heart's rhythmic lub-dub is a symphony of valves closing, but irregularities in blood flow can introduce discordant notes. Murmurs, often described as whooshing or swishing sounds, arise when blood flows turbulently through the heart. This turbulence can occur due to structural abnormalities like valve defects, holes in the heart, or narrowed arteries. For instance, a stenotic aortic valve forces blood to flow through a smaller opening, creating a murmur audible during systole (the lub phase). Understanding these murmurs is crucial, as they can signal underlying conditions requiring medical attention.
Detecting murmurs typically involves auscultation with a stethoscope, where healthcare providers listen for deviations from the normal lub-dub pattern. Murmurs are classified by their timing (systolic or diastolic), intensity (on a scale of 1 to 6), and location (e.g., at the apex or base of the heart). For example, a grade 3/6 systolic murmur at the left sternal border might indicate aortic stenosis. While some murmurs are harmless ("innocent" murmurs, common in children and pregnant women), others warrant further investigation, such as echocardiograms or Doppler studies, to assess their cause and severity.
Not all murmurs are created equal, and their implications vary widely. In children, a ventricular septal defect (a hole between the heart’s lower chambers) can produce a loud, holosystolic murmur, often requiring surgical repair. In contrast, older adults might develop murmurs due to age-related valve degeneration, such as mitral regurgitation, where blood leaks backward into the left atrium. Recognizing these differences is essential for tailored management, which may include medications, lifestyle changes, or surgical interventions.
Prevention and early detection are key to managing murmurs effectively. Regular check-ups, especially for individuals with risk factors like hypertension or a family history of heart disease, can catch abnormalities before they worsen. For those diagnosed with murmurs, monitoring symptoms like shortness of breath, fatigue, or chest pain is critical. Practical tips include maintaining a heart-healthy diet, exercising regularly, and avoiding smoking. In some cases, antibiotics may be prescribed before dental procedures to prevent infective endocarditis, a rare but serious complication of certain heart murmurs.
In conclusion, while the lub-dub rhythm is the heart’s normal melody, murmurs serve as important indicators of irregular blood flow. By understanding their causes, detection methods, and implications, individuals and healthcare providers can take proactive steps to address underlying issues. Whether benign or symptomatic, murmurs remind us of the heart’s complexity and the need for vigilant care to preserve its harmonious function.
The Accuracy of Sound of Metal: A Realistic Portrayal?
You may want to see also
Explore related products






![]()
Cardiac Cycle Timing: The timing and sequence of valve closures determine the precise lub and dub sounds
The heart's rhythmic lub-dub is a symphony of precision, orchestrated by the cardiac cycle's timing. This cycle, a sequence of contractions and relaxations, relies on the exact moment when heart valves close. The lub sound, medically termed the first heart sound (S1), occurs when the atrioventricular valves (tricuspid and mitral) slam shut as the ventricles begin to contract. This closure prevents blood from flowing backward into the atria, creating a low-pitched vibration audible to the stethoscope. Understanding this timing is crucial for diagnosing valve disorders, as deviations can indicate conditions like mitral stenosis or regurgitation.
To appreciate the lub's origin, consider the cardiac cycle's phases. During ventricular systole, the ventricles contract, forcing blood into the aorta and pulmonary artery. The atrioventricular valves close abruptly, generating S1. This closure is not just a mechanical event but a critical checkpoint ensuring unidirectional blood flow. For instance, in children, the lub sound is softer due to smaller valve structures and lower blood pressure, while in adults, it becomes more pronounced with increased cardiac output. Clinicians use this knowledge to assess heart health, often pairing it with echocardiograms for a comprehensive evaluation.
The timing of valve closures is so precise that even milliseconds matter. For example, in a healthy adult, the atrioventricular valves close within 0.1 seconds of ventricular contraction onset. This rapid closure is essential for maintaining efficient blood flow. However, in conditions like left bundle branch block, the timing is delayed, altering the lub's quality. Patients with such conditions may exhibit a "split S1," where the mitral and tricuspid valves close at slightly different times, producing a double lub sound. Recognizing these nuances allows healthcare providers to tailor treatments, such as pacing therapies, to restore normal cardiac rhythm.
Practical tips for auscultation include placing the stethoscope at the mitral area (fifth intercostal space, mid-clavicular line) to hear the lub clearly. Encourage patients to breathe deeply, as inspiration increases venous return and amplifies heart sounds. For pediatric patients, use a smaller diaphragm and apply gentle pressure to avoid discomfort. Remember, the lub's timing and intensity provide vital clues about valve function and overall cardiac performance. By mastering this aspect of the cardiac cycle, clinicians can detect early signs of dysfunction and intervene effectively, ensuring the heart's symphony remains harmonious.
Unveiling Silent Sound Technology: Revolutionizing Communication and Beyond
You may want to see also
Frequently asked questions
The lub sound, also known as the first heart sound (S1), is caused by the closure of the atrioventricular (AV) valves—the mitral and tricuspid valves—as the ventricles begin to contract.
The lub sound is generally louder because the closure of the AV valves (mitral and tricuspid) involves a larger pressure difference and more forceful snapping shut compared to the semilunar valves (aortic and pulmonary) that produce the dub sound.
Yes, the lub sound can be abnormal if there is a problem with the AV valves, such as mitral stenosis or regurgitation, which can alter the timing, pitch, or intensity of the sound.
The lub sound (S1) is produced by the closure of the AV valves at the start of ventricular contraction, while the dub sound (S2) is caused by the closure of the semilunar valves (aortic and pulmonary) at the end of ventricular contraction.
The lub sound can be heard using a stethoscope placed on the chest, specifically at the mitral or tricuspid valve areas, during a cardiac auscultation. It is a low-pitched sound that marks the beginning of systole.