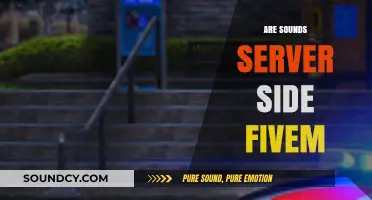
Speech sound disorders (SSDs), characterized by difficulties in producing speech sounds correctly, have long been a subject of interest in both clinical and research settings. While environmental factors such as hearing loss, oral motor deficits, and socio-economic influences play significant roles, there is growing evidence to suggest a genetic component to these disorders. Recent studies have identified specific genetic markers and familial patterns that may predispose individuals to SSDs, indicating that heredity could contribute to the etiology of conditions like childhood apraxia of speech or phonological disorders. Understanding the genetic underpinnings of SSDs not only sheds light on their origins but also holds promise for early identification, personalized interventions, and potential preventive measures.
| Characteristics | Values |
|---|---|
| Genetic Influence | Speech sound disorders (SSD) have a significant genetic component, with heritability estimates ranging from 40% to 70%. |
| Twin Studies | Studies on twins show higher concordance rates for SSD in monozygotic twins compared to dizygotic twins, suggesting a strong genetic link. |
| Family Aggregation | SSDs tend to cluster in families, indicating a familial predisposition. |
| Candidate Genes | Genes associated with neural migration, language development, and speech motor control (e.g., FOXP2, CNTNAP2, GRIN2A) have been implicated in SSDs. |
| Chromosomal Abnormalities | Certain chromosomal abnormalities (e.g., 7q31, 16p12.2) are linked to SSDs, often co-occurring with other developmental disorders. |
| Polygenic Risk | SSDs are likely polygenic, involving multiple genes with small effects rather than a single causative gene. |
| Gene-Environment Interaction | Genetic predisposition interacts with environmental factors (e.g., parental speech patterns, socioeconomic status) to influence SSD risk. |
| Overlap with Other Disorders | SSDs often co-occur with conditions like developmental language disorder, dyslexia, and autism spectrum disorder, which also have genetic underpinnings. |
| Population Variability | Genetic contributions to SSDs may vary across populations due to genetic diversity and environmental differences. |
| Epigenetic Factors | Epigenetic mechanisms (e.g., DNA methylation) may modulate gene expression related to speech and language development, contributing to SSD risk. |
| Genetic Testing | While genetic testing is not yet standard for SSDs, advancements in genomics may lead to personalized interventions in the future. |
| Heritability Differences by Type | Heritability may vary depending on the type of SSD (e.g., articulation disorders vs. phonological disorders). |
| Role of FOXP2 Gene | The FOXP2 gene is a well-studied example of a gene directly linked to speech and language development, with mutations causing severe SSDs. |
| Environmental Modifiers | Factors like early intervention, parental involvement, and speech therapy can mitigate genetic risks and improve outcomes for individuals with SSDs. |
| Research Gaps | Further research is needed to identify specific genetic variants, understand gene-environment interactions, and develop targeted therapies for SSDs. |
Explore related products






What You'll Learn
![]()
Genetic markers linked to speech sound disorders
Recent research has begun to unravel the complex genetic underpinnings of speech sound disorders (SSD), shedding light on specific genetic markers that may contribute to their development. Studies have identified several candidate genes associated with SSD, particularly those involved in neural development, migration, and connectivity. For instance, variations in the FOXP2 gene, often referred to as the "language gene," have been linked to impairments in speech and language production. Mutations in FOXP2 are known to cause severe speech and language disorders, and even subtle variations in this gene may increase susceptibility to SSD in the general population.
Another genetic marker of interest is the CNTNAP2 gene, which plays a crucial role in neuronal communication and the development of neural circuits. Variants in CNTNAP2 have been associated with a range of neurodevelopmental disorders, including SSD, autism spectrum disorder (ASD), and specific language impairment (SLI). Research suggests that these variants may disrupt the precise timing and coordination of neural signals required for accurate speech production. Additionally, the ATP2C2 gene, involved in intracellular transport and neural function, has been implicated in cases of childhood apraxia of speech (CAS), a severe form of SSD.
Genome-wide association studies (GWAS) have further expanded our understanding of the genetic landscape of SSD. These studies have identified multiple loci across the genome that are associated with speech and language difficulties. For example, a GWAS published in *Nature Genetics* highlighted several genetic regions linked to phonological awareness and speech sound processing, which are core deficits in SSD. While many of these loci have small individual effects, their cumulative impact may significantly influence an individual's risk of developing SSD.
Epigenetic factors, which influence gene expression without altering the DNA sequence, also play a role in the genetic basis of SSD. Studies have shown that environmental factors, such as prenatal exposure to toxins or early childhood experiences, can modify the expression of genes related to speech and language development. For instance, epigenetic changes in genes like SRPX2, which is involved in neuronal migration and synaptic plasticity, have been observed in individuals with SSD. This interplay between genetics and environment underscores the complexity of SSD etiology.
Understanding these genetic markers has important implications for early identification, intervention, and personalized treatment of SSD. Genetic testing, though not yet standard practice for SSD, could potentially identify at-risk individuals and guide targeted therapies. Moreover, insights into the genetic mechanisms of SSD may inform the development of novel interventions that address the underlying neural deficits. As research continues to advance, the identification of additional genetic markers will likely refine our understanding of SSD and improve outcomes for affected individuals.
Identifying a Failing Flywheel: Unusual Noises and Warning Signs
You may want to see also
Explore related products






![]()
Familial patterns in speech sound disorder prevalence
Research into the genetic underpinnings of speech sound disorders (SSDs) has increasingly highlighted the role of familial patterns in their prevalence. Studies have consistently shown that children with a family history of SSDs are at a higher risk of developing these disorders themselves. This familial aggregation suggests a genetic component, as the likelihood of SSDs occurring in multiple family members exceeds what would be expected by chance alone. For instance, twin studies have demonstrated a higher concordance rate for SSDs in monozygotic twins compared to dizygotic twins, further supporting the idea that genetic factors play a significant role in the transmission of these disorders.
Familial patterns in SSD prevalence are not limited to immediate family members but often extend to extended relatives, indicating a broader genetic influence. Parents with a history of speech or language difficulties are more likely to have children with similar issues, and this risk increases if both parents are affected. Additionally, siblings of children with SSDs are at a higher risk, with prevalence rates significantly elevated compared to the general population. These patterns suggest that genetic susceptibility to SSDs may be inherited in a complex manner, potentially involving multiple genes and their interactions with environmental factors.
Genetic studies have begun to identify specific loci and candidate genes associated with SSDs, though the exact mechanisms remain under investigation. For example, variations in genes related to neural migration, auditory processing, and speech motor control have been implicated in familial cases of SSDs. The FOXP2 gene, often referred to as the "language gene," is one of the most studied in this context, as mutations in this gene are known to cause severe speech and language impairments. However, SSDs are likely polygenic, meaning multiple genes contribute to the phenotype, each with small individual effects but significant cumulative impact.
Environmental factors also play a role in the manifestation of SSDs, even in families with a genetic predisposition. Factors such as socioeconomic status, parental education, and access to early intervention services can influence the severity and outcome of SSDs. However, the consistent observation of familial clustering underscores the importance of genetic factors in determining susceptibility. Understanding these familial patterns is crucial for early identification and intervention, as children from high-risk families can benefit from targeted screening and support to address speech sound difficulties before they become more entrenched.
In conclusion, familial patterns in the prevalence of speech sound disorders provide compelling evidence for a genetic basis, though the interplay between genetic and environmental factors is complex. The higher risk observed in relatives of affected individuals highlights the need for comprehensive family histories in clinical assessments. Ongoing genetic research aims to unravel the specific genes and mechanisms involved, which could lead to more personalized approaches to diagnosis and treatment. By recognizing and addressing the familial nature of SSDs, clinicians and researchers can improve outcomes for individuals and families affected by these disorders.
How Sweet the Sound: Your Perfect Beach Rental Escape Awaits
You may want to see also
Explore related products



$66.49 $69.99



![]()
Role of inherited neurological factors in articulation
Research indicates that speech sound disorders (SSD) often have a genetic component, with inherited neurological factors playing a significant role in articulation difficulties. Studies on twins and families have shown a higher concordance rate for SSD among identical twins compared to fraternal twins, suggesting a strong genetic influence. This genetic predisposition is believed to affect the development and functioning of neural pathways involved in speech motor planning and execution. For instance, variations in genes associated with neural migration, synaptic function, and brain connectivity may contribute to the impaired coordination of articulatory movements observed in individuals with SSD.
Inherited neurological factors can influence articulation by affecting the brain's ability to process and produce speech sounds accurately. The cerebellum, basal ganglia, and cortical regions such as Broca's area are critical for speech motor control, and genetic variations can alter their structure or function. For example, mutations in genes like *FOXP2*, which is crucial for speech and language development, have been linked to severe articulation problems. Individuals with *FOXP2* mutations often exhibit difficulties in sequencing and coordinating the precise movements required for clear speech, highlighting the direct connection between genetic factors and articulation.
Neuroimaging studies have further supported the role of inherited neurological factors in SSD. Differences in brain activation patterns during speech tasks have been observed in individuals with a family history of speech disorders, even in the absence of overt symptoms. These findings suggest that genetic predispositions may lead to subtle alterations in neural circuitry, making individuals more susceptible to articulation difficulties under certain conditions, such as developmental stress or environmental triggers. Such neurological differences can manifest as inconsistencies in sound production, phonological errors, or reduced speech clarity.
The interplay between inherited neurological factors and environmental influences is also critical in understanding articulation disorders. While genetic predispositions may set the stage for SSD, factors like auditory processing deficits, oral motor impairments, or limited linguistic input can exacerbate articulation difficulties. For instance, a child with a genetic susceptibility to SSD may struggle more if they also experience hearing impairments or inadequate speech modeling in their environment. This highlights the importance of considering both genetic and environmental factors in the assessment and intervention of articulation disorders.
In conclusion, inherited neurological factors significantly contribute to the role of genetics in speech sound disorders, particularly in articulation. Genetic variations affecting neural development and function can impair the precise coordination of speech movements, leading to observable difficulties in sound production. Understanding these genetic underpinnings not only advances our knowledge of SSD but also informs targeted interventions that address the specific neurological mechanisms involved. Early identification of genetic risk factors, combined with tailored therapeutic approaches, holds promise for improving articulation outcomes in affected individuals.
Exploring the Mystical and Soothing Sound of 432hz Frequency
You may want to see also
Explore related products






![]()
Genetic syndromes associated with speech sound impairments
Speech sound disorders (SSD) can have a genetic basis, and several genetic syndromes are known to be associated with speech sound impairments. These syndromes often involve complex interactions between genetic mutations and developmental processes that affect speech and language. Understanding these genetic links is crucial for early identification, intervention, and support for affected individuals. Below are detailed discussions of specific genetic syndromes associated with speech sound impairments.
Down Syndrome (Trisomy 21) is one of the most well-known genetic conditions linked to speech sound disorders. Individuals with Down syndrome often experience challenges in articulating sounds due to anatomical differences, such as a smaller oral cavity, enlarged tongue (macroglossia), and low muscle tone (hypotonia). These physical characteristics can lead to difficulties in producing precise speech sounds, resulting in phonological errors. Speech therapy tailored to address these anatomical and physiological challenges is essential for improving communication skills in individuals with Down syndrome.
Childhood Apraxia of Speech (CAS), while not a syndrome itself, is often associated with genetic conditions such as FOXP2 gene mutations. The FOXP2 gene plays a critical role in speech and language development, and mutations in this gene can lead to severe speech sound disorders. Individuals with FOXP2 mutations may exhibit difficulties in planning and coordinating the movements necessary for speech, a hallmark of CAS. Early intervention, including intensive speech therapy, is vital for improving speech outcomes in these cases.
Kleen-Wakeman Syndrome (KWS) is a rare genetic disorder caused by mutations in the SRCAP gene. Affected individuals often present with significant speech and language delays, including difficulties in articulating sounds. The syndrome is also associated with intellectual disability, distinctive facial features, and other developmental challenges. Speech-language pathologists play a key role in assessing and addressing the specific speech sound impairments in individuals with KWS, often incorporating augmentative and alternative communication (AAC) strategies when necessary.
22q11.2 Deletion Syndrome (DiGeorge Syndrome) is another genetic condition associated with speech sound disorders. This syndrome results from a deletion on chromosome 22 and is linked to a range of developmental issues, including speech and language impairments. Individuals with 22q11.2 deletion syndrome may experience articulation difficulties, phonological disorders, and overall delays in speech and language development. These impairments are often compounded by other associated features, such as velopharyngeal dysfunction, which can further impact speech clarity. Multidisciplinary intervention, including speech therapy, is critical for addressing these complex needs.
Williams Syndrome (WS), caused by a deletion in the 7q11.23 region of chromosome 7, is also associated with speech sound impairments. While individuals with Williams syndrome often exhibit relative strengths in social communication and vocabulary, they frequently struggle with articulation and phonological skills. The unique cognitive and linguistic profile of Williams syndrome requires specialized speech therapy approaches that focus on improving speech sound production while leveraging their social and linguistic strengths.
In summary, genetic syndromes such as Down syndrome, FOXP2-related disorders, Kleefstra syndrome, 22q11.2 deletion syndrome, and Williams syndrome are associated with speech sound impairments. These conditions highlight the complex interplay between genetics, anatomy, and development in shaping speech and language abilities. Early identification of these syndromes, coupled with targeted speech therapy interventions, is essential for optimizing communication outcomes in affected individuals.
How Sweet the Sound: A Melody That Saved My Soul
You may want to see also
Explore related products
![Hereditary [Blu-ray + DVD + Digital]](https://m.media-amazon.com/images/I/619QdXiRReL._AC_UY218_.jpg)

![Hereditary [DVD]](https://m.media-amazon.com/images/I/41JOgxtUhEL._AC_UY218_.jpg)
![Hereditary (Limited Edition Steelbook) [Region Free][4K Ultra HD]](https://m.media-amazon.com/images/I/61-OrwmN+uL._AC_UY218_.jpg)


![]()
Twin studies on speech sound disorder heritability
Twin studies have been instrumental in unraveling the genetic underpinnings of speech sound disorders (SSDs), providing critical insights into their heritability. These studies leverage the unique genetic similarities between monozygotic (identical) twins, who share 100% of their genes, and dizygotic (fraternal) twins, who share approximately 50% of their genes, to estimate the influence of genetics versus environment. Research has consistently shown that if one twin has an SSD, the likelihood of the other twin also having the disorder is significantly higher in monozygotic twins compared to dizygotic twins. This pattern strongly suggests a genetic component in the etiology of SSDs. For instance, a landmark study by Bishop et al. (1995) found that the concordance rate for SSDs in monozygotic twins was approximately 70%, while in dizygotic twins, it was around 30%, indicating a substantial heritability factor.
Further twin studies have employed advanced statistical models to quantify the heritability of SSDs more precisely. These models often estimate that genetic factors account for 40% to 70% of the variance in speech sound disorders, with the remaining variance attributed to environmental and other non-shared factors. For example, a study by Dale et al. (2003) used structural equation modeling to analyze twin data and concluded that genetic influences were significant, particularly for phonological impairments. These findings align with broader research on language and communication disorders, which often highlight a strong genetic basis. However, it is important to note that heritability does not imply determinism; genetic predisposition interacts with environmental factors, such as parental speech input and socio-economic status, in complex ways.
One of the strengths of twin studies is their ability to control for shared environmental factors, which can confound interpretations of heritability. By comparing the similarity of SSDs in twins raised together versus those raised apart, researchers can disentangle the effects of genes from those of the shared environment. Studies have shown that while shared environmental factors do play a role, particularly in early childhood, their influence diminishes as children grow older. This suggests that genetic factors become more prominent in the persistence of SSDs over time. For instance, a longitudinal twin study by Tomblin et al. (2004) found that genetic influences on speech sound production became more pronounced as children transitioned from preschool to school age.
Despite their contributions, twin studies on SSD heritability are not without limitations. One challenge is the relatively small sample sizes often used in these studies, which can limit statistical power and generalizability. Additionally, twin studies assume that the environment of monozygotic and dizygotic twins is equally similar, which may not always hold true. For example, parents might treat identical twins more similarly than fraternal twins, potentially inflating estimates of genetic influence. To address these limitations, researchers often complement twin studies with other methodologies, such as adoption studies and genome-wide association studies (GWAS), to triangulate evidence of genetic involvement in SSDs.
In conclusion, twin studies have been pivotal in establishing the heritability of speech sound disorders, consistently demonstrating that genetic factors play a significant role in their development. While environmental influences are also important, particularly in early childhood, the higher concordance rates in monozygotic twins compared to dizygotic twins underscore the genetic basis of SSDs. These findings have important implications for clinical practice, suggesting that early identification of genetic risk factors could lead to more targeted interventions. However, ongoing research is needed to identify specific genes associated with SSDs and to understand how genetic and environmental factors interact to shape speech sound development.
Unveiling the Mystery: How Bats Generate Ultrasonic Sound Waves
You may want to see also
Frequently asked questions
No, speech sound disorders are not solely genetic. While genetic factors can play a role, environmental, developmental, and neurological factors also contribute to their development.
Yes, there is evidence that some speech sound disorders, such as childhood apraxia of speech, may have a genetic component and can run in families.
Not necessarily. While there may be a genetic predisposition, the presence of a speech sound disorder in a parent does not guarantee their child will develop one.
No, not all types are linked to genetics. Some, like articulation disorders, are often influenced by environmental factors, while others, like phonological disorders, may have a genetic component.
Currently, genetic testing cannot definitively predict speech sound disorders, as they are often multifactorial and influenced by both genetic and environmental factors.