Assessing lung sounds is a critical skill in clinical practice, providing valuable insights into respiratory health and aiding in the diagnosis of various pulmonary conditions. By using a stethoscope, healthcare professionals can auscultate different regions of the lungs to detect normal and abnormal breath sounds, such as wheezes, crackles, or rhonchi. Proper technique involves ensuring a quiet environment, positioning the patient comfortably, and systematically listening to all lung fields. Understanding the characteristics of lung sounds, their location, and their timing in the respiratory cycle helps differentiate between conditions like asthma, pneumonia, or chronic obstructive pulmonary disease (COPD). Mastery of this skill enhances diagnostic accuracy and guides appropriate patient management.
| Characteristics | Values |
|---|---|
| Preparation | Ensure patient is seated or semi-reclined; expose chest area; use stethoscope. |
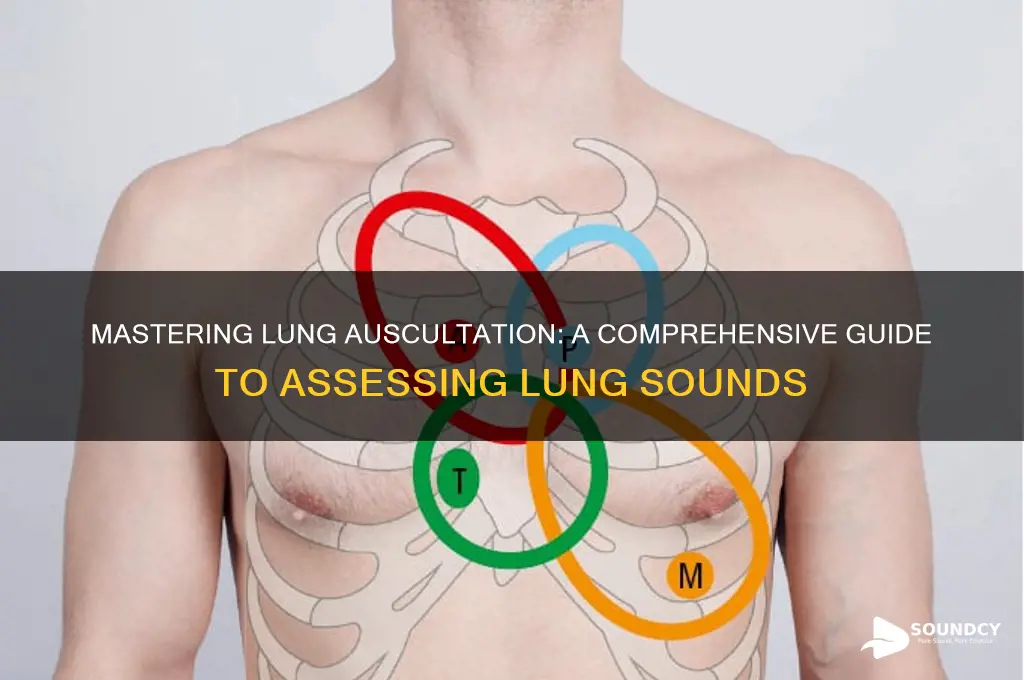
| Location | Assess all lung fields: anterior, posterior, lateral, and axillary regions. |
| Breath Sounds | Normal: Vesicular (soft inspiration, longer expiration). |
| Abnormal: Crackles, wheezes, rhonchi, stridor, diminished/absent sounds. | |
| Crackles | Brief, discontinuous sounds; heard during inspiration; indicate fluid/infection. |
| Wheezes | High-pitched, continuous sounds; heard during expiration; indicate airway obstruction. |
| Rhonchi | Low-pitched, rattling sounds; heard during inspiration/expiration; indicate mucus/secretions. |
| Stridor | High-pitched, musical sound; heard during inspiration; indicates upper airway obstruction. |
| Diminished Sounds | Reduced breath sounds; indicate air trapping, pneumothorax, or consolidation. |
| Absent Sounds | No breath sounds; indicate pneumothorax, pleural effusion, or obstruction. |
| Technique | Place stethoscope firmly on skin; listen during quiet breathing; compare sides. |
| Duration | Assess for at least 30 seconds per lung field. |
| Documentation | Record location, type, and intensity of sounds; note symmetry between sides. |
| Environmental Factors | Ensure quiet room; ask patient to breathe normally; avoid talking during assessment. |
| Patient Positioning | May need to reposition for posterior/lateral fields (e.g., patient leaning forward). |
| Frequency | Repeat assessment if clinical condition changes or as per medical protocol. |
Explore related products






What You'll Learn
- Preparation: Ensure patient comfort, quiet environment, and proper stethoscope placement for accurate lung sound assessment
- Normal Breath Sounds: Identify vesicular, bronchovesicular, and bronchial sounds in different lung regions
- Adventitious Sounds: Recognize crackles, wheezes, rhonchi, and stridor as abnormal lung sound indicators
- Assessment Techniques: Use systematic auscultation, comparing bilateral lung fields for consistency or discrepancies
- Documentation: Record findings clearly, noting sound type, location, intensity, and patient position during assessment
![]()
Preparation: Ensure patient comfort, quiet environment, and proper stethoscope placement for accurate lung sound assessment
Before beginning a lung sound assessment, it is crucial to prioritize the patient's comfort to ensure cooperation and minimize anxiety. Position the patient in a relaxed posture, such as sitting upright or reclining slightly, depending on their preference and medical condition. Ensure the room temperature is comfortable, and offer additional support like pillows or blankets if needed. Explain the procedure clearly and calmly to alleviate any concerns, as a relaxed patient will facilitate a more accurate assessment. Comfort is key, as tension or discomfort can alter breathing patterns and affect the sounds you hear.
Creating a quiet environment is essential for accurately assessing lung sounds, as ambient noise can interfere with your ability to discern subtle auditory cues. Choose a room with minimal background noise, and ask others to keep conversations to a minimum. Turn off any unnecessary equipment or devices that may produce sounds. If the environment is noisy, consider using a sound-insulated room or scheduling the assessment during quieter hours. A silent setting allows you to focus solely on the lung sounds, ensuring a thorough and precise evaluation.
Proper stethoscope placement is critical for an accurate lung sound assessment. Begin by inspecting the stethoscope for any damage or debris, ensuring the earpieces fit snugly and the diaphragm and bell are clean. Position yourself at the patient's side or front, depending on the lung area being assessed. Place the stethoscope's diaphragm (for high-pitched sounds) or bell (for low-pitched sounds) firmly against the skin, avoiding clothing or jewelry that could muffle sounds. Ensure a tight seal to prevent air leaks, which can distort the auscultated sounds. Move systematically across the lung fields, listening to each area for a complete assessment.
When positioning the stethoscope, follow an anatomical approach to cover all lung segments. Start at the apex of the lung, near the shoulder, and move downward to the base, located at the back and sides of the chest. Pay attention to key areas such as the trachea, axillae, and scapulae, as these regions can provide important auditory clues. Ensure the patient takes slow, deep breaths during the assessment, as this enhances the clarity of lung sounds. Proper placement and technique will enable you to detect normal and abnormal sounds, such as crackles, wheezes, or diminished breath sounds, which are vital for diagnosis.
Finally, maintain a systematic and patient-centered approach throughout the preparation and assessment. Double-check that the patient remains comfortable and understands the process, as this fosters cooperation. Confirm the environment is quiet and the stethoscope is correctly placed before beginning. A well-prepared assessment not only ensures accurate results but also builds trust with the patient. By prioritizing comfort, minimizing noise, and mastering stethoscope placement, you can conduct a thorough lung sound evaluation that supports effective clinical decision-making.
Understanding the Unique Characteristics of the American Accent
You may want to see also
Explore related products






![]()
Normal Breath Sounds: Identify vesicular, bronchovesicular, and bronchial sounds in different lung regions
Assessing normal breath sounds is a critical skill in auscultation, allowing healthcare providers to differentiate between healthy lung function and potential respiratory issues. Normal breath sounds are categorized into three main types: vesicular, bronchovesicular, and bronchial, each with distinct characteristics and typical locations within the lung regions. Understanding these sounds is essential for accurate lung assessment.
Vesicular breath sounds are the soft, low-pitched sounds heard during inspiration, with a shorter and quieter expiratory phase. These sounds are best heard over the peripheral lung fields, such as the bases, mid-zones, and periphery of the lungs. Vesicular breathing is the most common sound in healthy adults and is characterized by its gentle, rustling quality, akin to the sound of air moving through leaves. The inspiratory phase is longer and more prominent than the expiratory phase, which is barely audible. This pattern is typical in areas where air moves through smaller airways and alveoli, such as the alveolar regions of the lungs.
Bronchovesicular breath sounds are intermediate in pitch and intensity, blending the qualities of vesicular and bronchial sounds. They are heard over the central lung fields, particularly the upper lobe areas near the tracheal bifurcation, such as the second and third intercostal spaces anteriorly. Bronchovesicular sounds have a slightly louder and higher-pitched quality compared to vesicular sounds, with inspiration and expiration phases of roughly equal duration. This balance occurs because these areas have a mix of larger and smaller airways, creating a sound that is neither purely vesicular nor bronchial.
Bronchial breath sounds are high-pitched and loud, with a prominent expiratory phase that is often longer than inspiration. These sounds are normally heard over the trachea but can also be auscultated over the bronchi in the lung fields, such as the suprasternal notch and the back between the scapulae. Bronchial breathing has a hollow, tubular quality, similar to the sound of breathing through a pipe. In healthy individuals, bronchial sounds are confined to the larger airways, but their presence in peripheral lung fields may indicate pathology, such as consolidation or fluid in the alveoli.
To accurately identify these sounds, use a stethoscope and listen systematically across the lung regions. Begin by comparing sounds between corresponding areas on the right and left sides to ensure symmetry. Note the pitch, intensity, and duration of inspiratory and expiratory phases. Vesicular sounds should dominate in the peripheral fields, bronchovesicular sounds in the central fields, and bronchial sounds over the trachea. Familiarity with these normal patterns is crucial for detecting abnormalities during lung assessments.
In summary, mastering the identification of vesicular, bronchovesicular, and bronchial breath sounds in their respective lung regions is fundamental to auscultation. Vesicular sounds are soft and low-pitched in peripheral fields, bronchovesicular sounds are intermediate in central fields, and bronchial sounds are loud and high-pitched over the trachea. Recognizing these normal patterns enables healthcare providers to distinguish healthy lung function from pathological conditions, ensuring accurate diagnosis and timely intervention.
Renting Sound Boards: A Practical Option for Events and Productions?
You may want to see also
Explore related products






![]()
Adventitious Sounds: Recognize crackles, wheezes, rhonchi, and stridor as abnormal lung sound indicators
Adventitious lung sounds are abnormal breath sounds that indicate underlying respiratory conditions. These sounds, including crackles, wheezes, rhonchi, and stridor, are crucial to identify during a lung assessment as they provide valuable insights into the patient's pulmonary health. Recognizing these sounds requires a systematic approach and a keen ear, often aided by a stethoscope. When auscultating the lungs, it's essential to listen for these abnormal sounds, as they can be indicative of various pathologies, from infections to chronic respiratory diseases.
Crackles are one of the most common adventitious sounds and are often described as brief, discontinuous, and popping noises. They are typically heard during inspiration and can be fine or coarse. Fine crackles are soft, high-pitched, and very brief, often heard in patients with conditions like pneumonia or pulmonary fibrosis. Coarse crackles, on the other hand, are louder and lower in pitch, commonly associated with conditions such as congestive heart failure or bronchiectasis. These sounds are caused by the sudden opening of small airways or alveoli, often due to fluid or mucus.
Wheezes are high-pitched, continuous sounds that occur during both inspiration and expiration. They resemble a whistling noise and are typically indicative of airway obstruction or narrowing. Asthma, chronic obstructive pulmonary disease (COPD), and bronchitis are common conditions associated with wheezing. The pitch and intensity of wheezes can vary, with higher-pitched sounds suggesting more proximal airway obstruction.
Rhonchi are low-pitched, snoring-like sounds that are continuous and can be heard during both inhalation and exhalation. These sounds are often described as rattling and are caused by the vibration of mucus or secretions in the larger airways. Rhonchi are commonly associated with conditions that produce excessive mucus, such as chronic bronchitis or cystic fibrosis. The presence of rhonchi may indicate the need for airway clearance techniques or further investigation into the underlying cause.
Stridor is a high-pitched, musical sound that is usually heard during inspiration, but can sometimes be present during expiration as well. It is often described as a harsh, vibrating noise and is a sign of upper airway obstruction. Stridor can be a medical emergency, as it may indicate a severe narrowing of the airway, potentially caused by conditions like epiglottitis, foreign body aspiration, or vocal cord dysfunction. Immediate medical attention is required when stridor is detected.
In summary, adventitious lung sounds are vital indicators of respiratory health. Crackles, wheezes, rhonchi, and stridor each have distinct characteristics and are associated with specific respiratory conditions. Healthcare professionals must be adept at recognizing these sounds to facilitate accurate diagnoses and timely interventions. Auscultation skills, combined with a comprehensive understanding of these abnormal lung sounds, are essential tools for assessing and managing patients with respiratory disorders.
Does AirTag Make Sound? Exploring Apple's Tracking Device Features
You may want to see also
Explore related products






![]()
Assessment Techniques: Use systematic auscultation, comparing bilateral lung fields for consistency or discrepancies
When assessing lung sounds, systematic auscultation is a cornerstone technique that ensures a thorough and accurate evaluation. Begin by positioning the patient comfortably, typically in a seated or supine position, to allow for easy access to all lung fields. Use a stethoscope with proper ear placement to maximize sound clarity. Divide the chest into specific regions: the anterior, posterior, and lateral lung fields. Start auscultation in a systematic manner, typically from the apex of the lung (near the shoulder) moving downward to the base (near the diaphragm). This methodical approach ensures that no area is overlooked and provides a structured framework for comparison.
During auscultation, focus on comparing bilateral lung fields to identify consistency or discrepancies. Listen to corresponding areas on both the left and right sides of the chest, such as the upper, middle, and lower lung zones. Normal lung sounds, including bronchial, vesicular, and bronchovesicular sounds, should be symmetrical between the two sides. Pay attention to the intensity, pitch, and quality of the sounds. For example, vesicular breathing should be soft and low-pitched, while bronchial breathing is louder and higher-pitched. Discrepancies, such as unilateral wheezing, crackles, or diminished breath sounds, may indicate pathology and warrant further investigation.
To enhance accuracy, ensure the patient is breathing normally and deeply during auscultation. Instruct them to inhale and exhale fully, as this allows for better detection of abnormal sounds. Be mindful of environmental noise that could interfere with your assessment, and reposition the stethoscope diaphragm or bell as needed to capture both high- and low-frequency sounds. The diaphragm is more effective for higher-pitched sounds, while the bell is better suited for lower-pitched sounds like crackles or whispered pectoriloquy.
Systematic auscultation also involves noting the timing and location of abnormal sounds. For instance, crackles that occur at the beginning of inspiration may suggest different conditions compared to those heard at the end. Similarly, localized wheezing in one lung field could indicate an obstructive process, such as asthma or a foreign body. Documenting these findings in a structured manner, such as by lung zone, helps in creating a clear clinical picture and aids in differential diagnosis.
Finally, integrate the auscultation findings with other assessment data, such as the patient’s history, symptoms, and physical exam observations. For example, a patient with a history of smoking and unilateral diminished breath sounds may require further imaging to rule out chronic obstructive pulmonary disease (COPD) or lung cancer. Systematic auscultation, when combined with a comparative approach, not only identifies abnormalities but also guides the next steps in patient care, ensuring a comprehensive and patient-centered evaluation.
Sound Machines: Safe Sleep Aid for Babies?
You may want to see also
Explore related products






![]()
Documentation: Record findings clearly, noting sound type, location, intensity, and patient position during assessment
When documenting lung sounds, clarity and precision are essential to ensure accurate communication of findings. Begin by noting the type of sound heard, such as normal breath sounds (vesicular or bronchovesicular), adventitious sounds (wheezes, crackles, rhonchi, or stridor), or absent breath sounds. Clearly describe the characteristics of the sound, such as whether crackles are fine or coarse, or if wheezes are high-pitched or low-pitched. This specificity helps differentiate between various respiratory conditions and guides further clinical decision-making.
Next, document the location where the sound was heard, identifying the specific lung field (e.g., right upper lobe, left lower lobe) or anatomical region (e.g., anterior chest, posterior base). Note if the sound is unilateral, bilateral, or localized to a particular area. Include the intensity of the sound, using descriptive terms such as soft, moderate, or loud, or grading it on a scale (e.g., 1+ to 4+). This provides insight into the severity of the underlying issue and aids in monitoring changes over time.
Record the patient’s position during the assessment, as this can influence the distribution and quality of lung sounds. For example, note if the patient was sitting upright, lying supine, or in a lateral decubitus position. Certain sounds, like crackles, may be more prominent in specific positions, and documenting this detail ensures consistency in future assessments and comparisons.
Include any associated findings that may impact the interpretation of lung sounds, such as the patient’s breathing effort, cough, or visible accessory muscle use. Also, note if the sounds change with different phases of respiration (inspiration or expiration), as this can help differentiate between conditions like asthma (expiratory wheezing) or pulmonary edema (inspiratory crackles).
Finally, ensure the documentation is organized and concise, using a structured format if possible. For example, you might use a table or bullet points to list the sound type, location, intensity, and patient position for each lung field. This approach enhances readability and ensures that critical information is easily accessible for other healthcare providers. Consistent and detailed documentation is vital for tracking progress, informing treatment plans, and maintaining continuity of care.
Do Plants Communicate Through Sound? Unveiling Nature's Hidden Language
You may want to see also
Frequently asked questions
The basic lung sounds include normal breath sounds (vesicular and bronchovesicular), adventitious sounds (wheezes, crackles, rhonchi, and stridor), and absent or decreased breath sounds. Vesicular sounds are soft and rustling, while bronchovesicular sounds are slightly louder. Adventitious sounds indicate potential respiratory issues.
Place the stethoscope’s diaphragm (flat side) on the patient’s chest for low-pitched sounds and the bell (open side) for high-pitched sounds. Listen systematically across all lung fields (anterior, posterior, and lateral) during both inspiration and expiration, ensuring a quiet environment for accurate assessment.
Crackles are discontinuous, bubbling sounds often heard in patients with fluid in the lungs (e.g., pneumonia or heart failure). Wheezes are high-pitched, continuous sounds typically associated with narrowed airways, such as in asthma or chronic obstructive pulmonary disease (COPD).
Normal lung sounds are consistent, soft, and clear throughout the lung fields. Abnormal sounds include wheezes, crackles, rhonchi, or stridor, which may indicate conditions like asthma, pneumonia, or airway obstruction. Absent or decreased sounds can suggest pneumothorax or fluid accumulation. Always compare both sides for asymmetry.