Assessing breathing sounds is a critical skill in clinical practice, as it provides valuable insights into a patient’s respiratory health. By auscultating lung sounds using a stethoscope, healthcare professionals can identify normal breath sounds, such as vesicular and bronchial breathing, or detect abnormal findings like wheezes, crackles, rhonchi, and stridor. These sounds often indicate underlying conditions, such as asthma, pneumonia, chronic obstructive pulmonary disease (COPD), or heart failure. Proper assessment involves systematic listening across lung fields, noting pitch, intensity, timing, and location of sounds, while considering the patient’s medical history and symptoms. Mastery of this technique enables early diagnosis, targeted treatment, and improved patient outcomes.
Explore related products






What You'll Learn
- Use of Stethoscope: Proper placement and technique for auscultation to hear lung sounds clearly
- Types of Breath Sounds: Identify normal, abnormal, and adventitious sounds like wheezes or crackles
- Assessment Locations: Key chest areas to listen for specific lung sounds accurately
- Patient Positioning: Optimal positions for assessing anterior, posterior, and lateral lung fields
- Documentation Standards: Recording findings clearly, noting symmetry, intensity, and abnormalities in breathing sounds
![]()
Use of Stethoscope: Proper placement and technique for auscultation to hear lung sounds clearly
To effectively assess breathing sounds using a stethoscope, proper placement and technique are crucial. Begin by ensuring the patient is in a comfortable position, either sitting upright or lying down, as this allows for optimal lung expansion. The stethoscope should be held with the diaphragm (the larger side) or the bell (the smaller side) firmly against the skin, creating a tight seal to minimize ambient noise. Start by placing the stethoscope on the anterior chest wall, specifically over the trachea, to listen for normal or abnormal breath sounds such as stridor or stertor, which can indicate upper airway issues. Gradually move to other areas to assess lung sounds comprehensively.
When auscultating lung sounds, systematically cover all lung fields, including the anterior, posterior, and lateral chest walls. For the anterior chest, place the stethoscope at the second, fourth, and sixth intercostal spaces on both the right and left sides. For the posterior chest, focus on the scapular regions and the bases of the lungs, as these areas are prone to accumulating fluid or mucus. Ensure the patient takes slow, deep breaths during auscultation to capture both inspiratory and expiratory phases clearly. The diaphragm is generally used for adult patients to hear higher-pitched sounds, while the bell is ideal for detecting lower-pitched sounds, such as crackles or wheezes.
Proper technique also involves minimizing external noise and ensuring the stethoscope is not rubbing against clothing or jewelry. Keep the tubing free from kinks or twists, as this can interfere with sound transmission. When moving the stethoscope, do so gently to avoid creating friction sounds that could be mistaken for lung sounds. Additionally, maintain consistent pressure on the stethoscope to ensure a steady acoustic seal. If using an electronic stethoscope, adjust the volume and frequency settings as needed to enhance clarity.
To differentiate between normal and abnormal lung sounds, familiarize yourself with the characteristics of each. Normal breath sounds are soft and consistent, with inspiration slightly longer than expiration. Wheezes, crackles, and rhonchi are common abnormal sounds that indicate conditions such as asthma, pneumonia, or chronic obstructive pulmonary disease (COPD). Practice and experience are key to distinguishing these sounds accurately. Always compare findings between corresponding lung fields to identify asymmetries, which can be clinically significant.
Finally, document your findings clearly, noting the location, intensity, and quality of the sounds heard. For example, describe wheezes as "high-pitched, musical sounds heard during expiration" and crackles as "brief, discontinuous sounds heard during inspiration." This detailed documentation aids in diagnosis and monitoring of respiratory conditions. By mastering proper stethoscope placement and auscultation techniques, healthcare providers can effectively assess breathing sounds and contribute to accurate patient care.
Dahmer's Whale Sounds: A Disturbing Connection?
You may want to see also
Explore related products






![]()
Types of Breath Sounds: Identify normal, abnormal, and adventitious sounds like wheezes or crackles
Breath sounds are an essential component of respiratory assessment, providing valuable insights into a patient's lung health. Understanding the different types of breath sounds is crucial for healthcare professionals to identify normal, abnormal, and adventitious sounds that may indicate underlying respiratory conditions. Normal breath sounds are typically soft, gentle, and consistent, with a smooth airflow during both inspiration and expiration. These sounds are often described as vesicular, which are low-pitched and heard throughout the chest wall. They are characterized by a longer inspiratory phase compared to the expiratory phase and are best heard using a stethoscope with the diaphragm placed lightly on the chest.
Abnormal breath sounds, on the other hand, deviate from the typical vesicular pattern and may indicate respiratory distress or disease. One common abnormal breath sound is bronchial breathing, which is louder and higher-pitched than normal. This sound is often heard over the trachea and mainstem bronchi and can be a sign of consolidation, such as pneumonia or pulmonary edema. Another abnormal breath sound is bronchovesicular, which is a mix of vesicular and bronchial sounds, often heard in areas where the lungs are thicker or more consolidated. These sounds may indicate conditions like chronic obstructive pulmonary disease (COPD) or asthma.
Adventitious breath sounds are additional sounds that are not normally present and can be indicative of specific respiratory conditions. Wheezes are high-pitched, whistling sounds that occur due to narrowed or obstructed airways. They are typically heard during expiration but can also be present during inspiration. Wheezes are commonly associated with asthma, COPD, or bronchitis. Crackles, also known as rales, are another type of adventitious sound characterized by brief, popping noises that result from fluid in the small airways or alveoli. Crackles can be fine or coarse and are often heard in patients with conditions like pneumonia, heart failure, or interstitial lung disease.
Identifying and differentiating between these breath sounds require careful auscultation and a systematic approach. Healthcare providers should listen to various lung fields, comparing the sounds between different areas. The use of both the diaphragm and bell of the stethoscope can help capture a range of frequencies. For instance, the diaphragm is more sensitive to higher-pitched sounds like wheezes, while the bell can better detect lower-pitched sounds such as crackles. It is also essential to assess the intensity, duration, and timing of these sounds in relation to the respiratory cycle.
In summary, assessing breath sounds is a critical skill for healthcare professionals to detect respiratory abnormalities. By recognizing the characteristics of normal, abnormal, and adventitious sounds, clinicians can make informed decisions about patient care. Wheezes and crackles, as adventitious sounds, provide specific clues to the nature of the respiratory issue. Proper auscultation techniques and a thorough understanding of breath sound variations are key to accurate diagnosis and subsequent treatment planning. This knowledge enables timely interventions and improved patient outcomes in respiratory care.
Understanding Non-Diegetic Sounds in Media
You may want to see also
Explore related products






![]()
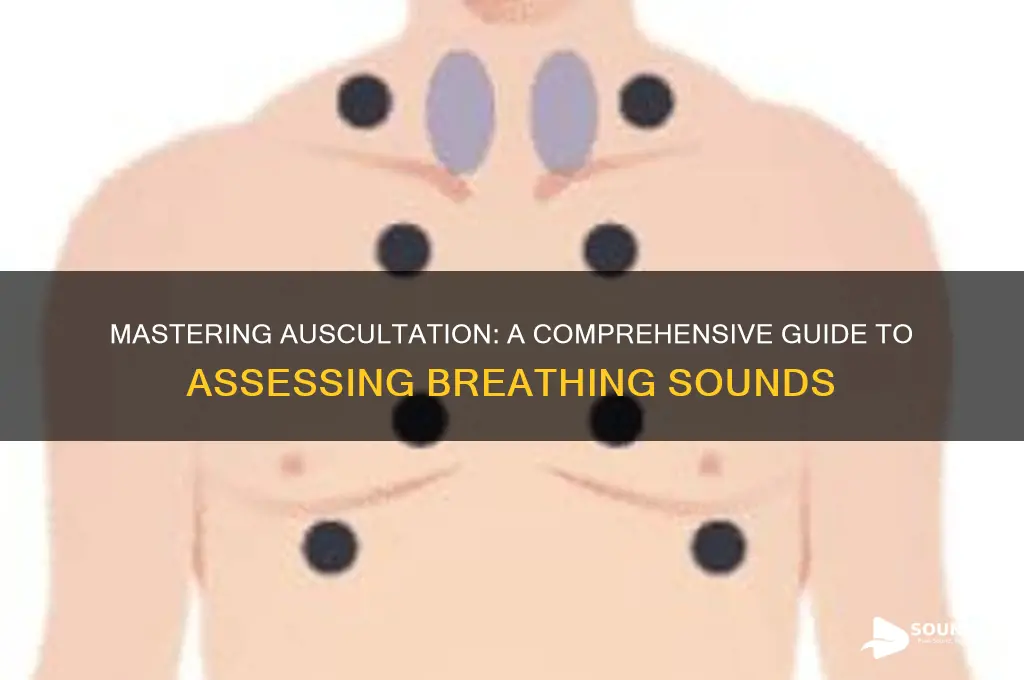
Assessment Locations: Key chest areas to listen for specific lung sounds accurately
When assessing breathing sounds, it is crucial to focus on specific chest areas to accurately identify and interpret lung sounds. The chest wall is divided into several anatomical regions, each corresponding to different lung segments. Proper placement of the stethoscope on these key areas ensures a comprehensive evaluation of respiratory function. The primary locations for auscultation include the anterior chest, posterior chest, and lateral chest. Each area provides unique insights into the airflow and potential abnormalities within the lungs.
The anterior chest is typically assessed with the patient in a seated or supine position. Key areas include the tracheal region, located over the sternum, which helps detect stridor or abnormal tracheal sounds. The upper anterior chest (second intercostal spaces) and lower anterior chest (sixth intercostal spaces) are also important. These regions correspond to the upper and lower lobes of the lungs, respectively, and are ideal for listening to breath sounds such as vesicular breathing or adventitious sounds like wheezes or crackles. Proper placement of the stethoscope on these areas is essential to avoid artifactual sounds from clothing or improper contact.
The posterior chest is assessed with the patient in an upright or seated position, and it provides access to the lung bases and lower lobes. Key locations include the scapular regions (between the scapulae) and the infrascapular regions (below the scapulae). These areas are critical for detecting basal crackles, which may indicate conditions like pneumonia or congestive heart failure. The posterior axillary lines (fourth to sixth intercostal spaces) are also important, as they allow for auscultation of the lung bases and detection of sounds like wheezing or diminished breath sounds.
The lateral chest is often overlooked but is vital for assessing the middle lobes and lingula. With the patient in a seated or supine position, place the stethoscope on the midclavicular lines (fifth intercostal spaces) and anterior axillary lines (fourth intercostal spaces). These areas help identify sounds such as bronchial breathing or adventitious sounds that may indicate consolidation or obstruction. Proper patient positioning, such as having them lean forward slightly, can enhance sound clarity in these regions.
Lastly, the apical regions of the lungs, located just above the clavicles, are important for detecting high-pitched sounds like wheezes or diminished breath sounds. These areas are best assessed with the patient’s head slightly tilted backward and the stethoscope placed lightly on the skin. Each of these assessment locations requires precise stethoscope placement and patient cooperation to ensure accurate auscultation. By systematically evaluating these key chest areas, healthcare providers can effectively identify respiratory abnormalities and guide appropriate clinical interventions.
Hearing the Unseen: A Schizophrenic's Auditory World Explored
You may want to see also
Explore related products






![]()
Patient Positioning: Optimal positions for assessing anterior, posterior, and lateral lung fields
When assessing breathing sounds, proper patient positioning is crucial to ensure accurate auscultation of the anterior, posterior, and lateral lung fields. For the anterior lung fields, the patient should be positioned in a seated or semi-recumbent position. This allows the clinician to easily access the front of the chest, including the upper and lower lobes. The patient should sit upright with their arms resting comfortably at their sides, ensuring the chest wall is fully exposed. This position helps to relax the chest muscles and facilitates the detection of breath sounds, wheezes, or crackles in the anterior regions.
To assess the posterior lung fields, the patient should be positioned in a seated or upright position, preferably leaning slightly forward. This positioning allows the clinician to auscultate the back of the chest, including the lower lobes and the bases of the lungs. The patient can sit on the edge of the bed or in a chair, leaning forward with their arms resting on a table or their lap. This posture helps to separate the scapulae, providing better access to the posterior lung fields. Encouraging the patient to take slow, deep breaths during auscultation enhances the clarity of the breath sounds.
For evaluating the lateral lung fields, the patient should be positioned in a seated or standing position, with the arm on the side being assessed raised above the head or resting on the clinician’s shoulder. This position exposes the lateral chest wall, allowing for optimal auscultation of the mid-axillary and lateral lung regions. If the patient is unable to stand, they can be seated with the arm supported to maintain the chest wall in a relaxed and accessible position. This positioning is particularly important for detecting abnormalities in the middle lobes or lateral segments of the lungs.
In cases where the patient is unable to sit or stand, supine or lateral decubitus positions can be utilized. For supine positioning, the clinician can auscultate the anterior lung fields directly. If assessing the posterior or lateral fields in a supine patient, the clinician may need to gently turn the patient’s head or body to expose the desired area. However, seated or upright positions are generally preferred as they provide better lung expansion and clearer breath sounds.
Lastly, it is essential to ensure the patient is comfortable and relaxed during positioning, as tension can alter breath sounds. Clear communication and reassurance can help the patient cooperate, allowing for a more accurate assessment. Always adjust the positioning as needed to accommodate the patient’s mobility, comfort, or medical condition while maintaining access to the lung fields being evaluated. Proper positioning not only enhances the accuracy of auscultation but also ensures a thorough assessment of all lung regions.
Exploring the Diverse Sound Effects in Super Smash Bros. Ultimate
You may want to see also
Explore related products






![]()
Documentation Standards: Recording findings clearly, noting symmetry, intensity, and abnormalities in breathing sounds
When documenting breathing sound assessments, clarity and precision are paramount to ensure accurate communication of findings. Begin by noting the patient’s position during the assessment (e.g., sitting, supine) and the auscultation sites examined, such as the anterior, posterior, and lateral chest walls. Clearly state whether the breathing sounds are symmetric between the left and right sides, as asymmetry may indicate underlying pathology. For example, document: "Breathing sounds symmetric bilaterally" or "Decreased breath sounds noted over the right lower lobe compared to the left." This establishes a baseline for comparison and highlights potential areas of concern.
Intensity of breathing sounds should be recorded using standardized descriptors such as normal, increased, or decreased. Specify the nature of the intensity, such as "Vesicular breath sounds of normal intensity heard throughout" or "Bronchial breath sounds of increased intensity over the left upper lobe." If adventitious sounds are present, describe their characteristics, including their timing (e.g., inspiratory, expiratory, or bilateral), quality (e.g., wheezes, crackles, rhonchi), and grade (e.g., soft, moderate, loud). For instance, document: "Fine crackles heard at the right lung base during late inspiration" or "Expiratory wheezes noted bilaterally, more prominent on the left."
Abnormalities in breathing sounds must be documented with specificity to guide further diagnostic and therapeutic interventions. Note any absence of sounds, such as "Absent breath sounds over the left lower lobe," which may suggest pneumothorax or fluid accumulation. Describe the distribution of abnormalities, such as "Scattered rhonchi throughout all lung fields" or "Localized wheezing in the right middle lobe." If the patient’s breathing pattern is abnormal, such as labored breathing or use of accessory muscles, include this in the documentation, as it provides context for the auscultation findings.
Consistency in documentation is critical for longitudinal care. Use consistent terminology and avoid vague descriptions. For example, instead of "Sounds are abnormal," specify: "Coarse crackles heard in the bilateral lung bases, more pronounced on the right." Include any changes from previous assessments, such as: "Breath sounds previously decreased in the left lower lobe are now clear and equal bilaterally." This ensures continuity and allows for accurate tracking of the patient’s respiratory status over time.
Finally, conclude the documentation with a summary statement that ties the findings together and highlights clinical significance. For instance: "Breathing sounds symmetric with normal vesicular intensity and no adventitious sounds noted" or "Asymmetric breath sounds with decreased intensity and fine crackles in the right lower lobe, suggestive of possible pneumonia." This provides a concise overview for other healthcare providers and aids in decision-making. Adhering to these documentation standards ensures that breathing sound assessments are recorded clearly, comprehensively, and in a manner that supports patient care.
Do MSI Monitors Have Built-In Speakers? A Comprehensive Guide
You may want to see also
Frequently asked questions
The primary techniques include auscultation (listening with a stethoscope), palpation (feeling vibrations), and observation (noting visible chest movements and effort).
Normal breath sounds include bronchial and vesicular sounds, while abnormal sounds include wheezes, crackles, stridor, and rhonchi, each indicating different respiratory conditions.
Crackles are fine, rattling sounds often heard during inhalation, associated with fluid or mucus in the airways. Wheezes are high-pitched, whistling sounds typically heard during exhalation, indicating airway narrowing or obstruction.