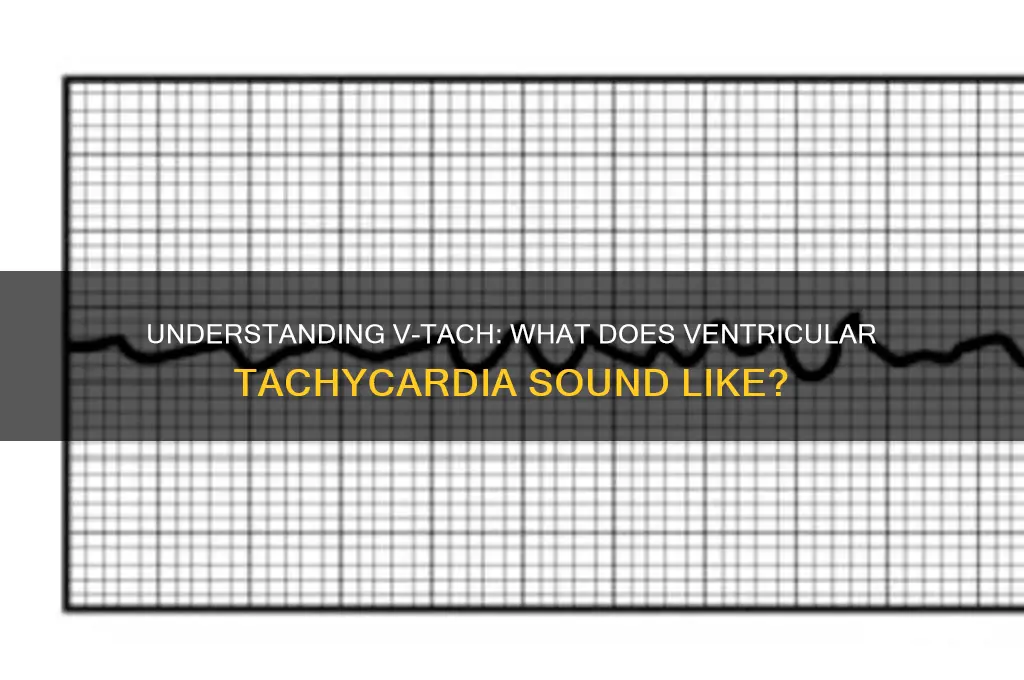
Ventricular tachycardia (VTach) is a life-threatening cardiac arrhythmia characterized by rapid, irregular heartbeats originating in the ventricles, the heart's lower chambers. When auscultating VTach, the rhythm is typically fast, ranging from 100 to 250 beats per minute, and often lacks the normal P waves seen in a healthy ECG. The sound of VTach is distinct, with a rapid, chaotic rhythm that may be described as a series of quick, uneven thumps rather than the steady, regular beat of a normal heartbeat. This abnormal rhythm can be detected through a stethoscope or ECG, and its identification is crucial for prompt medical intervention, as VTach can quickly deteriorate into ventricular fibrillation or cardiac arrest if left untreated.
| Characteristics | Values |
|---|---|
| Rhythm | Regular or irregular, depending on the type of V-Tach (monomorphic/polymorphic) |
| Rate | Typically 100-250 beats per minute (bpm) |
| QRS Complex | Wide (>0.12 seconds), often bizarre or distorted shape |
| P Waves | Absent or dissociated from QRS complexes |
| Heart Sounds | May be absent or weak due to ineffective cardiac output |
| Duration | Can be sustained (lasting >30 seconds) or nonsustained (<30 seconds) |
| Associated Symptoms | Dizziness, palpitations, syncope, or sudden cardiac arrest |
| ECG Appearance | Rapid, wide QRS complexes without a discernible P wave |
| Causes | Myocardial ischemia, cardiomyopathy, electrolyte imbalances, or genetic disorders |
| Treatment | Defibrillation, antiarrhythmic drugs (e.g., amiodarone), or ICD placement |
| Prognosis | Life-threatening if untreated; survival depends on prompt intervention |
Explore related products






What You'll Learn
- Rhythm Characteristics: Irregular, wide QRS complexes, no P waves, chaotic electrical activity
- Heart Rate Range: Typically 100-250 beats per minute, often sustained and life-threatening
- Clinical Presentation: Sudden onset, dizziness, palpitations, unconsciousness, or cardiac arrest
- Differential Diagnosis: Distinguish from SVT with aberrancy, PVCs, or atrial fibrillation
- Treatment Options: Immediate defibrillation, antiarrhythmics, or cardioversion to restore normal rhythm
![]()
Rhythm Characteristics: Irregular, wide QRS complexes, no P waves, chaotic electrical activity
Ventricular tachycardia (VTach) is a life-threatening arrhythmia characterized by a distinct set of rhythm characteristics that are crucial for identification. One of the hallmark features is the irregularity of the rhythm. Unlike the predictable pattern of a normal sinus rhythm, VTach presents as a chaotic and disorganized sequence of heartbeats. This irregularity is a direct result of the ventricles generating their own electrical impulses at a rapid and uncontrolled rate, often exceeding 100 beats per minute. The absence of a consistent pattern makes it challenging for the heart to pump blood effectively, leading to hemodynamic instability.
Another defining characteristic of VTach is the presence of wide QRS complexes. In a normal ECG, the QRS complex typically measures less than 0.12 seconds, reflecting the coordinated depolarization of the ventricles. In VTach, the QRS complexes are significantly widened, often exceeding 0.12 seconds, due to the abnormal conduction pathways originating from the ventricles rather than the sinoatrial (SA) node. This widening is a critical indicator of ventricular origin and distinguishes VTach from supraventricular tachycardias. The morphology of these wide QRS complexes may vary but is consistently abnormal, further emphasizing the chaotic nature of the rhythm.
The absence of P waves is another key feature of VTach. In a normal ECG, P waves represent the depolarization of the atria and are typically visible before each QRS complex. In VTach, the atria are often not involved in the rhythm, and their electrical activity is either dissociated from the ventricles or completely absent. This dissociation results in no discernible P waves on the ECG, or if present, they are unrelated to the QRS complexes. The lack of P waves underscores the ventricular origin of the arrhythmia and the disorganized electrical activity.
The term chaotic electrical activity aptly describes the overall appearance of VTach on an ECG. The rhythm is not merely fast but also entirely disorganized, with no clear pattern or regularity. This chaos is evident in the irregular intervals between QRS complexes, the varying amplitudes and morphologies of the complexes, and the absence of any coordinated atrial activity. The chaotic nature of VTach reflects the uncontrolled and abnormal electrical impulses originating from the ventricles, which can rapidly deteriorate into ventricular fibrillation if not promptly treated.
In summary, VTach is identified by its irregular rhythm, wide QRS complexes, absence of P waves, and chaotic electrical activity. These characteristics collectively paint a picture of a dangerous arrhythmia that requires immediate intervention. Recognizing these features is essential for healthcare providers to diagnose and manage VTach effectively, as delays in treatment can lead to severe complications, including cardiac arrest. Understanding how VTach "sounds" on an ECG—both visually and in terms of its rhythm characteristics—is critical for timely and accurate identification.
Razer Kraken: Soundproof or Not?
You may want to see also
Explore related products






![]()
Heart Rate Range: Typically 100-250 beats per minute, often sustained and life-threatening
Ventricular tachycardia (VTach) is a life-threatening arrhythmia characterized by a heart rate range typically between 100 and 250 beats per minute. This rapid rate occurs because the ventricles, the heart's main pumping chambers, take over the electrical signaling, bypassing the normal pacemaker function of the sinoatrial node. Unlike a normal heart rhythm, VTach is often sustained, meaning it lasts for more than 30 seconds or requires intervention to terminate. This sustained nature is what makes it particularly dangerous, as it can lead to hemodynamic instability, where the heart is unable to pump enough blood to meet the body's needs.
When listening to VTach through a stethoscope or analyzing it on an electrocardiogram (ECG), the rhythm is notably irregular and chaotic. The heart sounds may be difficult to discern due to the rapid and uncoordinated contractions of the ventricles. Instead of the familiar "lub-dub" of a normal heartbeat, VTach often produces a continuous, monotonous sequence of beats without the usual pauses. This is because the ventricles are contracting so rapidly that there is little time for the heart to fill with blood adequately, resulting in diminished cardiac output.
The sound of VTach on an ECG is equally distinctive. It typically shows wide QRS complexes, which are the electrical signals representing ventricular depolarization. These complexes are usually wider than 0.12 seconds and often appear bizarre or distorted in shape. The rhythm is regularly irregular, meaning the intervals between beats are inconsistent, further emphasizing the chaotic nature of the arrhythmia. This pattern is a critical diagnostic feature that differentiates VTach from other tachycardias.
Clinically, VTach is a medical emergency, especially when sustained. Patients may present with symptoms such as palpitations, dizziness, shortness of breath, chest pain, or even loss of consciousness. The rapid heart rate prevents the ventricles from filling properly, leading to reduced blood flow to vital organs, including the brain and coronary arteries. If left untreated, VTach can degenerate into ventricular fibrillation (VFib), a more severe arrhythmia where the ventricles quiver ineffectively, causing immediate cardiac arrest.
Immediate intervention is crucial for managing VTach. In stable patients, antiarrhythmic medications like amiodarone or procainamide may be used to restore a normal rhythm. However, unstable patients—those with hypotension, chest pain, or altered mental status—require urgent electrical cardioversion. This involves delivering an electric shock to the heart to reset its electrical activity. Early recognition of VTach through its characteristic heart rate range and ECG findings is essential for prompt treatment and preventing potentially fatal complications.
Sound Waves and Piezoelectric Crystals: Unlocking Energy Conversion Secrets
You may want to see also
Explore related products






![]()
Clinical Presentation: Sudden onset, dizziness, palpitations, unconsciousness, or cardiac arrest
The clinical presentation of ventricular tachycardia (VTach) is often dramatic and requires immediate attention, as it can rapidly deteriorate into a life-threatening situation. Sudden onset is a hallmark of VTach, with patients typically experiencing an abrupt change in their cardiac rhythm. This sudden onset is usually accompanied by dizziness, which can range from lightheadedness to a profound feeling of faintness. The dizziness occurs due to the heart's inability to pump blood effectively, leading to decreased cerebral perfusion. Patients may describe this sensation as a feeling of "the room spinning" or an overwhelming need to sit or lie down.
Palpitations are another common symptom, where individuals become acutely aware of their heartbeat, often describing it as rapid, irregular, or "fluttering." These palpitations are a direct result of the heart's ventricles contracting at an abnormally high rate, typically between 100 to 250 beats per minute. The sensation can be so intense that it causes anxiety or panic in the patient, further exacerbating their condition. It is crucial for healthcare providers to recognize that the presence of palpitations, especially when combined with other symptoms, should raise suspicion of VTach.
As VTach progresses, the risk of unconsciousness increases significantly. This occurs because the inefficient pumping action of the heart during VTach leads to inadequate blood flow to vital organs, particularly the brain. Unconsciousness may be preceded by symptoms such as confusion, weakness, or a feeling of impending doom. Once unconscious, the patient is at imminent risk of cardiac arrest, where the heart's electrical activity becomes so chaotic that it ceases to pump blood effectively. At this stage, immediate defibrillation and advanced cardiac life support are critical to restore a normal heart rhythm and prevent death.
The sound of VTach on auscultation or via cardiac monitoring is distinct and alarming. Unlike the regular, rhythmic beat of a normal heartbeat, VTach produces a rapid, irregular rhythm that lacks the usual "lub-dub" sounds of the heart valves. Instead, it may sound like a continuous, chaotic thumping or a series of rapid, uneven beats. This abnormal rhythm is often described as "wide and bizarre" on an electrocardiogram (ECG), with QRS complexes that are wider than normal and lacking the P waves seen in a regular sinus rhythm. Recognizing this sound or ECG pattern is crucial for prompt diagnosis and intervention.
In summary, the clinical presentation of VTach is characterized by its sudden onset, accompanied by dizziness, palpitations, and the potential for rapid progression to unconsciousness or cardiac arrest. The distinctive sound of VTach, whether heard through auscultation or visualized on an ECG, serves as a critical diagnostic clue. Healthcare providers must act swiftly to identify and treat VTach, as timely intervention can be the difference between life and death. Understanding these symptoms and their progression is essential for effective management and patient outcomes.
Understanding Consonant Production: The Art of Speech Sound Creation
You may want to see also
Explore related products






![]()
Differential Diagnosis: Distinguish from SVT with aberrancy, PVCs, or atrial fibrillation
When distinguishing Ventricular Tachycardia (VTach) from SVT with aberrancy, PVCs, or atrial fibrillation (AFib), understanding the auditory characteristics and ECG patterns is crucial. VTach typically produces a wide QRS complex (>120 ms) due to its ventricular origin, and the rhythm is often regular and monomorphic. The sound of VTach is characterized by a rapid, uniform heartbeat without the variability seen in other arrhythmias. In contrast, SVT with aberrancy also presents with wide QRS complexes, but the rhythm is typically regular, and the underlying cause is a supraventricular tachycardia with aberrant conduction (e.g., bundle branch block). Listening for a consistent, rapid rhythm without the variability of AFib or the occasional ectopic beats of PVCs can help differentiate VTach from SVT with aberrancy.
PVCs (Premature Ventricular Contractions) are distinguished from VTach by their isolated, premature nature. PVCs are single, wide QRS complexes that disrupt the normal sinus rhythm, often followed by a compensatory pause. The sound of PVCs includes an occasional "skipped beat" or an early, forceful beat, which contrasts with the continuous, rapid rhythm of VTach. In VTach, the wide QRS complexes occur consecutively without a preceding P wave, whereas PVCs are intermittent and not sustained. Recognizing the pattern of isolated ectopy versus sustained ventricular rhythm is key to differentiating these two conditions.
Atrial Fibrillation (AFib) is another important differential diagnosis. AFib is characterized by an irregularly irregular rhythm with chaotic atrial activity, resulting in variably conducted ventricular responses. The sound of AFib is distinctly irregular, with no consistent pattern between heartbeats. In contrast, VTach typically has a regular rhythm, even though it is rapid. Additionally, AFib often presents with narrow QRS complexes unless there is underlying bundle branch block or aberrancy. The absence of a regular, monomorphic ventricular rhythm in AFib helps distinguish it from VTach.
To further differentiate these conditions, consider the patient's hemodynamic stability. VTach is often associated with hemodynamic compromise due to its ventricular origin, whereas SVT with aberrancy and PVCs are usually well-tolerated. AFib may or may not cause hemodynamic instability, depending on the ventricular rate. ECG analysis, including the presence of AV dissociation (seen in VTach but not in SVT or AFib), can also aid in diagnosis. AV dissociation appears as P waves occurring independently of the QRS complexes, a hallmark of VTach.
In summary, distinguishing VTach from SVT with aberrancy, PVCs, or AFib requires careful attention to rhythm regularity, QRS width, hemodynamic status, and ECG findings. VTach sounds like a rapid, regular, wide-complex rhythm, while SVT with aberrancy mimics this but has a supraventricular origin. PVCs produce occasional wide beats with compensatory pauses, and AFib is irregularly irregular with variably conducted QRS complexes. Mastery of these auditory and ECG patterns is essential for accurate diagnosis and appropriate management.
Pairing Sound Mates Earbuds: Quick and Easy Steps
You may want to see also
Explore related products



![]()
Treatment Options: Immediate defibrillation, antiarrhythmics, or cardioversion to restore normal rhythm
When addressing ventricular tachycardia (V-tach), a life-threatening arrhythmia characterized by rapid, irregular heartbeats originating in the ventricles, immediate and effective treatment is crucial. The primary goal is to restore a normal heart rhythm promptly to prevent hemodynamic collapse or ventricular fibrillation. Immediate defibrillation is the first-line treatment for unstable V-tach, where the patient is hemodynamically compromised, showing signs like hypotension, altered mental status, or chest pain. Defibrillation delivers a high-energy electric shock to the heart, halting the chaotic electrical activity and allowing the sinus node to re-establish a normal rhythm. This intervention is time-sensitive and must be performed without delay to improve survival rates.
In cases where the patient is stable—meaning they are conscious, have a palpable pulse, and are hemodynamically stable—antiarrhythmic medications may be used instead of immediate defibrillation. Amiodarone and lidocaine are commonly administered intravenously to suppress the abnormal electrical signals in the ventricles. These medications work by prolonging the refractory period of cardiac cells, thereby interrupting the re-entrant circuits that sustain V-tach. However, antiarrhythmics must be used cautiously, as they can sometimes worsen the arrhythmia or cause significant side effects, particularly in patients with impaired cardiac function.
Cardioversion is another treatment option, particularly for stable V-tach or when defibrillation is not immediately available. Cardioversion involves delivering a synchronized electric shock to the heart during a specific phase of the cardiac cycle (the R wave) to avoid inducing ventricular fibrillation. This method is less aggressive than defibrillation and is often used in controlled settings, such as in a hospital or emergency department. It is effective in terminating V-tach and restoring a normal sinus rhythm, especially when combined with antiarrhythmic therapy.
The choice of treatment—whether immediate defibrillation, antiarrhythmics, or cardioversion—depends on the patient’s clinical stability and the resources available. Unstable patients require immediate defibrillation to prevent cardiac arrest, while stable patients may benefit from pharmacological or synchronized electrical interventions. Regardless of the approach, continuous monitoring and rapid decision-making are essential to manage V-tach effectively. Additionally, identifying and addressing underlying causes, such as ischemia, electrolyte imbalances, or structural heart disease, is critical to prevent recurrence and ensure long-term management.
In summary, treating V-tach requires a swift and tailored approach. Immediate defibrillation is the cornerstone for unstable patients, while antiarrhythmics and cardioversion are viable options for stable individuals. Each treatment modality has its indications and risks, emphasizing the need for clinical judgment and expertise. Understanding the urgency and nuances of these interventions is vital for healthcare providers to manage this potentially fatal arrhythmia effectively.
Do Cinemagraphs Include Sound? Exploring the Silent Motion Trend
You may want to see also
Frequently asked questions
V-tach typically sounds like a rapid, regular rhythm without the normal P waves seen in a healthy heartbeat. The QRS complexes are wide and often appear at a rate of 100-250 beats per minute.
Unlike a normal heartbeat, which has a steady, rhythmic pattern, V-tach sounds faster and more chaotic, with wide QRS complexes and no visible P waves, indicating the heart’s electrical activity is originating in the ventricles.
While a stethoscope can detect a rapid heartbeat, it cannot provide the detailed rhythm information needed to diagnose V-tach. An ECG or heart monitor is required to accurately identify the wide QRS complexes and absence of P waves.
Many heart monitors and defibrillators are programmed to emit a distinct alarm or alert when V-tach is detected, as it is a life-threatening arrhythmia that requires immediate intervention.
V-tach sounds more organized and regular compared to AFib, which is typically irregular and chaotic. V-tach also has wide QRS complexes, whereas AFib shows narrow complexes with absent P waves.