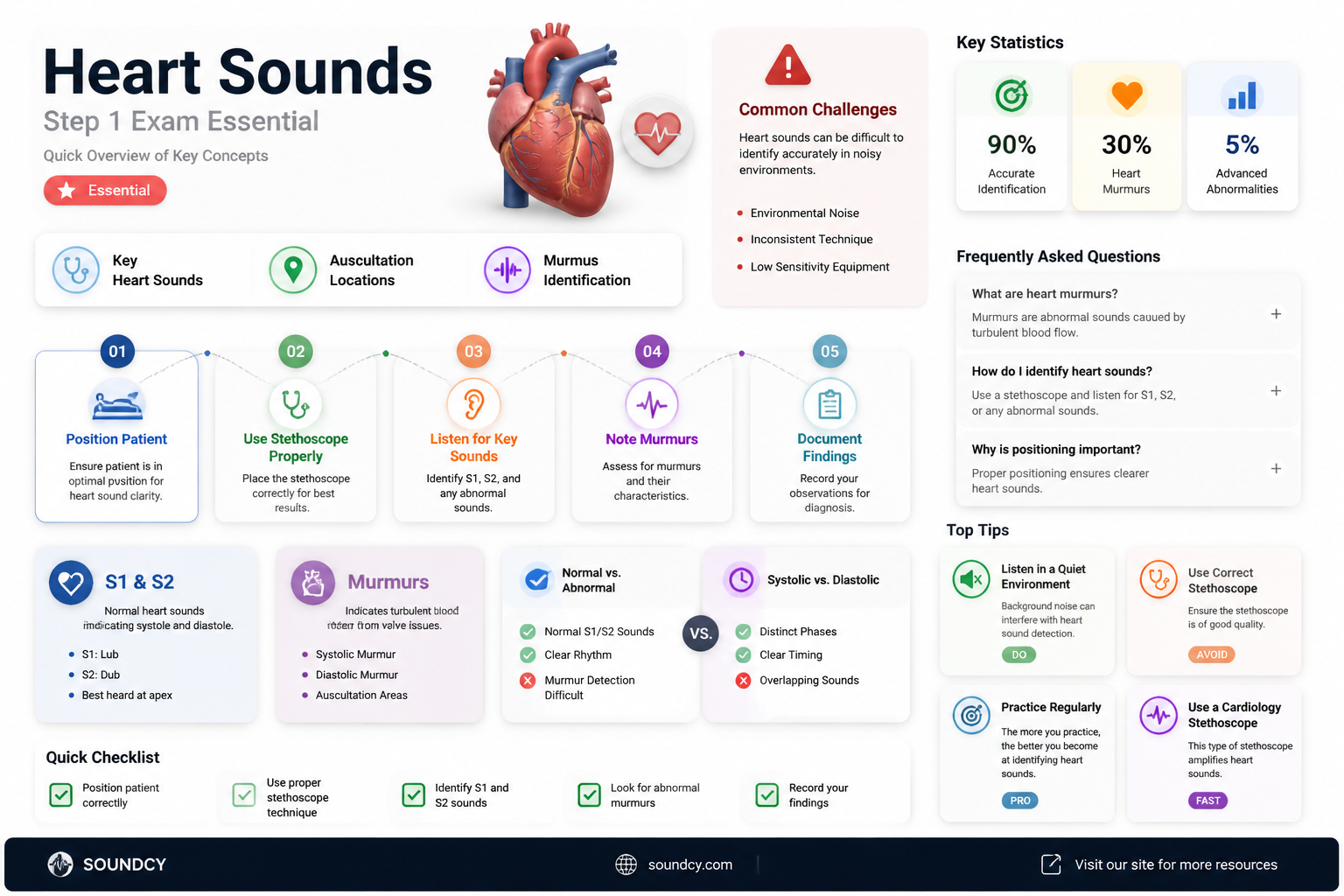
USMLE Step 1 is the first national board exam that all United States medical students must take before graduating from medical school. The exam includes heart sounds and murmurs, which can be challenging to identify and differentiate. Students often struggle with determining the location and timing of murmurs, such as mid, late, or pan-systolic. Knowing the heart sounds can give students an advantage during the exam. Various resources, such as Amboss and UWorld, offer practice with heart sounds, but the quality of the audio can vary. Some students recommend focusing on the question stem and theory, incidence, location, associations, and age related to the murmur, as the audio quality may not always be reliable.
| Characteristics | Values |
|---|---|
| Exam | USMLE Step 1 |
| Exam type | First national board exam |
| Examinee | All United States medical students |
| Exam time | Before graduating medical school |
| Heart sounds | Lub-dubs, systolic, diastolic, S3, S4, aortic regurg murmur, mitral regurg, aortic stenosis, mitral stenosis, etc. |
Explore related products






What You'll Learn
![]()
Differentiating systolic and diastolic murmurs
Murmurs are additional sounds generated by turbulent blood flow in the heart and blood vessels. Murmurs may be systolic, diastolic or continuous. Systolic murmurs are the most common type of murmur in children and are graded on a scale of 6. Diastolic murmurs, on the other hand, are graded on a scale of 4. Diastolic murmurs always indicate the presence of a valvular abnormality and are thus always pathological findings.
Systolic murmurs occur when blood is ejected through a narrowed orifice, such as in the case of stenosis of the aortic or pulmonic valves. They are typically classified into systolic ejection murmurs (SEM, crescendo-decrescendo) and decrescendo systolic murmurs. SEMs result from turbulent blood flow due to obstruction across the semilunar valves, outflow tracts, or arteries. The murmur is heard shortly after S1 (pulse), with its intensity increasing as more blood flows across the obstruction and then decreasing. Decrescendo systolic murmurs, a subtype of holosystolic murmurs, may be heard in patients with small VSDs. In the latter part of systole, the small VSD may close, causing the murmur to no longer be audible.
Diastolic murmurs occur when blood flows backward through a diseased valve when ventricular pressures drop during relaxation. This is seen in regurgitation of the aortic or pulmonic valves. Diastolic murmurs can be further classified into early, mid, and late diastolic murmurs. Early diastolic murmurs, such as aortic and pulmonary regurgitation, immediately follow S2. Mid-diastolic murmurs, or rumbles, are caused by increased flow through the mitral or tricuspid valves. Late diastolic murmurs, such as rheumatic mitral stenosis, are due to pathological narrowing of the AV valves.
Sound in Water: Faster Travel?
You may want to see also
Explore related products


$31.99 $34.99




![]()
Identifying aortic regurgitation
Aortic regurgitation, also known as aortic insufficiency, is a common form of heart valve disease. It occurs when the aortic valve, which controls blood flow between the aorta and the heart's main pumping chamber, does not close tightly. This results in blood leaking backward with each heartbeat, causing the heart to work harder over time to supply enough blood to the body.
The condition ranges from mild to severe and can be acute or chronic. Chronic, mild aortic regurgitation may not exhibit any symptoms for an extended period. However, as the condition progresses, symptoms such as chest pain, shortness of breath, palpitations, and chest pain or difficulty breathing may develop.
To diagnose aortic regurgitation, a physical examination is crucial. During the exam, healthcare providers inspect or palpate the precordium to check the location of the Point of Maximal Impulse (PMI). Normally, the PMI is at the 5th intercostal space on the left midclavicular line. A chest X-ray may also reveal swelling of the left lower heart chamber. Additionally, lab tests can help rule out other causes of symptoms, although they cannot directly diagnose aortic regurgitation.
Once a diagnosis of aortic regurgitation is established, further evaluation is necessary to identify any signs of heart failure, which can be either systolic or diastolic. One indicator of systolic heart failure is an S3 gallop, which is associated with heart enlargement in chronic aortic regurgitation. Peripheral cyanosis and cold, clammy extremities are also signs of systolic heart failure, resulting from poor peripheral blood flow due to reduced cardiac output. Calculating the pulse pressure (systolic BP – diastolic BP) is essential, as a high pulse pressure is typically observed in aortic regurgitation, while a normal or decreased pulse pressure may indicate incipient systolic heart failure.
The treatment for aortic regurgitation focuses on correcting the faulty aortic valve. Surgery may be performed to repair or replace the valve, and there is growing interest in minimally invasive procedures where a replacement valve is implanted via catheter. For those with aortic regurgitation-induced angina or congestive heart failure, prompt treatment is crucial for a favourable outcome.
Long Island Sound: A Northeast Gem
You may want to see also
Explore related products






![]()
Recognising mitral valve prolapse
Mitral valve prolapse is a common heart issue, affecting 2-3% of the general population. It is characterised by floppy valve leaflets that don't close tightly, allowing blood to leak backward from the left ventricle into the left atrium. This leakage is called regurgitation and can sometimes cause a heart murmur. MVP is often harmless, and many people with the condition have no symptoms and don't even know they have it. However, some people with MVP experience chest pain, shortness of breath, and heart palpitations.
MVP is usually identified during cardiac auscultation, and an echocardiogram (echo) is used to confirm the diagnosis. An echo uses ultrasound to evaluate the characteristics of the valve cusps and the amount of blood leaking through the valve. The test results, along with the patient's symptoms, will guide healthcare professionals in determining if further testing or treatment is needed.
To recognise mitral valve prolapse, it is essential to understand its symptoms, risk factors, and diagnostic procedures. Here are some key points to recognise and identify MVP:
- Symptoms: While most people with MVP are asymptomatic, some may experience chest pain, shortness of breath during exertion, and heart palpitations (feeling of rapid or irregular heartbeat).
- Risk factors: MVP can be genetic and is linked to several genes, including FLNA, DCHS1, DZIP1, and PLD1. It is also associated with connective tissue disorders such as Marfan syndrome, Ehlers-Danlos syndrome, and Loeys-Dietz syndrome. Additionally, rheumatic heart disease, scoliosis, and Graves' disease may increase the risk of MVP.
- Diagnosis: Cardiac auscultation, or listening to the heart sounds with a stethoscope, is typically the first step in identifying MVP. A murmur or an extra sound during systole or diastole may indicate MVP. Further diagnosis is confirmed through an echocardiogram, which uses ultrasound to visualise the valve cusps and assess the amount of regurgitation.
In summary, recognising mitral valve prolapse involves understanding its symptoms, risk factors, and diagnostic procedures. While MVP is often benign, it is crucial to identify and manage it appropriately to prevent potential complications. Early detection through cardiac auscultation and echocardiograms plays a vital role in ensuring timely treatment and maintaining cardiovascular health.
Korotkoff Sounds: The Five Phases of Blood Pressure Measurement
You may want to see also
Explore related products






![]()
Understanding the cardiac exam
The cardiac exam is typically structured around four pillars: history taking, inspection, palpation, and auscultation. History taking involves obtaining a thorough understanding of the patient's cardiac symptoms, including their medical history and any relevant family history. This information helps to build a comprehensive picture of the patient's cardiac health.
Inspection involves a careful examination of the patient's general appearance, skin, nails, mouth, neck, and extremities. For instance, inspecting the skin temperature can provide clues about cardiac function, with cool skin suggesting poor perfusion due to reduced cardiac output. Additionally, the presence of certain skin conditions, such as xanthomata or acanthosis nigricans, can be indicative of hypercholesterolemia or insulin resistance, respectively, both of which have correlations with heart disease.
Palpation is another critical aspect of the cardiac exam. This includes assessing the patient's peripheral pulses and evaluating distension of the right internal jugular vein (IJ). The IJ is in straight-line communication with the right atrium, and its distension can indicate elevated central venous pressure (CVP), providing valuable insights into intravascular volume status and cardiac function.
Auscultation is the use of a stethoscope to listen to the sounds produced by the heart and blood flow in the arteries and veins. It is crucial for differentiating cardiac murmurs from arterial bruits or venous hums. Murmurs are usually louder over the upper precordium and diminish toward the neck, while bruits are higher-pitched and heard only over the arteries. Auscultation also plays a role in blood pressure measurement, with the first sound heard as systolic pressure and the disappearance of sound indicating diastolic pressure.
In summary, understanding the cardiac exam requires a strong foundation in cardiac anatomy and the four pillars of history taking, inspection, palpation, and auscultation. By skillfully applying these principles, healthcare professionals can make accurate diagnoses and provide effective treatment for patients with cardiac conditions.
Aston Martin V8 Vantage: Music to Your Ears?
You may want to see also
Explore related products






![]()
Incidence, location, associations, and age of murmurs
Heart murmurs are sounds made by turbulent blood flow through the heart, often described as "whooshing" or "swishing". They can be heard with a stethoscope and can be present at birth (congenital) or develop later in life (acquired). Heart murmurs are common in newborns and children, with up to 80% of children experiencing a murmur during their early years. Some murmurs may resolve with time, while others persist into adulthood. The incidence of murmurs in infants ranges from 0.6% to 8.6%, with most being benign and transient. However, a significant proportion, around 37%, of these murmurs are associated with congenital heart disease, requiring early intervention.
The location of a murmur can be determined by using a stethoscope to listen to valve sounds and identify if it is systolic or diastolic. For example, an aortic regurgitation murmur may be indicated by bounding neck veins. In addition, the quality and timing of distal pulses can provide important information, with benign murmurs typically presenting with equal and normal pulses.
Associations of murmurs include congenital heart defects, such as holes in the heart or cardiac shunts, which can cause irregular blood flow. In older children and adolescents, a decrease in activity level, worsening exercise tolerance, and symptoms such as shortness of breath or chest pain may indicate underlying cardiac pathology. Advanced maternal age and conditions such as maternal infections and diabetes mellitus are associated with an increased risk of heart defects in newborns.
Age-related changes in murmurs include the potential resolution of innocent murmurs as individuals transition into adulthood. While most murmurs in older children are benign, it is important to monitor for any concerning symptoms or changes in activity levels, as these may indicate underlying cardiac issues.
Setting Up Elgato Sound Capture: A Step-by-Step Guide
You may want to see also
Frequently asked questions
Heart sounds refer to the sounds produced by the heart when blood flows through it or when the heart valves close.
Heart murmurs are whooshing or swishing sounds made by turbulent blood flow in or near the heart.
To identify a heart murmur, you should listen for any unusual sounds, such as lub-dubs, and determine the location, timing (systolic or diastolic), and characteristics of the murmur. Knowing the common types of murmurs, such as AS, PDA, S3, and S4, can also help in identification.
Yes, heart sounds and murmurs are included in the USMLE Step 1 exam, which is the first national board exam for medical students in the United States.