Appendicitis is a common cause of acute abdominal pain in adults and children, with a lifetime risk of 8.6% in males and 6.7% in females. It is challenging to diagnose due to its variable clinical presentation, and the rate of unnecessary appendectomies is approximately 15%. The diagnosis of acute appendicitis involves critical thinking, inductive and deductive reasoning, and a comprehensive evaluation of symptoms. The presence or absence of bowel sounds is an important indicator in diagnosing appendicitis, with decreased or absent bowel sounds being more common in children with appendicitis. In this context, bowel sounds refer to the noises produced by the movement of food, liquids, and gases through the intestines, which can be assessed by auscultation.
| Characteristics | Values |
|---|---|
| Most common cause of acute abdominal pain | Adults and children |
| Lifetime risk | 8.6% in males, 6.7% in females |
| Most common non-obstetric surgical emergency | Pregnancy |
| Symptoms in adults | Right lower quadrant pain, abdominal rigidity, periumbilical pain radiating to the right lower quadrant |
| Symptoms in children | Absent or decreased bowel sounds, a positive psoas sign, a positive obturator sign, a positive Rovsing sign |
| Bowel sounds | Hypoactive, absent in the presence of generalized peritonitis |
| Bowel obstruction | Can be identified with an abdominal X-ray |
| Appendicitis diagnosis | Plain film radiography, ultrasonography, preoperative computer tomography (CT) |
| Appendicitis treatment | Appendectomy, intravenous antibiotics, opioid painkillers, nonsteroidal anti-inflammatory drugs, acetaminophen, antibiotic therapy |
Explore related products





What You'll Learn
- Bowel sounds are absent or decreased in children with appendicitis
- Bowel sounds are diminished as appendiceal inflammation progresses
- Bowel obstruction may be indicated by absent bowel sounds
- Bowel sounds may be hypoactive in adults with appendicitis
- Normal or hyperactive bowel sounds cast doubt on appendicitis
![]()
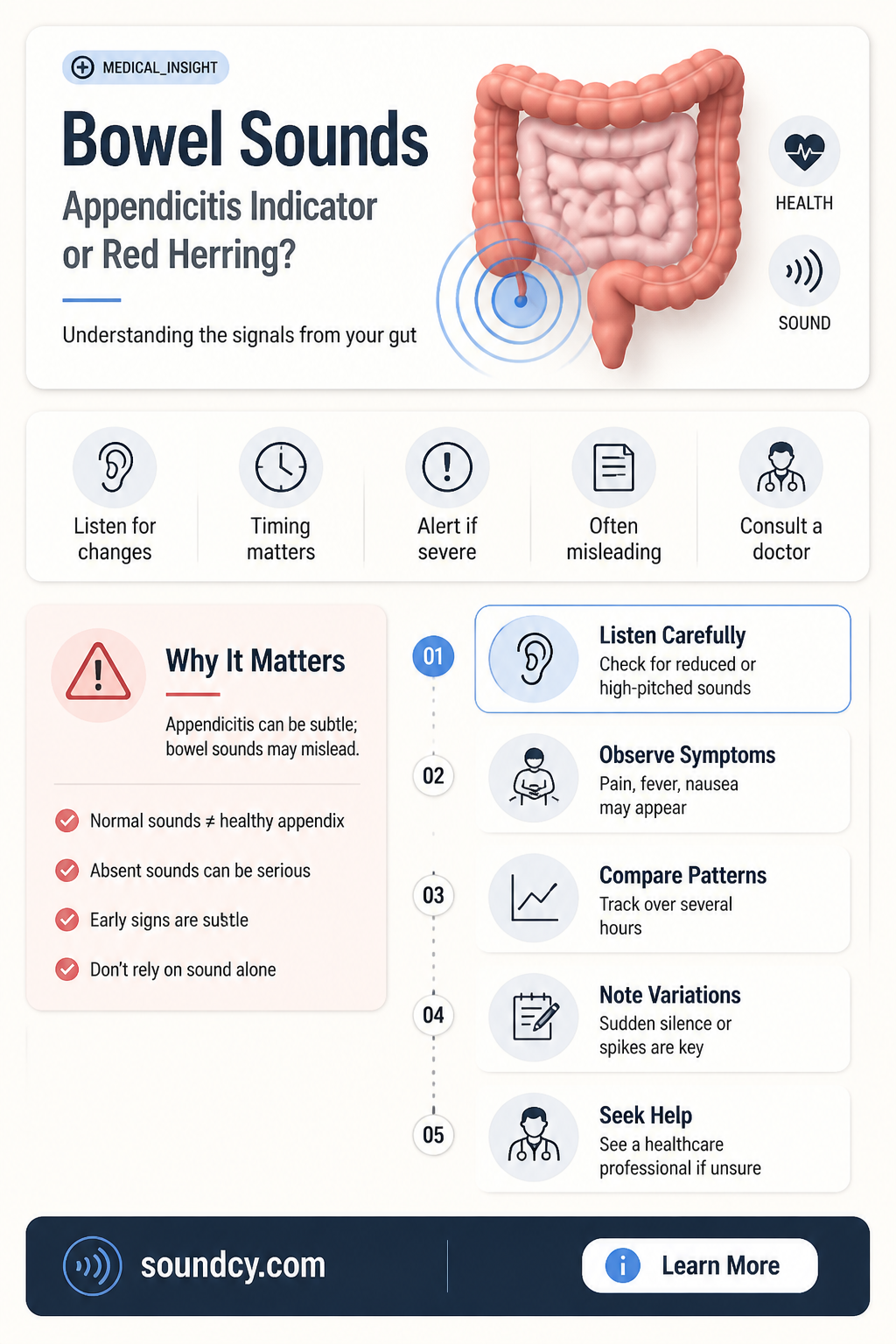
Bowel sounds are absent or decreased in children with appendicitis
Appendicitis is one of the most common causes of acute abdominal pain in both adults and children, with a lifetime risk of 8.6% in males and 6.7% in females. The diagnosis of acute appendicitis involves inductive and deductive reasoning, starting with a chief complaint, followed by a probing evaluation and expansion of the patient's history of symptoms.
In children, absent or decreased bowel sounds, a positive psoas sign, a positive obturator sign, and a positive Rovsing sign are the most reliable indicators of acute appendicitis. The Alvarado score, Pediatric Appendicitis Score, and Appendicitis Inflammatory Response score incorporate common clinical and laboratory findings to help make a timely diagnosis. Bowel sounds may be hypoactive or absent in the presence of generalized peritonitis, which is associated with appendicitis.
As appendiceal inflammation progresses, the protective mechanism of the bowel causes it to become less active, and bowel sounds are diminished until the abdomen becomes quiet. Normal or hyperactive bowel sounds cast doubt on a diagnosis of appendicitis. While evaluating bowel sounds, examiners should also listen to the lower lobes of the chest, as pneumonia in this area can cause inflammation that may be interpreted as abdominal pain.
The diagnosis of appendicitis can be challenging, especially in children, pregnant women, and the elderly, who may present with late or atypical features, leading to more severe or lethal complications. The variable location of the appendix also contributes to variations in clinical presentation. Imaging techniques such as ultrasonography and computer tomography (CT) can aid in diagnosis, and treatment options include appendectomy, antibiotic therapy, and pain management.
Adding Audio to PPT: A Simple Guide
You may want to see also
Explore related products






![]()
Bowel sounds are diminished as appendiceal inflammation progresses
Appendicitis is one of the most common causes of acute abdominal pain in adults and children, with a lifetime risk of 8.6% in males and 6.7% in females. The diagnosis of acute appendicitis involves inductive and deductive reasoning, starting with a chief complaint, followed by a probing evaluation and expansion of the patient's history of symptoms.
The most common presenting symptom of acute appendicitis is mid-abdominal or epigastric abdominal pain associated with anorexia, nausea, vomiting, fever, and leukocytosis. As the obstruction proceeds to edema and inflammation of the appendiceal wall, pain starts to localize in the dermatome overlying the infected appendix in the right lower quadrant. The single most important observation that places acute appendicitis at the top of a list of differential diagnoses is right lower quadrant tenderness.
In children, absent or decreased bowel sounds, a positive psoas sign, a positive obturator sign, and a positive Rovsing sign are most reliable for ruling in acute appendicitis. Bowel sounds may be hypoactive in association with appendicitis and absent in the presence of generalized peritonitis. As appendiceal inflammation progresses, the protective mechanism of the bowel causes it to become less active, and bowel sounds are diminished until the abdomen becomes quiet with frank peritonitis. Normal or hyperactive bowel sounds should cast doubt on a diagnosis of appendicitis.
The diagnosis of acute appendicitis can be challenging, especially in pregnant women, and atypical presentations are more common in children, geriatric, and pregnant patient populations, leading to delays in diagnosis. Clinical scoring systems and inflammatory markers are commonly used, but their limitations have led to the increased use of diagnostic imaging in suspected cases of appendicitis.
The Trumpet Sounds: What Happens Next?
You may want to see also
Explore related products






![]()
Bowel obstruction may be indicated by absent bowel sounds
In the context of appendicitis, absent or decreased bowel sounds are one of the most reliable signs for ruling in acute appendicitis in children. Appendicitis is a common cause of acute abdominal pain in both adults and children, and it can lead to serious complications such as perforation, abscesses, peritonitis, bowel obstruction, fertility issues, and sepsis. The diagnosis of acute appendicitis involves a combination of history, physical examination, and laboratory studies. Right lower quadrant pain, abdominal rigidity, and periumbilical pain radiating to the right lower quadrant are the most indicative signs in adults.
The presence or absence of bowel sounds is an important factor in the diagnosis of appendicitis. As appendiceal inflammation progresses, the bowel becomes less active, and bowel sounds diminish until the abdomen becomes quiet. Therefore, normal or hyperactive bowel sounds cast doubt on a diagnosis of appendicitis. However, it is important to note that absent bowel sounds can also be caused by other factors, such as abdominal surgery, certain medications, or general anesthesia.
In summary, absent bowel sounds can be an indicator of bowel obstruction and may be a sign of acute appendicitis in children. However, it is not the only factor considered in the diagnosis, and other symptoms and clinical findings are also evaluated to make a timely and accurate diagnosis.
Listen to Chest Sounds: A Stethoscope Guide
You may want to see also
Explore related products






![]()
Bowel sounds may be hypoactive in adults with appendicitis
Appendicitis is one of the most common causes of acute abdominal pain in adults and children, with a lifetime risk of 8.6% in males and 6.7% in females. It is notoriously difficult to diagnose, and the rate of unnecessary appendectomies is approximately 15%. The diagnosis of acute appendicitis is a good example of critical thinking in medicine, requiring both inductive and deductive reasoning.
The most common presenting symptom of acute appendicitis is mid-abdominal or epigastric abdominal pain associated with anorexia, nausea, vomiting, fever, and leukocytosis. As the infection extends into the peritoneal layer, pain becomes more localized to the region of the appendix. Bowel sounds may be hypoactive in adults with appendicitis, and absent in the presence of generalized peritonitis. The protective mechanism of the bowel causes it to become less active as appendiceal inflammation progresses, and bowel sounds are diminished until the abdomen becomes quiet.
Absent or decreased bowel sounds, a positive psoas sign, a positive obturator sign, and a positive Rovsing sign are most reliable for ruling in acute appendicitis in children. The Alvarado score, Pediatric Appendicitis Score, and Appendicitis Inflammatory Response score are useful in stratifying patients as low, moderate, or high risk and can aid in making a timely diagnosis. In adults, right lower quadrant pain, abdominal rigidity, and periumbilical pain radiating to the right lower quadrant are the best signs for ruling in acute appendicitis.
It is important to distinguish between appendicitis and other clinical conditions that may mimic it, such as caecal diverticulitis, infectious ileitis, ovarian cysts, and inflammatory bowel disease. Diagnostic imaging, such as ultrasonography and computer tomography (CT), can be useful in distinguishing between differential diagnoses.
The Sound of Silence: Performed by Simon & Garfunkel
You may want to see also
Explore related products






![]()
Normal or hyperactive bowel sounds cast doubt on appendicitis
Appendicitis is one of the most common causes of acute abdominal pain in adults and children, with a lifetime risk of 8.6% in males and 6.7% in females. It is the most common non-obstetric surgical emergency during pregnancy. The diagnosis of acute appendicitis is challenging and involves inductive and deductive reasoning. It starts with a chief complaint, followed by a probing evaluation and an expansion of the patient's history of symptoms.
The most common presenting symptom of acute appendicitis is mid-abdominal or epigastric abdominal pain associated with anorexia, nausea, vomiting, fever, and leukocytosis. As the infection progresses, pain becomes more localized to the region of the appendix. Physical examination in older children may reveal tenderness at McBurney's point, while younger children may only show localization to the right iliac fossa.
Right lower quadrant pain, abdominal rigidity, and periumbilical pain radiating to the right lower quadrant are the best signs for ruling in acute appendicitis in adults. In children, absent or decreased bowel sounds, a positive psoas sign, a positive obturator sign, and a positive Rovsing sign are most reliable for ruling in acute appendicitis. However, normal or hyperactive bowel sounds cast doubt on a diagnosis of appendicitis.
The presence of normal or hyperactive bowel sounds should prompt further evaluation, such as listening to the lower lobes of the chest, as pneumonia of the lower lobes can cause inflammation and be interpreted as abdominal pain. Additionally, the variable location of the appendix can lead to variations in clinical presentation, especially in pregnant women. Therefore, it is essential to consider other clinical conditions that may mimic appendicitis, such as caecal diverticulitis, infectious ileitis, ovarian cysts, and inflammatory bowel disease.
Ambient Sound: Sony XM4's Superpower
You may want to see also
Frequently asked questions
Bowel sounds may be hypoactive or absent in patients with appendicitis. This is due to the protective mechanism of the bowel, which causes it to become less active as appendiceal inflammation progresses. Normal or hyperactive bowel sounds cast doubt on a diagnosis of appendicitis.
Appendicitis is one of the most common causes of acute abdominal pain in adults and children. It affects all demographic groups and has a lifetime risk of 8.6% in males and 6.7% in females.
The most common symptom of acute appendicitis is mid-abdominal or epigastric abdominal pain associated with anorexia, nausea, vomiting, fever, and leukocytosis. Pain is typically constant and worsened by movement or palpation.
The diagnosis of acute appendicitis involves inductive and deductive reasoning. It starts with a chief complaint, followed by a probing evaluation and a history of symptoms. Physical examination findings specific for acute appendicitis include the psoas sign, the obturator sign, and the Rovsing sign. Imaging techniques such as ultrasonography and computer tomography (CT) can also aid in diagnosis.
The standard treatment for acute appendicitis is appendectomy, performed either via open laparotomy or laparoscopy. Antibiotic therapy is also an effective treatment option, especially in adults and children, and can be administered intravenously.