Auscultation is a technique used to listen to a patient's lung sounds and is a fundamental component of physical examination that can assist in diagnosing respiratory issues. It involves using a stethoscope to listen to the patient's respiratory system and interpreting the sounds heard. Lung sounds are caused by vibrations of the vocal cords during inhalation and exhalation, which are transmitted to the trachea and bronchi. These sounds can be used to monitor airflow through the trachea and bronchial tree. It is important to be able to distinguish between normal respiratory sounds and abnormal ones, such as crackles, wheezes, and pleural rub, in order to make a correct diagnosis. EMTs and paramedics are expected to auscultate a patient's blood pressure and listen to lung sounds as part of a respiratory illness physical exam.
| Characteristics | Values |
|---|---|
| Auscultation | Listening with a stethoscope |
| Purpose | To diagnose respiratory issues |
| Lung sounds | Vesicular, bronchial, bronchovesicular, crackles, rhonchi, wheezes, stridor and rubs |
| Lung sound characteristics | Volume, pitch, rustling quality, sound intensity |
| Lung sound location | Anterior chest, posterior chest, flanks |
| Lung sound procedure | Place diaphragm of stethoscope on patient's bare skin, apply gentle pressure, listen from high to low on patient's back |
Explore related products






What You'll Learn
![]()
Normal lung sounds
To listen for normal lung sounds, healthcare providers typically use a stethoscope on the patient's chest or back. It is important to start high on the patient's back and work down, ensuring the diaphragm of the stethoscope is placed firmly on the patient's bare skin. This technique helps distinguish lung sounds from bowel sounds, which can be heard below the posterior rib cage.
Additionally, providers may ask patients to take deep breaths or speak certain phrases to assess the clarity of the sounds. Normally, words whispered or spoken should be faintly heard through the stethoscope, indicating that the lungs are functioning properly.
By listening to a variety of normal lung sounds and understanding their characteristics, healthcare providers can more effectively identify abnormal lung sounds, such as crackles, wheezes, or pleural rub, which can indicate underlying respiratory issues.
Birdsong: Identifying Birds by Their Tunes
You may want to see also
Explore related products






![]()
Abnormal lung sounds
Listening to lung sounds is an essential part of the physical examination of a patient. Auscultation, which is listening with a stethoscope, is a non-invasive, inexpensive, and safe procedure that helps diagnose various respiratory disorders.
To listen to lung sounds, the diaphragm of the stethoscope is placed on the patient's bare back, above the posterior rib cage, and worked downwards. It is important to hold the diaphragm firmly in place, applying just enough pressure to prevent it from sliding as the patient breathes.
Normal lung sounds are described as a gentle whoosh of air during exhalation and inhalation. Vesicular sounds are the most common, usually heard over most of the chest wall. They are low to moderate in sound intensity with a low pitch of 200-600Hz and a rustling quality. Bronchial breath sounds are hollow and tubular, with a higher pitch than vesicular sounds.
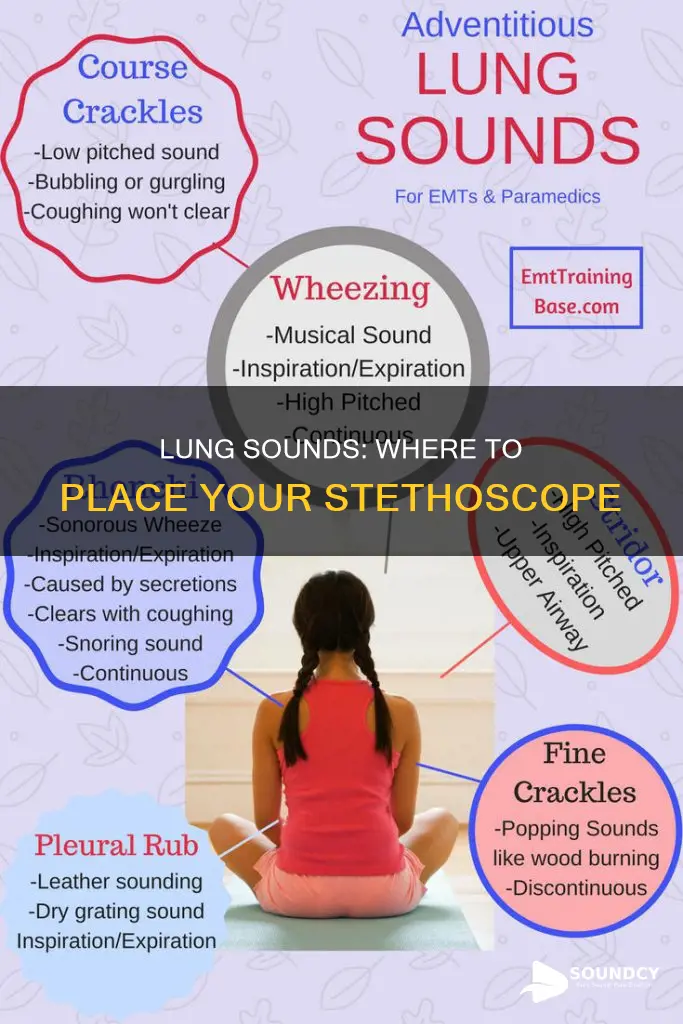
- Crackles: short, explosive, and non-musical sounds produced by patients with parenchymal lung diseases such as pneumonia, interstitial pulmonary fibrosis, and pulmonary edema.
- Wheezes: musical high-pitched sounds associated with airway diseases such as asthma and chronic obstructive pulmonary disease (COPD).
- Rhonchi: musical low-pitched sounds similar to snoring, indicating secretions in the airway, often cleared by coughing.
- Stridor: a high-pitched sound heard on inhalation and exhalation, indicating an obstruction in the airway.
- Pleural friction rub: a gritty sound caused by inflamed membranes lining the lungs rubbing against each other. This may occur during inhalation and exhalation and does not clear with coughing.
- Rales: abnormal sounds that may indicate pulmonary oedema or chronic bronchitis.
Identifying abnormal lung sounds requires familiarity with normal lung sounds and mindfulness during auscultation. Clinicians with more experience are better able to interpret respiratory sounds accurately. Automated classification systems using artificial intelligence have been developed to aid in the accurate identification and diagnosis of abnormal lung sounds.
Sound Properties: Understanding the Science of Hearing
You may want to see also
Explore related products

$59.99 $89.99



$13.6 $15.95


![]()
Lung sound characteristics
Normal breath sounds include bronchial, vesicular, or bronchovesicular sounds. Vesicular sounds are the most common auscultated sounds, usually heard over most of the chest wall. They are low to moderate in sound intensity with a low pitch of 200-600 Hz and a rustling quality. During expiration, the sound intensity can diminish. Bronchial breath sounds, on the other hand, are hollow and tubular, with a higher pitch than vesicular sounds.
Adventitious sounds are abnormal sounds that can indicate respiratory issues. These include crackles, rhonchi, wheezes, stridor, and rubs. Crackles are fine or coarse sounds that can be heard during inhalation or exhalation and are indicative of fluid or inflammation in the lungs. Wheezes are high-pitched sounds that occur when air tries to flow through a partially blocked airway. They can be inspiratory, expiratory, or both, and indicate narrowing of the airways. Stridor is a high-pitched sound that occurs when air flows through a severely blocked upper airway and is a medical emergency.
It is important to be familiar with both normal and abnormal lung sounds to be able to identify any abnormalities. Visualizing the anatomical location of the lungs is also crucial. The lungs are underneath and protected by the ribs, so starting high on the patient's back and working your way down is recommended to avoid hearing bowel sounds. The diaphragm of the stethoscope should be placed gently on the patient's bare skin, with enough pressure to keep it in place during breathing.
Sound Machines: White Noise, Better Sleep
You may want to see also
Explore related products






![]()
Lung sound locations
Lung auscultation is an important part of the physical examination and is helpful in diagnosing respiratory disorders. It involves using a stethoscope to listen to a patient's respiratory system and interpreting the lung sounds heard. It is a non-invasive, safe, and inexpensive procedure that is one of the oldest diagnostic techniques.
To listen to lung sounds, it is important to first prepare a quiet environment to clearly hear the patient's lung sounds. The patient should be sitting in a chair or upright on the side of the bed, with their chest and back exposed. Using gentle pressure, place the diaphragm (chest piece) of the stethoscope flat on the patient's chest. Listen to lung sounds on the anterior chest using the "stepladder" pattern, starting high and working your way down the patient's back.
The lungs are located underneath and protected by the ribs. If you are too low or below the posterior rib cage, you are more likely to hear bowel sounds instead of the whoosh of air moving in and out of the lungs. The diaphragm of the stethoscope, placed on the patient's bare skin, needs to be held firmly in place but not pressed deeply into the patient's tissue.
Normal lung sounds include bronchial, vesicular, or bronchovesicular sounds. These sounds have different characteristics depending on the anatomical auscultation location. Vesicular sounds are the most common auscultated sounds, usually heard over most of the chest wall. They are low to moderate in sound intensity with a low pitch and a rustling quality. During expiration, the sound intensity can diminish. Bronchial breath sounds, on the other hand, are hollow and tubular, with a higher pitch than vesicular sounds.
Abnormal lung sounds include crackles, wheezes, and pleural rub. It is important to be familiar with both normal and abnormal lung sounds to be able to identify any abnormalities during auscultation.
Troubleshooting Headset Static: Finding the Source
You may want to see also
Explore related products






![]()
Lung sound assessment
To perform a lung sound assessment, it is important to first ensure the patient is haemodynamically stable and their pain, if any, has been treated. The patient should then be positioned sitting in a chair or upright on the side of the bed, with their chest and back exposed while maintaining privacy and dignity. The diaphragm of the stethoscope is placed gently and firmly on the patient's bare skin, ensuring it does not slide with their breathing. It is important to start high on the patient's back, working your way down as you are more likely to hear bowel sounds if you start too low.
There are several types of lung sounds that can be heard during auscultation, including normal breath sounds such as bronchial, vesicular, or bronchovesicular sounds, and abnormal or adventitious sounds such as crackles, rhonchi, wheezes, stridor, and rubs. Vesicular sounds are the most common and are usually heard over most of the chest wall. They are low to moderate in intensity with a low pitch and a rustling quality. Bronchial breath sounds, on the other hand, are hollow and tubular, with a higher pitch than vesicular sounds.
Practicing lung sound auscultation and familiarising oneself with normal lung sounds is crucial for identifying abnormal sounds. This can be done through courses, quizzes, reference guides, and repetition drills. Additionally, it is important to consider the patient's medical history and current condition, age, and chest wall thickness when interpreting lung sounds. Other aspects of the patient's breathing, such as shallow breathing, pain, use of accessory muscles, and sputum production, should also be monitored during the assessment.
Sound Speed: How Fast Does it Travel?
You may want to see also
Frequently asked questions
Auscultation is a procedure that involves listening to a patient's lung sounds using a stethoscope. It is a fundamental, non-invasive component of physical examination that can assist in diagnosing respiratory issues.
Normal lung sounds include bronchial, vesicular, or bronchovesicular sounds. Vesicular sounds are the most common and are usually heard over most of the chest wall. They are low to moderate in sound intensity with a low pitch and a rustling quality.
Abnormal lung sounds, also known as adventitious sounds, include crackles, rhonchi, wheezes, stridor and rubs.
It is important to prepare a quiet environment to clearly hear the patient's lung sounds. The patient should be sitting in a chair or upright on the side of the bed, with their chest and back exposed. Using gentle pressure, place the diaphragm of the stethoscope flat on the patient's chest and listen to lung sounds on the anterior chest using the "stepladder" pattern. Start high on the patient's back and work your way down, making sure the diaphragm is held firmly in place.