Auscultation of lung sounds is a critical skill in medical practice, allowing healthcare professionals to assess respiratory health by listening to the sounds produced by airflow in the lungs. To effectively auscultate lung sounds, it is essential to know the specific anatomical locations where these sounds are best heard. The lungs are divided into lobes—three in the right lung (upper, middle, and lower) and two in the left lung (upper and lower)—and each area corresponds to distinct auscultation sites. Key locations include the anterior chest wall, posterior chest wall, and lateral chest wall, with specific points such as the apex of the lung, axillae, and bases. Proper positioning of the stethoscope over these areas ensures accurate detection of normal and abnormal lung sounds, aiding in the diagnosis of conditions like pneumonia, asthma, or chronic obstructive pulmonary disease (COPD). Understanding these auscultation sites is fundamental for comprehensive respiratory assessments.
| Characteristics | Values |
|---|---|
| Anterior Chest Wall | Auscultate over the upper, mid, and lower regions of the anterior chest. |
| Posterior Chest Wall | Auscultate over the upper, mid, and lower regions of the posterior chest. |
| Lateral Chest Wall | Auscultate over the axillary regions (lateral aspects of the chest). |
| Anterior Axillary Line | Focus on the mid-clavicular line for assessing lung sounds. |
| Posterior Axillary Line | Focus on the scapular region for posterior lung sounds. |
| Apical Region | Auscultate just above the clavicle for the lung apex. |
| Tracheal Area | Auscultate over the trachea to assess for breath sounds symmetry. |
| Lung Fields | Divide the chest into six lung zones (upper, middle, and lower on both sides). |
| Percussion Points | Use percussion to identify dullness or hyper-resonance before auscultation. |
| Patient Position | Auscultate in sitting or supine positions for optimal sound detection. |
| Key Landmarks | Use anatomical landmarks like the clavicle, scapula, and spine for guidance. |
| Depth of Auscultation | Listen at different depths (superficial to deep) for varied lung sounds. |
| Duration | Spend 10-15 seconds per location to adequately assess lung sounds. |
| Breathing Instructions | Ask the patient to breathe deeply through the mouth for clearer sounds. |
| Equipment | Use a stethoscope with proper diaphragm and bell placement. |
Explore related products




What You'll Learn
- Anterior Chest Wall: Auscultate upper, mid, lower zones bilaterally for breath sounds and abnormalities
- Posterior Chest Wall: Focus on scapular regions and lung bases for crackles or wheezes
- Lateral Chest Wall: Assess axillary areas for diminished or adventitious lung sounds
- Apical Lung Fields: Check above clavicles for unique sounds like bronchial breath sounds
- Tracheal Area: Listen over trachea for normal or abnormal breath sounds and symmetry
![]()
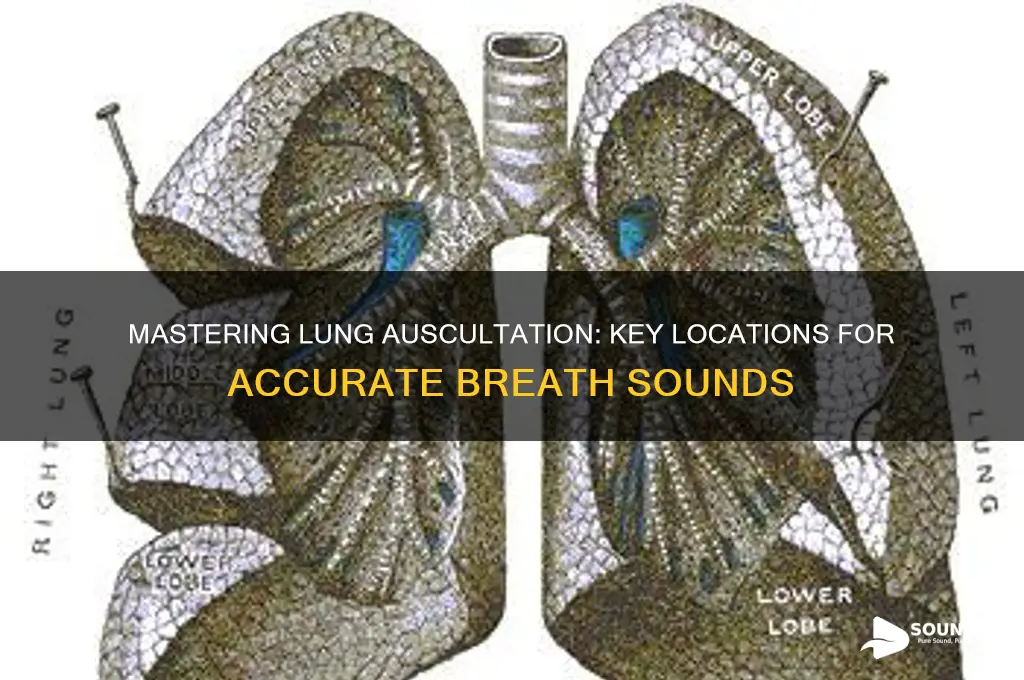
Anterior Chest Wall: Auscultate upper, mid, lower zones bilaterally for breath sounds and abnormalities
The anterior chest wall serves as a critical window into lung health, offering a direct pathway to assess breath sounds and detect abnormalities across distinct zones. Begin by dividing the chest into upper, mid, and lower zones bilaterally, ensuring a systematic approach. Position the patient in a seated or supine posture, exposing the chest fully to facilitate access. Use a stethoscope with firm but gentle pressure to minimize artifact and maximize sound clarity. Start at the upper zones, located just below the clavicles, and progress downward, comparing left and right sides for symmetry in sound quality and intensity.
Auscultation of the upper zones is particularly useful for detecting conditions like upper lobe pneumonia or chronic obstructive pulmonary disease (COPD), as these areas often reveal early signs of pathology. Listen for normal breath sounds, such as vesicular breathing, characterized by a soft, rustling quality during inspiration and a quieter phase during expiration. Abnormalities like wheezing, crackles, or diminished sounds warrant further investigation. For instance, bilateral wheezing in the upper zones may suggest asthma, while unilateral crackles could indicate localized infection or fluid accumulation.
The mid-zones, spanning the area between the nipples, are often the most straightforward to auscultate due to their central location. Here, breath sounds are typically louder and clearer, making it easier to identify deviations from normal. Pay attention to the transition between inspiration and expiration, as prolonged or turbulent phases can signal airway obstruction or consolidation. In pediatric patients, this area is especially valuable for assessing conditions like bronchiolitis, where wheezing and crackles are commonly heard.
The lower zones, situated below the nipple line, require careful attention due to their proximity to the diaphragm and potential for diminished sound transmission. Encourage the patient to take slow, deep breaths to enhance sound detection. Abnormal findings in this region, such as dullness or absent breath sounds, may indicate pleural effusion, pneumonia, or atelectasis. For elderly patients or those with obesity, adjusting the stethoscope angle and applying slightly firmer pressure can improve acoustic clarity.
In practice, a methodical approach to auscultating the anterior chest wall zones bilaterally is essential for accurate diagnosis. Begin with the upper zones, progress to the mid-zones, and conclude with the lower zones, ensuring each area is thoroughly examined. Document findings systematically, noting any asymmetry or abnormalities. For example, if crackles are heard in the left lower zone but not the right, this could suggest a localized issue like aspiration or early-stage heart failure. By mastering this technique, healthcare providers can effectively identify respiratory conditions early, guiding timely intervention and improving patient outcomes.
Thursday at 11 AM: Perfect Timing or Productivity Pitfall?
You may want to see also
![]()
Posterior Chest Wall: Focus on scapular regions and lung bases for crackles or wheezes
The posterior chest wall, particularly the scapular regions and lung bases, is a critical area for auscultation, as it often reveals subtle yet significant lung sounds that may indicate underlying respiratory conditions. These areas are prone to accumulation of fluid or mucus, making them prime locations for detecting crackles or wheezes. For instance, crackles in the lung bases can suggest congestive heart failure or pneumonia, while wheezes may point to asthma or chronic obstructive pulmonary disease (COPD). Understanding the anatomical significance of these regions ensures a more accurate diagnosis and targeted treatment plan.
To effectively auscultate the posterior chest wall, position the patient in a seated or upright posture, with arms resting comfortably on a surface to expose the scapular areas. Begin by placing the stethoscope’s diaphragm over the lung bases, listening for abnormal sounds as the patient takes slow, deep breaths. Gradually move upward toward the scapular regions, ensuring coverage of the entire posterior surface. Pay close attention to symmetry between the left and right sides, as asymmetry may indicate localized pathology. For pediatric patients, use a smaller stethoscope head and shorter auscultation times to minimize discomfort.
A comparative analysis of lung sounds in these regions can provide valuable insights. Crackles, often described as fine or coarse, are typically heard during inspiration and suggest fluid or inflammation in the alveoli. Wheezes, on the other hand, are high-pitched whistling sounds heard during expiration, indicative of airway narrowing. For example, fine crackles in the lung bases may resemble the sound of opening a Velcro strap, while wheezes can resemble the noise of air escaping a tight balloon. Recognizing these distinctions is essential for differentiating between conditions like interstitial lung disease and bronchial asthma.
Practical tips can enhance the auscultation process. Ensure the room is quiet to avoid masking faint sounds, and instruct the patient to breathe naturally to prevent artifactual noises. For elderly patients or those with obesity, gently pressing the stethoscope against the skin can improve sound transmission. Additionally, documenting the location and quality of sounds systematically (e.g., "fine crackles at left lung base") aids in longitudinal monitoring and communication with colleagues. Mastering these techniques transforms auscultation from a routine task into a powerful diagnostic tool.
In conclusion, focusing on the posterior chest wall, especially the scapular regions and lung bases, is indispensable for detecting crackles and wheezes that may signal respiratory pathology. By combining anatomical knowledge, precise technique, and comparative analysis, healthcare providers can uncover critical clues that guide diagnosis and treatment. Whether assessing a child with suspected pneumonia or an adult with COPD, this targeted approach ensures no abnormality goes unnoticed, ultimately improving patient outcomes.
Unveiling the Unique Vocalizations: What Does a Platypus Sound Like?
You may want to see also
![]()
Lateral Chest Wall: Assess axillary areas for diminished or adventitious lung sounds
The lateral chest wall, particularly the axillary areas, offers a unique window into lung health, often revealing subtle changes that might be missed in more central auscultation zones. These regions are especially valuable for detecting diminished breath sounds, which can indicate conditions like pneumothorax or pleural effusion, or adventitious sounds such as crackles or wheezes, suggestive of pneumonia or COPD exacerbation. Proper assessment here requires careful positioning—ask the patient to raise their arm slightly to expose the axilla fully, ensuring the stethoscope diaphragm makes firm contact with the skin. This technique is particularly useful in pediatric patients, where the chest wall is less expansive, and in elderly individuals with reduced lung compliance, where peripheral changes may manifest earlier.
A systematic approach to auscultating the axillary areas can significantly enhance diagnostic accuracy. Begin by comparing both sides simultaneously, noting asymmetry in sound intensity or quality. For instance, unilateral diminished sounds in the axilla may point to a localized obstruction or consolidation. Adventitious sounds in this area, such as crackles, often correlate with basal lung involvement, as seen in early-stage heart failure or aspiration pneumonia. Practitioners should also be mindful of patient body habitus—obese individuals may require additional pressure to overcome subcutaneous tissue interference, while underweight patients may exhibit exaggerated sound transmission.
One practical tip for optimizing axillary auscultation is to use the stethoscope's bell for low-pitched sounds, such as distant wheezes or pleural rubs, and the diaphragm for higher-pitched sounds like crackles or normal breath sounds. This dual approach ensures a comprehensive auditory profile. Additionally, encouraging the patient to take slow, deep breaths can amplify both normal and abnormal sounds, making them easier to discern. For children or uncooperative patients, auscultate during tidal breathing, focusing on the natural rhythm to avoid artifactual sounds induced by forced respiration.
While the axillary areas are diagnostically rich, they are often overlooked in routine lung examinations. Incorporating this region into standard practice can uncover early signs of pathology, particularly in patients with vague respiratory symptoms. For example, a middle-aged smoker presenting with mild dyspnea might exhibit wheezing in the axilla before central airways are affected, prompting timely intervention. Conversely, absence of expected sounds here can confirm the extent of conditions like a large pneumothorax, guiding immediate management decisions.
In conclusion, the lateral chest wall, especially the axillary areas, should not be a peripheral consideration in lung auscultation but a focal point for detecting nuanced changes. By integrating this region into the examination protocol, clinicians can enhance diagnostic precision, particularly in populations where central lung sounds may be misleading or insufficient. Mastery of this technique requires practice, but the payoff is significant—earlier detection of respiratory abnormalities and more targeted patient care.
How Gloss Affects the Sound of Your Ukulele
You may want to see also
![]()
Apical Lung Fields: Check above clavicles for unique sounds like bronchial breath sounds
The apical lung fields, located just above the clavicles, are a critical yet often overlooked area during auscultation. These regions are unique because they can reveal distinct breath sounds, such as bronchial breath sounds, which are typically heard over the trachea but may indicate pathology when detected here. To assess this area effectively, position the patient in a seated or semi-recumbent posture, ensuring the shoulders are relaxed. Place the diaphragm of your stethoscope firmly but gently on the skin, directly above the clavicle, and listen for any abnormalities. This simple step can provide early clues to conditions like pneumonia, consolidation, or even tumors, making it an essential part of a thorough lung examination.
Auscultating the apical lung fields requires precision and attention to detail. Unlike other lung regions, where breath sounds are typically vesicular, the apices may exhibit variations due to their proximity to the trachea and the unique anatomy of the upper lobes. Bronchial breath sounds in this area, characterized by their higher pitch and longer duration, can mimic those heard over the larynx but are abnormal here. To differentiate, note the sound’s quality and duration, and compare it with the opposite side. If bronchial breath sounds are present unilaterally, suspect conditions like consolidation or fluid accumulation. Bilateral findings may suggest more diffuse issues, such as pulmonary edema or chronic obstructive pulmonary disease (COPD).
For healthcare providers, mastering auscultation of the apical lung fields is both an art and a science. Begin by ensuring proper patient positioning, as slouching or tension can distort findings. Use a systematic approach, starting with the right apex and moving to the left, to maintain consistency. Be mindful of external factors like ambient noise or patient movement, which can interfere with accurate assessment. If bronchial breath sounds are detected, consider additional tests such as chest X-rays or CT scans to confirm the underlying cause. This targeted approach not only enhances diagnostic accuracy but also demonstrates clinical competence and attention to detail.
One practical tip for auscultating the apical lung fields is to ask the patient to take slow, deep breaths, as this can amplify breath sounds and make abnormalities more apparent. For pediatric patients or individuals with limited cooperation, focus on observing chest rise and fall while listening, as this can provide visual cues to complement auditory findings. Remember, the apices are particularly susceptible to early changes in lung pathology, so a meticulous examination here can be a game-changer in early detection and intervention. By integrating this practice into routine assessments, clinicians can improve patient outcomes and refine their diagnostic skills.
Unveiling the Silent World: Do Jellyfish Produce Any Sounds?
You may want to see also
![]()
Tracheal Area: Listen over trachea for normal or abnormal breath sounds and symmetry
The trachea, a vital conduit for air, serves as a critical auscultation site for assessing respiratory health. Positioned centrally in the neck, it offers a direct acoustic pathway to detect breath sounds that can reveal underlying conditions. To begin, place the diaphragm of your stethoscope firmly over the trachea, ensuring minimal ambient noise interference. Normal breath sounds here are typically silent or faint, as the trachea itself does not produce significant noise during respiration. However, abnormal sounds such as stridor (a high-pitched noise) or gurgling may indicate obstruction, inflammation, or foreign body presence. This initial assessment sets the stage for a more comprehensive lung examination, providing immediate clues about airway patency and potential pathology.
Auscultating the tracheal area requires precision and awareness of anatomical landmarks. Locate the trachea by palpating the midline of the neck, just above the sternal notch. For adults, the trachea is approximately 10–12 cm long, while in children, it is proportionally smaller, necessitating gentler pressure to avoid discomfort. Listen during both inspiration and expiration, noting any asymmetry or changes in sound intensity. Stridor, for instance, is more pronounced during inspiration and suggests upper airway narrowing, often seen in conditions like croup or epiglottitis. Conversely, expiratory stridor may indicate asthma or lower airway obstruction. Recognizing these nuances is crucial for timely intervention and accurate diagnosis.
Symmetry in tracheal breath sounds is another key parameter to evaluate. Normally, air flows evenly through the trachea, producing consistent sounds bilaterally. However, deviations from symmetry can signal significant issues. For example, a unilateral absence of breath sounds may indicate a pneumothorax or severe airway obstruction on the affected side. To ensure accuracy, compare findings with the patient’s medical history and other auscultation sites. In pediatric patients, asymmetry may be more challenging to detect due to smaller airways, so a systematic approach is essential. Always document observations clearly, as they provide a baseline for monitoring progression or response to treatment.
Practical tips can enhance the effectiveness of tracheal auscultation. Ensure the patient is in a comfortable, upright position to optimize airflow. For children or uncooperative patients, auscultate during quiet breathing or sleep to minimize movement artifacts. Use a stethoscope with a high-quality diaphragm for clearer sound transmission. If abnormal sounds are detected, repeat the assessment after repositioning the stethoscope slightly to confirm consistency. Finally, correlate findings with other diagnostic tools, such as chest X-rays or spirometry, for a holistic evaluation. Mastery of tracheal auscultation not only refines diagnostic skills but also fosters confidence in clinical decision-making.
Unveiling Autism's Unique Voice: Exploring the Sounds of Neurodiversity
You may want to see also
Frequently asked questions
The best locations on the anterior chest are the upper, mid, and lower regions of both the right and left chest, specifically over the lung fields.
The posterior chest is best auscultated between the 4th and 6th intercostal spaces, where lung sounds are most audible.
Avoid auscultating directly over bony structures like the clavicle or scapula, as they can muffle lung sounds. Focus on the intercostal spaces instead.
The lung bases are found in the lower posterior chest, approximately at the level of the 8th to 10th ribs, where the diaphragm meets the lungs.
Crackles are often heard at the lung bases, while wheezes are typically more prominent in the upper lung fields. Always auscultate both regions thoroughly.