Auscultation of breath sounds is a critical skill in diagnosing respiratory conditions, and knowing the precise locations to listen is essential for accurate assessment. The primary areas to auscultate include the anterior, posterior, and lateral chest walls, as well as the axillae. On the anterior chest, focus on the upper and lower lobes by placing the stethoscope between the second and fifth intercostal spaces, midclavicular lines, and along the sternum. Posteriorly, target the scapular and infrascapular regions, as well as the interscapular area, to assess the lower lobes and basal segments. Lateral auscultation helps evaluate the middle lobe and lingula. Proper positioning and systematic coverage of these areas ensure comprehensive evaluation of breath sounds, aiding in the identification of abnormalities such as wheezing, crackles, or diminished airflow.
Auscultation Sites for Breath Sounds
| Characteristics | Values |
|---|---|
| Anterior Chest Wall | Upper, middle, and lower lobes can be assessed. Place the stethoscope on the front of the chest, moving from the clavicle to the base of the lungs. |
| Posterior Chest Wall | Provides access to the lower lobes and posterior segments of the upper lobes. Position the patient sitting or standing, and auscultate along the back from the scapulae to the lower ribs. |
| Lateral Chest Wall | Allows assessment of the middle and lower lobes. Place the stethoscope on the sides of the chest, from the axilla to the lower ribs. |
| Apex of the Lung | Located in the supraclavicular fossa, above the clavicle. Auscultate for breath sounds in this area to assess the apex of the lung. |
| Tracheal Breath Sounds | Auscultate over the trachea, which is located in the midline of the neck. Normal breath sounds should be heard bilaterally. |
| Lobar Regions | Each lung is divided into lobes (upper, middle, and lower). Auscultate in specific areas to assess each lobe: upper lobe (above the level of the clavicle), middle lobe (between the clavicle and the nipple line), and lower lobe (below the nipple line). |
| Segmental Regions | Lungs are further divided into segments. Auscultate in specific segmental areas for detailed assessment, e.g., anterior, lateral, and posterior segments. |
| Comparison | Always compare both sides of the chest to identify asymmetry or abnormalities. |
| Patient Position | Auscultation can be performed with the patient in various positions: sitting, standing, or lying down (supine or lateral decubitus). |
| Stethoscope Technique | Use a stethoscope with a diaphragm for high-pitched sounds and a bell for low-pitched sounds. Apply light pressure for optimal sound transmission. |
Explore related products






What You'll Learn
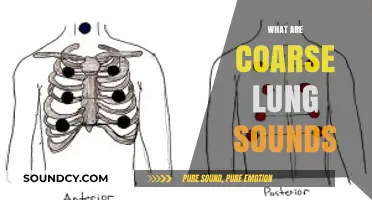
- Anterior Chest Wall: Auscultate upper, mid, lower zones bilaterally for normal or adventitious sounds
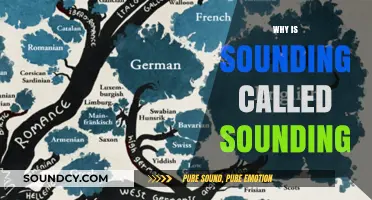
- Posterior Chest Wall: Focus on lung bases, apices, and scapular regions for crackles or wheezes
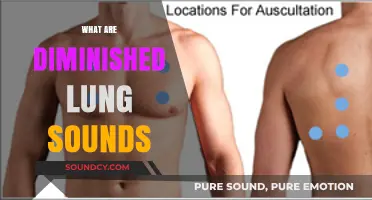
- Lateral Chest Wall: Assess axillary areas for diminished or absent breath sounds in pleural issues
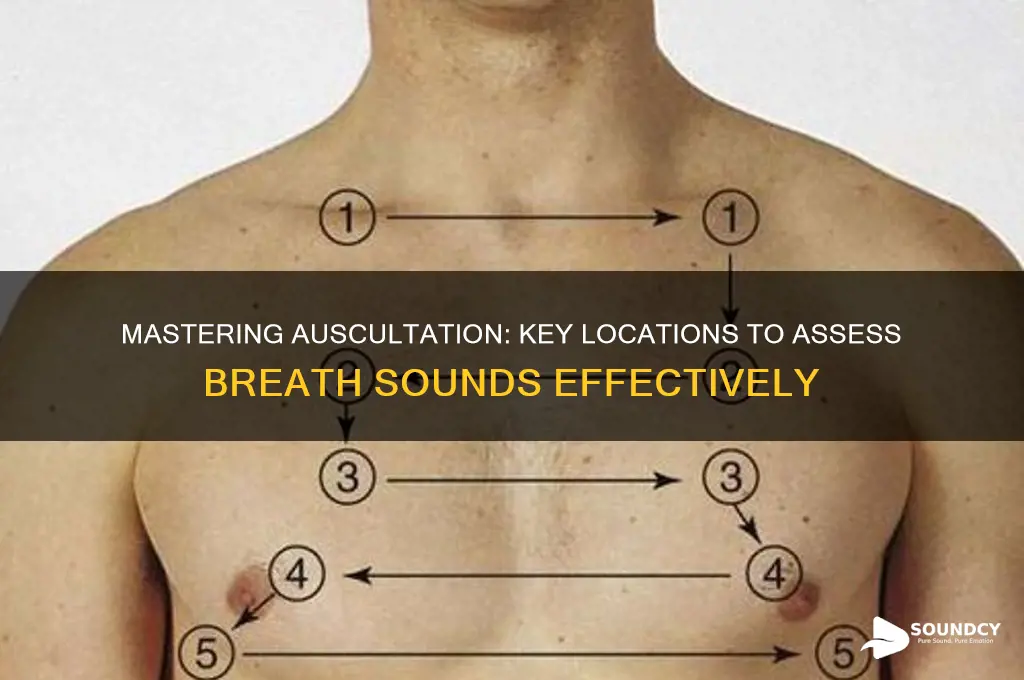
- Tracheal Region: Listen over the trachea for stridor or normal airflow patterns
- Comparison Technique: Compare bilateral lung fields to identify asymmetry or unilateral abnormalities
![]()
Anterior Chest Wall: Auscultate upper, mid, lower zones bilaterally for normal or adventitious sounds
When auscultating the anterior chest wall, it is essential to systematically examine the upper, mid, and lower zones bilaterally to identify normal or adventitious breath sounds. Begin by positioning the patient in a seated or supine position, ensuring they are comfortable and relaxed. Use a stethoscope with a diaphragm for high-pitched sounds and a bell for low-pitched sounds. Start with the upper zones, which correspond to the second and third rib spaces bilaterally. Place the stethoscope firmly on the skin, comparing both sides simultaneously to detect asymmetry or abnormalities. Normal breath sounds in this area should be clear and symmetrical, with inspiration and expiration being equal in duration and intensity.
Next, move to the mid-zones of the anterior chest wall, located between the fourth and sixth rib spaces. This area often provides a clearer representation of lung sounds due to less interference from chest wall structures. Auscultate bilaterally, listening for normal bronchial or bronchovesicular sounds, which are a blend of bronchi and alveoli sounds. Adventitious sounds such as wheezes, rhonchi, or crackles in this zone may indicate conditions like asthma, chronic obstructive pulmonary disease (COPD), or pneumonia. Ensure the stethoscope is moved systematically to cover the entire mid-zone, as localized abnormalities can be missed with inadequate coverage.
Proceed to the lower zones, situated between the seventh and ninth rib spaces, just above the costal margin. This area is particularly important for detecting basal lung pathologies. Normal vesicular breath sounds should be softer and longer during inspiration compared to expiration. Adventitious sounds like fine or coarse crackles may suggest fluid accumulation or infection, while diminished or absent breath sounds could indicate consolidation or pneumothorax. Bilateral comparison is crucial, as unilateral changes often signify localized issues. Maintain consistent pressure with the stethoscope to avoid artifactual sounds that could mimic pathology.
Throughout the auscultation of the anterior chest wall, pay attention to the quality, intensity, and duration of breath sounds. Normal sounds are typically symmetrical and consistent across zones, while adventitious sounds may vary in pitch, timing, and location. Document findings clearly, noting any asymmetry or abnormalities. Encourage the patient to breathe deeply and normally to ensure accurate assessment. If adventitious sounds are detected, further evaluation of posterior and lateral chest walls may be necessary to confirm the diagnosis and localize the pathology.
Finally, practice and familiarity with normal breath sounds are key to identifying abnormalities effectively. Repeat auscultation if necessary, especially in areas where sounds are faint or unclear. Remember that the anterior chest wall provides a foundational assessment, but a comprehensive lung examination should include other regions for a complete evaluation. Systematic and methodical auscultation of the upper, mid, and lower zones bilaterally ensures no critical findings are overlooked, enabling timely and accurate clinical decision-making.
Soundproofing Secrets: Best Ways to Insulate Your Space
You may want to see also
Explore related products






![]()
Posterior Chest Wall: Focus on lung bases, apices, and scapular regions for crackles or wheezes
When auscultating the posterior chest wall, it is crucial to focus on specific areas such as the lung bases, apices, and scapular regions to detect abnormal breath sounds like crackles or wheezes. Begin by positioning the patient in a seated or upright position, ensuring their arms are relaxed to expose the entire posterior chest wall. Use a stethoscope with the diaphragm for low-pitched sounds and the bell for high-pitched sounds. Start at the lung bases, which are located near the lower back, just above the diaphragm. These areas are prone to fluid accumulation, making them a common site for crackles, often heard in conditions like pneumonia or heart failure. Apply gentle pressure with the stethoscope to ensure optimal sound transmission and listen carefully for any adventitious sounds.
Next, move to the lung apices, situated at the uppermost part of the posterior chest wall, near the first and second ribs. This region is particularly important for detecting wheezes, which may indicate airway obstruction or conditions such as asthma or chronic obstructive pulmonary disease (COPD). Wheezes are high-pitched, whistling sounds that occur due to narrowed airways. Ensure the stethoscope is placed lightly on the skin to capture these sounds accurately. Compare findings between the left and right apices to identify asymmetry, which could suggest localized pathology.
The scapular regions, located between the shoulder blades, are another critical area to auscultate. These regions correspond to the middle and lower lung fields and are often associated with crackles in patients with interstitial lung disease or congestive heart failure. Position the stethoscope along the paraspinous muscles, moving systematically from top to bottom. Pay attention to the quality and timing of crackles—whether they are fine or coarse and if they occur during inspiration or expiration. This information is vital for differentiating between various respiratory conditions.
When auscultating these areas, maintain a methodical approach by dividing the posterior chest wall into sections and listening to each area for at least 5–10 seconds. Ensure the patient takes slow, deep breaths to maximize the detection of abnormal sounds. Document the location, intensity, and characteristics of any crackles or wheezes observed. For example, note whether crackles are localized to one lung base or widespread across the scapular regions. This detailed assessment aids in diagnosing the underlying cause of the abnormal breath sounds.
Finally, consider the patient’s clinical context while interpreting findings. For instance, bilateral basal crackles may suggest pulmonary edema, while unilateral crackles could indicate lobar pneumonia. Wheezes heard predominantly in the apices might point to upper airway obstruction. By focusing on the lung bases, apices, and scapular regions of the posterior chest wall, healthcare providers can effectively identify and localize respiratory abnormalities, guiding appropriate management and treatment. Always repeat auscultation if initial findings are unclear to ensure accuracy.
The Button: Press or Not to Press?
You may want to see also
Explore related products






![]()
Lateral Chest Wall: Assess axillary areas for diminished or absent breath sounds in pleural issues
When assessing the lateral chest wall, particularly the axillary areas, for breath sounds, it is crucial to focus on detecting diminished or absent sounds, which can indicate pleural issues. The axillary region, located in the armpit area, is an important site for auscultation because it allows the healthcare provider to evaluate the peripheral lung fields. To begin, ensure the patient is in a comfortable position, ideally sitting upright or semi-reclined, with their arms resting by their sides or slightly abducted to expose the axillary area. Use a stethoscope with the diaphragm for adults or the bell for children, placing it firmly but gently on the skin to minimize artifact noise.
Start by identifying the anatomical landmarks of the axillary region, which extends from the anterior to the posterior axillary folds. Divide this area into upper, middle, and lower zones to systematically assess breath sounds. Begin at the upper axillary region, moving downward, and compare findings between the left and right sides. Normal breath sounds in this area should be clear and symmetrical, with inspiration and expiration audible. However, in cases of pleural effusion, pneumothorax, or other pleural conditions, breath sounds may be significantly reduced or absent due to air or fluid accumulation in the pleural space.
Diminished breath sounds in the axillary area often suggest a pleural effusion, where fluid collects between the lung and chest wall, dampening sound transmission. In contrast, absent breath sounds are more indicative of a pneumothorax, where air in the pleural space collapses the lung and prevents air movement. To differentiate, note the quality and intensity of the sounds. For example, a pleural effusion may still allow faint sounds to be heard, whereas a pneumothorax typically results in complete silence. Additionally, assess for tactile fremitus, which is often decreased or absent in these conditions due to the disrupted vibration of the chest wall.
When auscultating, ensure the stethoscope is moved in a methodical pattern, covering the entire axillary region. Pay attention to any asymmetry between the left and right sides, as this is a key indicator of pathology. If diminished or absent breath sounds are detected, further investigation with imaging, such as a chest X-ray or ultrasound, is warranted to confirm the diagnosis. It is also important to correlate auscultation findings with the patient’s symptoms, such as shortness of breath, chest pain, or cough, which can provide additional context for the clinical picture.
Finally, document the findings clearly, noting the specific location, intensity, and quality of breath sounds in the axillary areas. Include observations about symmetry, tactile fremitus, and any associated symptoms. This detailed documentation aids in monitoring changes over time and guiding subsequent interventions. Assessing the lateral chest wall, particularly the axillary areas, is a critical skill in identifying pleural issues early, ensuring timely and appropriate management for the patient. Mastery of this technique enhances the accuracy of respiratory assessments and contributes to better patient outcomes.
Mastering Custom Key Sounds: A Step-by-Step Guide to Assigning Audio
You may want to see also
Explore related products






![]()
Tracheal Region: Listen over the trachea for stridor or normal airflow patterns
When auscultating breath sounds, the tracheal region is a critical area to assess, as it provides valuable information about airflow patterns and potential abnormalities. To begin, position the patient comfortably, preferably in an upright or semi-recumbent position, to ensure optimal sound transmission. Place the diaphragm of your stethoscope directly over the trachea, which is located in the anterior neck, just below the larynx and above the suprasternal notch. This area is easily accessible and allows for clear detection of breath sounds. The primary goal here is to listen for either normal airflow patterns or the presence of stridor, a high-pitched, musical sound indicative of upper airway obstruction.
Normal breath sounds in the tracheal region are characterized by a quiet, smooth airflow without any added noises. During inspiration and expiration, the sounds should be symmetrical and consistent, reflecting unobstructed air movement through the trachea. It is essential to listen carefully for any deviations from this norm, as even subtle changes can signal underlying issues. For instance, a mild increase in airflow noise might suggest tracheal irritation or inflammation, while complete silence could indicate a severe obstruction or improper stethoscope placement.
Stridor is a key abnormality to identify when auscultating the tracheal region. It is typically heard during inspiration and is caused by turbulent airflow through a narrowed or partially obstructed upper airway. Stridor can result from various conditions, including laryngeal edema, foreign body aspiration, or tumors. The pitch and intensity of stridor can provide clues about the obstruction's location: higher-pitched sounds often indicate a more distal obstruction, while lower-pitched sounds suggest a proximal issue. Recognizing stridor promptly is crucial, as it may signify a life-threatening condition requiring immediate intervention.
To ensure accurate assessment, maintain a systematic approach during auscultation. Compare the sounds between inspiration and expiration, noting any asymmetries or inconsistencies. Additionally, observe the patient's respiratory effort and overall comfort, as labored breathing or distress can further support your findings. If stridor or other abnormalities are detected, consider the patient's medical history and risk factors to guide further diagnostic steps. For example, a history of smoking or recent upper respiratory infection might influence the differential diagnosis.
In summary, auscultating the tracheal region involves careful placement of the stethoscope over the trachea to evaluate airflow patterns. Normal breath sounds are quiet and smooth, while stridor indicates turbulent airflow due to upper airway obstruction. Recognizing these distinctions is vital for identifying potential respiratory issues early. By combining auscultation with patient observation and medical history, healthcare providers can make informed decisions and ensure appropriate management of tracheal and upper airway conditions.
How Stone Matrix Asphalt Reduces Noise Pollution
You may want to see also
Explore related products






![]()
Comparison Technique: Compare bilateral lung fields to identify asymmetry or unilateral abnormalities
When employing the Comparison Technique to auscultate breath sounds, the primary goal is to identify asymmetry or unilateral abnormalities by systematically comparing the bilateral lung fields. Begin by positioning the patient in a comfortable, upright posture, ensuring both sides of the chest are accessible. Use a stethoscope with a diaphragm for high-pitched sounds and a bell for low-pitched sounds, depending on the suspected pathology. Start auscultation at the same anatomical location on both sides of the chest to maintain consistency. For example, begin at the first intercostal space along the midclavicular line on the right side, then move to the corresponding location on the left side. This bilateral comparison allows for immediate detection of discrepancies in breath sounds, such as diminished or absent sounds on one side, which may indicate conditions like pneumothorax or consolidation.
Proceed by systematically moving down the lung fields, auscultating at predefined points such as the midclavicular, anterior axillary, and midaxillary lines. Ensure each location is assessed on both the right and left sides before moving to the next. Pay close attention to the intensity, pitch, and quality of breath sounds, noting any differences between the two sides. For instance, wheezing or crackles confined to one lung field could suggest localized inflammation, infection, or obstruction. The comparison technique is particularly useful for identifying unilateral conditions like pleural effusion, where breath sounds may be significantly reduced on the affected side compared to the clear, resonant sounds on the contralateral side.
Incorporate posterior and lateral lung fields into the comparison to ensure a comprehensive assessment. Have the patient lean forward or turn to the side to access these areas, maintaining the bilateral comparison approach. For example, auscultate the scapular regions on both sides, noting any asymmetry in breath sounds that might indicate posterior basal pneumonia or atelectasis. The lateral fields, especially the axillary regions, are critical for detecting early signs of fluid accumulation or airspace disease, as these areas are often the first to show changes due to their dependent position.
Document findings meticulously, noting the specific locations of any asymmetry or abnormalities. For example, record observations such as "diminished breath sounds over the right lower lobe compared to the left" or "bilateral wheezing more pronounced on the left." This detailed documentation aids in diagnosis and monitoring of progression or resolution of lung conditions. The comparison technique not only highlights unilateral issues but also provides a baseline for future assessments, ensuring any new developments are promptly identified.
Finally, integrate the comparison technique with other auscultation methods, such as assessing for adventitious sounds or evaluating vocal resonance, to enhance diagnostic accuracy. For instance, if unilateral diminished breath sounds are detected, further investigate by percussing the chest to differentiate between consolidation and pneumothorax. By consistently comparing bilateral lung fields, clinicians can effectively identify asymmetry or unilateral abnormalities, guiding appropriate diagnostic and therapeutic interventions. This technique is a cornerstone of respiratory assessment, ensuring no subtle or significant differences between lung fields are overlooked.
Exploring the Speed of Sound: How Fast Does It Travel?
You may want to see also
Frequently asked questions
The best locations on the anterior chest are the trachea (for normal breath sounds), the second intercostal space (for aortic valve sounds), and the fourth to fifth intercostal spaces near the midclavicular line (for lung fields).
Focus on the scapula regions (for lower lung fields), the sixth to eighth intercostal spaces near the midscapular line (for posterior lung fields), and the tenth to twelfth intercostal spaces near the spine (for basal lung fields).
Yes, in pediatric patients, auscultate the anterior chest at the second and fourth intercostal spaces, and the posterior chest at the scapula regions and along the midscapular and paravertebral lines, adjusting for smaller anatomy.