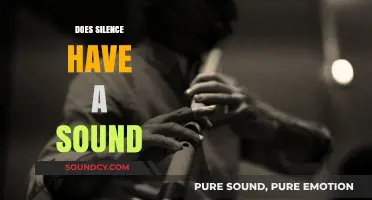
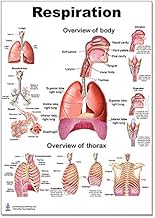
Vesicular sounds, also known as breath sounds, are primarily heard over the lung fields during auscultation and are characterized by their soft, blowing quality, resembling the rustling of leaves. These sounds are typically heard bilaterally and symmetrically across the chest, with their intensity and pitch varying depending on the location. They are most prominent over the anterior and posterior chest walls, particularly in the upper lung fields, and are generated by the movement of air through the larger airways, such as the bronchi and bronchioles. Understanding where vesicular sounds are heard is crucial for healthcare professionals, as alterations in their quality, intensity, or distribution can indicate underlying respiratory conditions, such as pneumonia, chronic obstructive pulmonary disease (COPD), or asthma.
| Characteristics | Values |
|---|---|
| Location | Primarily over the lung parenchyma, especially in the alveoli and small airways |
| Auscultation Area | Heard best over the anterior and posterior chest walls, with increased intensity in the upper lung fields |
| Sound Quality | Soft, low-pitched, rustling sounds resembling the rustling of leaves or taffeta |
| Duration | Lasts throughout the entire respiration cycle (both inspiration and expiration) |
| Intensity | Generally soft to moderately loud, depending on the depth of respiration |
| Timing | Continuous and even, without interruptions or gaps |
| Pathophysiology | Normal air movement in and out of the alveoli and small airways |
| Associated Conditions | Normal lung function; absent or decreased in conditions like pneumonia, atelectasis, or pleural effusion |
| Comparison | In contrast to bronchial breathing (louder, higher-pitched, and over larger airways) and absent breath sounds (e.g., in pneumothorax) |
| Clinical Significance | Indicates healthy lung tissue and normal ventilation; changes may suggest underlying pathology |
Explore related products





What You'll Learn
- Anterior Chest Wall: Vesicular sounds are heard over the anterior chest wall, especially in the upper lobes
- Posterior Chest Wall: These sounds are prominent over the posterior chest wall, particularly in the lower lobes
- Lateral Chest Wall: Vesicular sounds are audible along the lateral chest wall, extending from apex to base
- Apical Region: In the apical region, vesicular sounds are higher pitched and shorter in duration
- Basal Region: The basal region exhibits longer, softer vesicular sounds due to increased airflow resistance
![]()
Anterior Chest Wall: Vesicular sounds are heard over the anterior chest wall, especially in the upper lobes
Vesicular sounds are a fundamental component of respiratory auscultation, and their presence or absence can provide valuable insights into lung health. When examining the anterior chest wall, these sounds are particularly prominent, especially over the upper lobes of the lungs. The anterior chest wall corresponds to the front of the thorax, encompassing the area from the sternum to the axillary lines. This region overlies the upper lobes of both lungs, making it an ideal location to auscultate vesicular sounds in healthy individuals. These sounds are characterized by a soft, rustling quality that correlates with airflow during normal breathing.
The upper lobes of the lungs are well-ventilated and receive a significant portion of the inspired air, which explains why vesicular sounds are most pronounced in this area. During auscultation, the clinician should place the stethoscope over the anterior chest wall, focusing on the second and third intercostal spaces. Here, the sounds are typically continuous and of low intensity, reflecting the smooth movement of air through the alveoli. It is essential to listen carefully during both inspiration and expiration, as vesicular sounds are more prominent during inspiration due to the increased airflow.
Several factors contribute to the clarity and intensity of vesicular sounds over the anterior chest wall. The thinner subcutaneous tissue in this region allows for better sound transmission compared to other areas of the chest. Additionally, the upper lobes are less prone to obstruction or consolidation, ensuring that airflow remains laminar and produces the characteristic rustling sounds. Clinicians should be mindful of patient positioning during auscultation, as sitting or leaning forward slightly can enhance sound detection by optimizing lung expansion.
Abnormalities in vesicular sounds over the anterior chest wall can indicate underlying respiratory issues. For instance, diminished or absent sounds may suggest air trapping, consolidation, or pleural effusion. Conversely, exaggerated or coarse vesicular sounds could be indicative of conditions like chronic obstructive pulmonary disease (COPD) or bronchiectasis. Therefore, understanding the normal auscultatory findings over the anterior chest wall is crucial for identifying deviations that warrant further investigation.
In summary, the anterior chest wall is a key area for auscultating vesicular sounds, particularly over the upper lobes of the lungs. These sounds are soft, rustling, and continuous, reflecting normal airflow during breathing. Clinicians should focus on the second and third intercostal spaces, ensuring proper patient positioning to optimize sound detection. Recognizing the characteristics of vesicular sounds in this region is essential for identifying respiratory abnormalities and guiding appropriate clinical management.
Understanding Atrial Fibrillation: What Does AFib Sound Like?
You may want to see also
Explore related products




![]()
Posterior Chest Wall: These sounds are prominent over the posterior chest wall, particularly in the lower lobes
Vesicular sounds, a type of lung sound characterized by soft, low-pitched, and rustling noises, are most prominently heard over specific areas of the chest during auscultation. One key location where these sounds are particularly noticeable is the posterior chest wall, especially in the lower lobes. This area is crucial for clinicians to assess because it provides valuable insights into the health and function of the lungs. The posterior chest wall is an ideal site for detecting vesicular sounds due to the anatomical positioning of the lower lobes, which are more accessible and resonant in this region. When a healthcare provider listens to this area with a stethoscope, the sounds are typically clear and consistent, reflecting normal air movement through the alveoli.
The prominence of vesicular sounds over the posterior chest wall, particularly in the lower lobes, is attributed to the anatomical structure of the lungs. The lower lobes are larger and more vertically oriented compared to the upper lobes, allowing for greater air exchange and sound production during breathing. Additionally, the posterior chest wall provides a direct acoustic pathway for these sounds, as the stethoscope is placed on a relatively flat and thin surface, minimizing tissue interference. This makes the posterior chest wall an optimal location for auscultation, especially when evaluating patients in a seated or upright position, as gravity helps the lower lobes expand more fully.
Clinicians often focus on the posterior chest wall to differentiate vesicular sounds from other lung sounds, such as wheezes or crackles. Vesicular sounds in this area are typically symmetrical between the left and right sides, with a slight increase in intensity during inspiration. This symmetry and pattern are essential for establishing a baseline of normal lung function. Any deviation, such as diminished or asymmetrical sounds, may indicate underlying conditions like pneumonia, atelectasis, or chronic obstructive pulmonary disease (COPD), particularly affecting the lower lobes.
To effectively auscultate the posterior chest wall, the patient is usually positioned sitting upright or leaning forward slightly, exposing the back fully. The healthcare provider systematically listens to the lower lobe areas, moving the stethoscope in a methodical manner to ensure comprehensive coverage. This approach ensures that vesicular sounds are accurately assessed, and any abnormalities are detected early. The posterior chest wall, therefore, serves as a critical auscultation site for diagnosing and monitoring respiratory conditions.
In summary, the posterior chest wall, especially over the lower lobes, is a primary location for hearing vesicular sounds due to its anatomical advantages and acoustic properties. Clinicians rely on this area to evaluate lung health, leveraging the clarity and consistency of sounds produced during normal breathing. Proper auscultation techniques in this region are essential for accurate diagnosis and management of respiratory disorders, making it a cornerstone of pulmonary assessment.
Understanding the Duration of J3 Alarm Sound: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Lateral Chest Wall: Vesicular sounds are audible along the lateral chest wall, extending from apex to base
Vesicular sounds, a type of lung sound characterized by soft, low-pitched, and rustling qualities, are a fundamental component of respiratory auscultation. When assessing the lateral chest wall, these sounds are consistently audible, extending from the apex (the uppermost region of the lung) to the base (the lowest region). This continuity of vesicular sounds along the lateral aspect is a normal finding and reflects the healthy air movement through the alveoli during respiration. The lateral chest wall provides a broad surface area for auscultation, allowing healthcare providers to evaluate lung function across different lung segments effectively.
The lateral chest wall is particularly important for auscultation because it overlies multiple lung segments, including the upper, middle, and lower lobes. As air moves in and out of the alveoli, it creates the characteristic vesicular sound, which is more pronounced during inspiration due to the longer duration of airflow. During auscultation, the clinician should move the stethoscope systematically from the apex to the base, ensuring that vesicular sounds are present and consistent throughout. Any deviation, such as diminished or absent sounds, could indicate an underlying pathology like consolidation, pneumothorax, or pleural effusion.
When listening along the lateral chest wall, it is essential to compare findings between the left and right sides to identify asymmetry. Vesicular sounds should be symmetrical, as both lungs are typically involved in normal respiration. The lateral wall is also a key area to assess for changes in sound intensity or quality, which can provide clues about conditions such as chronic obstructive pulmonary disease (COPD) or asthma. For example, prolonged expiratory phases with wheezing may be heard in asthmatic patients, while diminished vesicular sounds could suggest airflow obstruction.
Instructively, to properly evaluate the lateral chest wall, the patient should be positioned in a seated or supine posture with the chest wall fully exposed. The stethoscope should be placed lightly on the skin to avoid altering the sound quality. Begin at the apex, located just above the clavicle, and move downward to the base, near the sixth to eighth rib. Each location should be assessed during both inspiration and expiration to ensure the vesicular sounds are normal and consistent. This methodical approach ensures a thorough examination of the lateral chest wall and aids in detecting any abnormalities.
Finally, understanding the normal distribution of vesicular sounds along the lateral chest wall is crucial for differentiating between healthy lung function and pathological conditions. The presence of vesicular sounds from apex to base confirms adequate air entry and alveolar ventilation. However, clinicians must remain vigilant for variations in sound quality, intensity, or duration, as these can indicate localized or diffuse lung disease. Mastery of auscultation techniques in this region enhances diagnostic accuracy and guides appropriate clinical management.
Ring Cameras: Indoor Audio and Video Surveillance
You may want to see also
Explore related products






![]()
Apical Region: In the apical region, vesicular sounds are higher pitched and shorter in duration
Vesicular sounds, which are a type of lung sound, are typically heard during auscultation of the chest and provide valuable information about respiratory function. When examining the various regions of the lungs, the apical region stands out for its unique acoustic characteristics. Located at the uppermost part of the lung fields, the apical region is accessible for auscultation just above the clavicle and extending slightly downward along the sides of the neck. In this area, vesicular sounds exhibit distinct qualities that differentiate them from sounds heard in other lung regions.
In the apical region, vesicular sounds are notably higher pitched compared to those heard in the basal or mid-lung regions. This higher pitch is a result of the anatomical structure and air flow dynamics within the upper lung segments. The air columns in these areas are shorter, and the alveoli are generally smaller, contributing to the production of sounds with a higher frequency. Clinicians can identify this characteristic pitch as a key indicator of the sound's origin during auscultation.
##
The duration of vesicular sounds in the apical region is another important feature. These sounds tend to be shorter in length, often described as brief or rapid. This is due to the faster air movement and the unique geometry of the upper airways, which allow for quicker air exchange. As a person inhales, the sound begins and ends more abruptly in the apical region, providing a distinct auditory pattern for healthcare professionals to recognize.
Auscultating the apical region requires careful placement of the stethoscope to capture these sounds effectively. Medical practitioners should position the stethoscope lightly on the skin, ensuring a good seal to minimize ambient noise interference. By doing so, they can clearly discern the higher-pitched and shorter vesicular sounds, which are essential for assessing respiratory health in this specific lung area. Understanding these regional variations in lung sounds is crucial for accurate diagnosis and monitoring of respiratory conditions.
The apical region's vesicular sounds offer a window into the functioning of the upper lung segments. Their higher pitch and shorter duration are not merely auditory curiosities but essential diagnostic tools. By recognizing these characteristics, healthcare providers can pinpoint the origin of lung sounds and make informed decisions regarding patient care, especially in the context of respiratory diseases or conditions affecting specific lung regions. This knowledge is fundamental in the clinical assessment of respiratory function and overall patient health.
Sexual Sounds: Sin or Natural Instinct?
You may want to see also
Explore related products

$34.72




![]()
Basal Region: The basal region exhibits longer, softer vesicular sounds due to increased airflow resistance
The basal region of the lungs, located near the chest wall and closer to the diaphragm, is a key area where vesicular sounds can be heard during auscultation. These sounds are characterized by their longer duration and softer quality, which are primarily due to increased airflow resistance in this region. When air moves through the larger bronchi and bronchioles of the basal region, it encounters more resistance compared to the upper lung fields. This resistance is a result of the narrower airways and the increased tissue density in the lower parts of the lungs. As a result, the airflow becomes more turbulent, producing the distinctive vesicular sounds that are softer and more prolonged.
Increased airflow resistance in the basal region is influenced by several anatomical and physiological factors. The airways in this area are more horizontal and have a greater cross-sectional area, which contributes to the slower movement of air. Additionally, the basal region is subject to greater pressure changes during respiration due to its proximity to the diaphragm. During inspiration, the diaphragm descends, creating a negative pressure that pulls air into the lungs, but this effect is more pronounced in the basal region, leading to a slower and more controlled airflow. This slower airflow is what gives the vesicular sounds their softer and more extended nature.
Clinicians often focus on the basal region during auscultation because it provides valuable information about lung function and potential abnormalities. The longer, softer vesicular sounds heard here are considered normal and indicate healthy airflow dynamics in the lower lung fields. However, any deviation from these characteristics, such as shortened or harsher sounds, may suggest the presence of conditions like consolidation, effusion, or atelectasis. Understanding the typical sound patterns in the basal region is crucial for differentiating between normal and pathological findings, making it an essential skill for healthcare professionals.
To effectively auscultate the basal region, proper technique is essential. The patient should be positioned in a way that allows easy access to the lower chest wall, such as sitting upright or leaning forward. The stethoscope diaphragm is then placed firmly on the skin over the basal region, ensuring a good seal to capture the sounds accurately. By comparing the sounds heard in the basal region to those in other lung fields, clinicians can assess the consistency of airflow and identify any regional differences that may indicate underlying issues. Mastery of this technique enables healthcare providers to make informed diagnoses and monitor respiratory health effectively.
In summary, the basal region of the lungs exhibits longer, softer vesicular sounds due to increased airflow resistance, which is a result of anatomical and physiological factors unique to this area. These sounds are a normal finding during auscultation and provide important insights into lung function. By understanding the mechanisms behind these sounds and employing proper auscultation techniques, clinicians can enhance their diagnostic capabilities and ensure comprehensive respiratory assessments. The basal region, therefore, remains a critical area of focus in the evaluation of lung health.
Is the 'Sissy Villain' Stereotype Homophobic?
You may want to see also
Frequently asked questions
Vesicular sounds are typically heard over the peripheral lung fields, particularly in the upper and mid zones of the lungs.
No, vesicular sounds are louder and more prominent in the peripheral lung fields compared to the central or apical regions.
No, vesicular sounds are not heard over the trachea; they are specific to the lung parenchyma during auscultation.
Vesicular sounds are more pronounced in the peripheral lung fields because these areas have a higher concentration of alveoli and smaller airways, where air movement is more audible.
Yes, vesicular sounds are heard throughout inspiration and are softer and shorter during expiration, with a gradual decrease in intensity.