Bronchovesicular sounds are a type of lung sound that combines characteristics of both bronchial and vesicular breath sounds, representing an intermediate pattern. They are typically heard over the trachea, mainstem bronchi, and areas where the lungs are denser or closer to the chest wall, such as the upper part of the lung fields or over the first and second intercostal spaces. These sounds are often described as medium in pitch and intensity, with a slight degree of harshness, reflecting the airflow through medium-sized airways. Understanding where bronchovesicular sounds are heard is crucial for clinicians, as their presence or absence in specific anatomical locations can provide valuable insights into respiratory health and potential underlying conditions.
| Characteristics | Values |
|---|---|
| Location | Over the trachea, mainstem bronchi, and near the lungs' upper regions |
| Intensity | Louder than vesicular sounds but softer than bronchial sounds |
| Pitch | Medium-pitched |
| Duration | Equal inspiration and expiration phases |
| Quality | Harsh or rough sound |
| Anatomical Association | Heard over the manubrium sterni and between the scapulae |
| Normal vs. Abnormal | Normal over specific areas; abnormal if heard elsewhere |
| Clinical Significance | Indicates air passage through larger airways |
| Comparison to Vesicular Sounds | Longer and louder expiratory phase than vesicular sounds |
| Comparison to Bronchial Sounds | Softer and less high-pitched than bronchial sounds |
Explore related products




What You'll Learn
- Anterior Chest Wall: Heard over manubrium, 2nd intercostal space, and upper sternal border
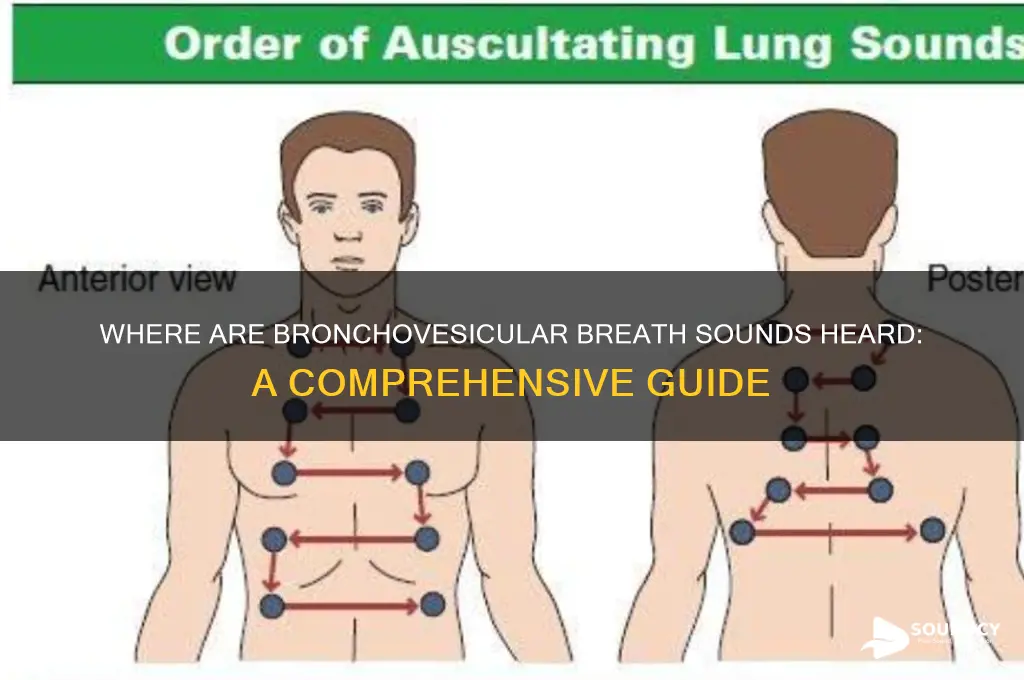
- Posterior Chest Wall: Audible between scapulae, over spine, and lower thoracic region
- Lateral Chest Wall: Detected at 1st–2nd intercostal spaces along midclavicular lines
- Pathological Conditions: Increased intensity in consolidation, pneumonia, or lung abscess areas
- Normal Variants: Prominent in thin individuals or during deep inspiration in healthy lungs
![]()
Anterior Chest Wall: Heard over manubrium, 2nd intercostal space, and upper sternal border
Bronchovesicular sounds are a type of lung sound that represents a blend between bronchial and vesicular breath sounds. These sounds are characterized by their medium pitch and intermediate duration, making them distinct from both the higher-pitched bronchial sounds and the softer, longer vesicular sounds. When auscultating the anterior chest wall, specific locations are key to identifying where bronchovesicular sounds are typically heard. One such area is over the manubrium, the 2nd intercostal space, and the upper sternal border. These locations are particularly important because they correspond to areas where larger airways are closer to the chest wall, allowing for the transmission of bronchovesicular sounds.
The manubrium, located at the top of the sternum, is a prime location for auscultating bronchovesicular sounds. This area overlies the trachea and the upper portions of the main bronchi, where air movement produces sounds that are neither purely bronchial nor vesicular. Clinicians should place the stethoscope firmly over the manubrium to listen for these sounds, ensuring proper contact to avoid missing subtle auditory cues. The manubrium’s proximity to the trachea makes it an ideal spot to detect changes in lung sounds that may indicate conditions such as partial obstruction or inflammation in the larger airways.
Moving downward, the 2nd intercostal space is another critical area for auscultating bronchovesicular sounds on the anterior chest wall. This space is located just below the manubrium and corresponds to the level of the aortic arch and the upper parts of the lungs. Here, the airways are still relatively large, and the chest wall is thin enough to allow clear transmission of lung sounds. Clinicians should listen bilaterally in the 2nd intercostal space to compare sounds between the left and right sides, as asymmetry may indicate localized pathology. Proper technique involves ensuring the patient is in a comfortable position, such as sitting upright, to optimize sound detection.
The upper sternal border is the final key area on the anterior chest wall where bronchovesicular sounds are heard. This region extends from the manubrium to the angle of Louis, where the manubrium meets the body of the sternum. The upper sternal border overlies the upper lobes of the lungs and the larger bronchi, making it an important site for auscultation. When listening here, clinicians should pay attention to the quality and intensity of the sounds, as changes may suggest conditions like pneumonia, chronic obstructive pulmonary disease (COPD), or other respiratory disorders. Consistent and systematic auscultation of this area is essential for a thorough lung examination.
In summary, bronchovesicular sounds on the anterior chest wall are best heard over the manubrium, the 2nd intercostal space, and the upper sternal border. These locations are strategically important due to their proximity to larger airways, which produce the characteristic medium-pitched, intermediate-duration sounds. Proper auscultation techniques, including firm stethoscope placement and bilateral comparison, are crucial for accurately detecting and interpreting these sounds. Understanding the anatomical basis of these auscultation sites enhances the clinician’s ability to diagnose and manage respiratory conditions effectively.
Sound Bug Repellents: Are They Safe?
You may want to see also
Explore related products






![]()
Posterior Chest Wall: Audible between scapulae, over spine, and lower thoracic region
Bronchovesicular sounds are a type of lung sound that combines characteristics of both bronchial and vesicular breath sounds. They are typically heard in areas where the trachea or large bronchi are located closer to the surface, but they can also be auscultated in specific regions of the posterior chest wall. One such area is the posterior chest wall, particularly between the scapulae, over the spine, and in the lower thoracic region. These locations are important for clinicians to assess, as they provide valuable information about the respiratory system.
When auscultating the posterior chest wall, the area between the scapulae is a key focus. This region is significant because it overlies the lower trachea and the bifurcation of the bronchi. Here, bronchovesicular sounds are often audible due to the proximity of the larger airways. These sounds are characterized by their medium pitch and intensity, with a slight expiratory prolongation. Clinicians should listen carefully in this area, as abnormalities in sound quality or intensity may indicate conditions such as partial obstruction, inflammation, or consolidation in the lower airways.
Moving over the spine, particularly in the mid-to-lower thoracic region, bronchovesicular sounds can also be heard. This area corresponds to the posterior aspects of the lungs, where the mainstem bronchi and their immediate branches are located. The sounds here are similar to those heard between the scapulae but may vary slightly in pitch or intensity depending on the patient’s anatomy and respiratory effort. It is crucial to compare findings from both sides of the spine to identify asymmetries, which could suggest localized pathology such as pneumonia or atelectasis.
The lower thoracic region of the posterior chest wall is another important site for auscultation. This area is particularly relevant for assessing the basal segments of the lower lobes. Bronchovesicular sounds in this region are expected due to the anatomical relationship between the skin surface and the underlying bronchi. Clinicians should pay attention to the transition from bronchovesicular to vesicular sounds as they move laterally, as an abnormal persistence of bronchovesicular sounds could indicate conditions like chronic obstructive pulmonary disease (COPD) or bronchiectasis.
In summary, the posterior chest wall, specifically between the scapulae, over the spine, and in the lower thoracic region, is a critical area for auscultating bronchovesicular sounds. These locations are anatomically linked to the larger airways, making them ideal for assessing respiratory health. Clinicians should systematically evaluate these regions, noting the quality, pitch, and symmetry of the sounds to detect early signs of respiratory abnormalities. Mastery of auscultation in these areas enhances diagnostic accuracy and patient care.
Identifying Bad Car Starter Sounds: Symptoms, Causes, and Solutions
You may want to see also
Explore related products






![]()
Lateral Chest Wall: Detected at 1st–2nd intercostal spaces along midclavicular lines
Bronchovesicular breath sounds are a type of lung sound that represents a blend between bronchial and vesicular sounds, often described as medium in pitch and intensity. These sounds are typically heard in specific areas of the chest where larger airways are closer to the surface, allowing for the transmission of these characteristic sounds. One such location is the lateral chest wall, specifically at the 1st–2nd intercostal spaces along the midclavicular lines. This area is particularly important for auscultation as it provides valuable insights into the respiratory health of the upper lobes of the lungs.
When assessing the lateral chest wall, the 1st and 2nd intercostal spaces along the midclavicular lines are anatomically positioned over the upper lobes of the lungs. This region is ideal for detecting bronchovesicular sounds because the larger airways (bronchi) are relatively close to the chest wall, facilitating the transmission of these sounds. To auscultate this area effectively, the patient should be in a comfortable seated or supine position, with the chest exposed. The healthcare provider should place the stethoscope diaphragm (for lower-pitched sounds) firmly but gently on the skin, ensuring a good seal to minimize ambient noise.
Bronchovesicular sounds in this area are considered normal during inspiration and expiration. They are often heard bilaterally and symmetrically, indicating healthy airflow through the upper airways. However, any asymmetry or deviation from normal sounds in this region may suggest pathology, such as consolidation, obstruction, or inflammation in the upper lobes. For example, an increase in bronchovesicular sounds (amplification) could indicate conditions like pneumonia or bronchiectasis, while a decrease or absence of these sounds might suggest pneumothorax or pleural effusion.
It is crucial to compare findings between the left and right sides when auscultating the 1st–2nd intercostal spaces along the midclavicular lines. This comparison helps in identifying unilateral abnormalities that may otherwise be missed. Additionally, the technique of auscultation should be systematic, moving from one intercostal space to the next, to ensure comprehensive coverage of the lateral chest wall. Proper patient positioning and a quiet environment are also essential to accurately detect and interpret bronchovesicular sounds in this area.
In summary, the lateral chest wall, particularly at the 1st–2nd intercostal spaces along the midclavicular lines, is a key location for detecting bronchovesicular breath sounds. These sounds provide important clinical information about the upper lobes of the lungs. Healthcare providers should be adept at auscultating this area, ensuring proper technique and patient positioning to accurately assess respiratory health. Recognizing normal versus abnormal sounds in this region is critical for diagnosing and managing respiratory conditions effectively.
Mastering Tight Mixes: Pro Techniques for Professional Sound Clarity
You may want to see also
Explore related products






![]()
Pathological Conditions: Increased intensity in consolidation, pneumonia, or lung abscess areas
Bronchovesicular sounds are typically heard over the trachea, mainstem bronchi, and areas where the larger bronchi lie close to the surface, such as the second and third intercostal spaces anteriorly and over the lower trachea. These sounds are a blend of bronchial and vesicular breath sounds, characterized by a medium pitch and intermediate duration. However, in certain pathological conditions, the intensity of bronchovesicular sounds can increase, particularly in areas of consolidation, pneumonia, or lung abscess. This phenomenon is crucial for clinicians to recognize, as it provides valuable diagnostic information about the underlying lung pathology.
In consolidation, which often occurs in conditions like pneumonia, the air-filled alveoli are replaced by fluid, inflammatory cells, or pus. This alteration in lung parenchyma increases the transmission of sound, leading to amplified bronchovesicular sounds in the affected areas. For instance, in lobar pneumonia, the consolidation is typically confined to a specific lobe or segment, and the increased intensity of bronchovesicular sounds can be localized to that region. Auscultation reveals these sounds to be louder and more pronounced compared to normal, often described as "enhanced" or "brassy." This finding is a key indicator of the inflammatory process and the presence of consolidated lung tissue.
Pneumonia itself, whether bacterial, viral, or fungal, often results in increased bronchovesicular sound intensity due to the inflammatory exudate filling the alveolar spaces. The sounds become more prominent as the air passages are surrounded by inflamed tissue, which conducts sound more efficiently. Additionally, the presence of bronchial breathing, a variation of bronchovesicular sounds with a more tubular quality, may be heard in areas of dense consolidation. This is particularly true in bacterial pneumonia, where the infection leads to significant alveolar filling and airway inflammation, further amplifying the sounds.
Lung abscess, another pathological condition characterized by localized necrosis and pus formation within the lung parenchyma, also leads to increased intensity of bronchovesicular sounds. The abscess creates a cavity filled with fluid and debris, which alters the acoustic properties of the lung tissue. As a result, auscultation over the abscess area reveals louder bronchovesicular sounds, often accompanied by adventitious sounds like crackles or rhonchi due to the presence of secretions and inflamed airways. This finding is especially useful in distinguishing lung abscess from other conditions, as the localized nature of the abscess typically confines the amplified sounds to a specific area.
Clinicians should be attentive to the localization and quality of these amplified bronchovesicular sounds, as they provide clues to the extent and nature of the underlying pathology. For example, in pneumonia, the sounds may be heard over an entire lobe, while in lung abscess, they are usually confined to a smaller, more discrete area. Recognizing these patterns aids in differentiating between conditions and guiding further diagnostic and therapeutic interventions. In summary, increased intensity of bronchovesicular sounds in areas of consolidation, pneumonia, or lung abscess is a critical auscultatory finding that reflects the pathological changes in lung tissue and assists in the clinical assessment of respiratory diseases.
How Long Does ADT Alarm Sound: Duration and Safety Insights
You may want to see also
Explore related products




![]()
Normal Variants: Prominent in thin individuals or during deep inspiration in healthy lungs
Bronchovesicular sounds are a type of lung sound that represents a blend between bronchial and vesicular breath sounds. Normally, these sounds are heard over the trachea and mainstem bronchi, but they can also be prominent in specific conditions or anatomical variations. One such normal variant is their prominence in thin individuals or during deep inspiration in healthy lungs. This phenomenon occurs due to the reduced soft tissue between the lung fields and the chest wall, allowing the transmission of these sounds more clearly. In thin individuals, the lack of subcutaneous fat enhances the conduction of bronchovesicular sounds, making them more audible during auscultation.
During deep inspiration, the increased volume of air moving through the larger airways amplifies bronchovesicular sounds in healthy lungs. This is particularly noticeable over areas where the bronchi are closer to the chest wall, such as the upper lobe regions. Deep breaths cause greater turbulence in the airways, which contributes to the louder and more pronounced nature of these sounds. It is important for healthcare providers to recognize this as a normal variant to avoid misinterpretation as pathology. Auscultation during both shallow and deep breathing can help differentiate between normal and abnormal findings.
In thin individuals, bronchovesicular sounds may be heard more prominently over a larger area of the lung fields compared to individuals with more soft tissue. This is because the sounds are not dampened by adipose tissue, allowing them to travel more freely to the chest wall. Clinicians should be aware of this anatomical variation to avoid misdiagnosis, especially in patients with low body mass index (BMI). Proper patient positioning and careful auscultation techniques are essential to accurately assess these sounds and distinguish them from abnormal breath sounds.
During deep inspiration, the pitch of bronchovesicular sounds may also increase slightly due to the higher flow rate of air through the airways. This is a physiological response and should not be confused with pathologic conditions such as consolidation or obstruction. Educating medical students and practitioners about these normal variants is crucial for accurate lung auscultation. Repeated practice and comparison between different patient profiles can enhance the ability to identify these sounds correctly.
In summary, the prominence of bronchovesicular sounds in thin individuals or during deep inspiration in healthy lungs is a normal variant that results from anatomical and physiological factors. Reduced soft tissue in thin individuals and increased airflow during deep breaths enhance the transmission and audibility of these sounds. Recognizing this variant is essential for accurate clinical assessment and to prevent unnecessary investigations. Healthcare providers should remain vigilant and consider patient-specific factors when interpreting lung sounds to ensure precise diagnosis and management.
Master Chrome Sound Settings: Easy Steps to Adjust Audio Levels
You may want to see also
Frequently asked questions
Bronchovesicular sounds are typically heard over the trachea, mainstem bronchi, and at the level of the first and second intercostal spaces.
Bronchovesicular sounds are intermediate between bronchial and vesicular sounds, with a balance of higher-pitched inspiratory and lower-pitched expiratory phases.
Yes, bronchovesicular sounds are normal over the suprasternal notch, between the scapulae, and over the lung fields adjacent to the sternum.
Abnormal bronchovesicular sounds in areas where vesicular sounds are expected may indicate consolidation, pneumonia, or other pathological conditions affecting the lungs.