Heart sounds occur during the cardiac cycle, which is the sequence of events in the heart as it beats. These sounds are primarily produced by the closing of the heart valves and the resulting vibrations transmitted through the heart structures and surrounding tissues. The first heart sound (S1) coincides with the closure of the mitral and tricuspid valves at the beginning of systole, marking the start of ventricular contraction. The second heart sound (S2) occurs at the end of systole, corresponding to the closure of the aortic and pulmonary valves as the ventricles finish ejecting blood. Additional heart sounds, such as S3 and S4, may be heard in certain conditions and are associated with early diastolic filling and late diastolic atrial contraction, respectively. Understanding when these sounds occur is crucial for diagnosing cardiac abnormalities and assessing heart function.
Explore related products






What You'll Learn
- Systolic Sounds: Occur when the heart contracts, blood is ejected from ventricles
- Diastolic Sounds: Happen when the heart relaxes, ventricles fill with blood
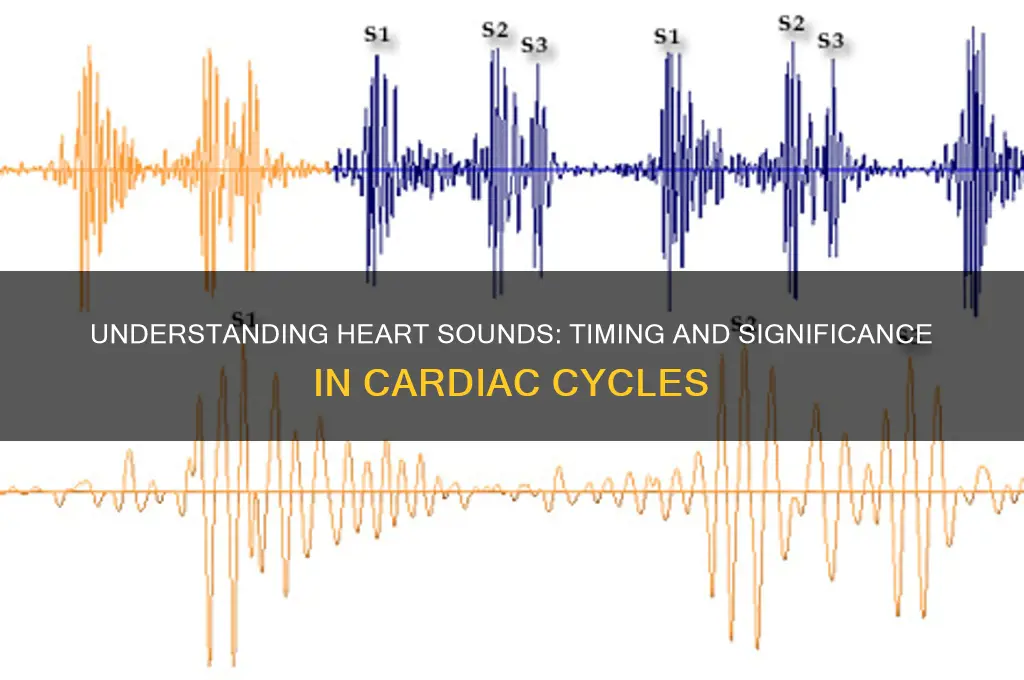
- First Heart Sound (S1): Marks mitral/tricuspid valve closure at the start of systole
- Second Heart Sound (S2): Indicates aortic/pulmonic valve closure at the end of systole
- Extra Heart Sounds: Include S3 (early diastole) and S4 (late diastole) in pathologies
![]()
Systolic Sounds: Occur when the heart contracts, blood is ejected from ventricles
Systolic sounds are the audible markers of the heart’s most forceful action: the contraction of its ventricles. When the left ventricle contracts, it ejects oxygen-rich blood into the aorta, while the right ventricle propels oxygen-poor blood into the pulmonary artery. This phase of the cardiac cycle, known as systole, generates the first and loudest heart sound, often described as “lub.” Clinicians use stethoscopes to detect abnormalities in this sound, such as murmurs or splits, which can indicate valve dysfunction or blood flow issues. Understanding systolic sounds is critical for diagnosing conditions like aortic stenosis or mitral regurgitation, where the heart’s efficiency is compromised during contraction.
To identify systolic sounds, place the stethoscope’s diaphragm over the heart’s apex (fifth intercostal space, mid-clavicular line) or the aortic area (second right intercostal space). The “lub” sound corresponds to the closure of the atrioventricular (AV) valves—mitral and tricuspid—as the ventricles contract. This sound is typically low-pitched and lasts about 0.14 seconds in adults. For pediatric patients, the duration may vary slightly due to faster heart rates. Practicing auscultation on diverse populations helps differentiate normal systolic sounds from pathological ones, ensuring accurate assessments.
Systolic sounds are not just auditory cues; they reflect the heart’s mechanical performance. For instance, a systolic murmur heard best at the apex may suggest mitral valve prolapse, while one at the base could indicate aortic stenosis. To evaluate these murmurs, clinicians use the Levine scale (grading from 1 to 6) to quantify their intensity. Patients with grade 3 or higher murmurs often require further imaging, such as echocardiography, to assess structural abnormalities. Early detection through careful auscultation can prevent complications like heart failure or arrhythmias.
Comparatively, systolic sounds differ from diastolic sounds in timing and significance. While systole is about ejection, diastole involves filling. Systolic sounds are louder and more dominant, making them easier to detect in routine examinations. However, their prominence also means abnormalities are less likely to be overlooked. For example, a systolic click followed by a murmur is a classic sign of mitral valve prolapse, whereas a diastolic rumble suggests aortic regurgitation. Mastering the nuances of systolic sounds enhances diagnostic precision, ensuring timely interventions for cardiac health.
Crafting the Perfect Turbo Miata Exhaust Note: Sound and Performance Tips
You may want to see also
Explore related products






![]()
Diastolic Sounds: Happen when the heart relaxes, ventricles fill with blood
Heart sounds are the symphony of cardiac activity, but not all notes are created equal. Diastolic sounds, in particular, occur during the heart's relaxation phase, when the ventricles fill with blood. This quieter, often overlooked period is just as critical as the heart's contraction, offering valuable insights into cardiovascular health. Understanding these sounds can help differentiate between normal function and potential issues like valve dysfunction or fluid overload.
Consider the diastolic murmur, a soft whooshing sound that may indicate blood flowing through a stenotic mitral valve. Unlike systolic sounds, which are louder and more pronounced, diastolic murmurs require careful auscultation, often best heard with the bell of a stethoscope. For instance, a low-pitched, rumbling murmur in early diastole could signal mitral stenosis, while a high-pitched, decrescendo murmur in late diastole might point to aortic regurgitation. Recognizing these nuances is essential for accurate diagnosis, especially in older adults where valvular disease is more prevalent.
To effectively assess diastolic sounds, follow these steps: position the patient in the left lateral decubitus position, place the stethoscope over the appropriate valve area, and listen intently during the heart’s relaxation phase. For mitral valve assessment, focus on the apex; for aortic regurgitation, the aortic area is key. Caution: environmental noise or rushed auscultation can lead to misinterpretation. Pairing this technique with echocardiography can provide a comprehensive evaluation, ensuring no subtle abnormalities are missed.
The takeaway is clear: diastolic sounds are a window into the heart’s passive filling phase, revealing critical details about valve function and blood flow dynamics. While systolic sounds dominate the cardiac soundtrack, diastolic murmurs demand equal attention. For healthcare providers, mastering this skill enhances diagnostic accuracy, particularly in populations at higher risk for valvular disease. Patients, too, benefit from this knowledge, as early detection can lead to timely interventions and improved outcomes.
Boost Your Productivity: Discover the Best Sounds for Focus and Concentration
You may want to see also
Explore related products






![]()
First Heart Sound (S1): Marks mitral/tricuspid valve closure at the start of systole
The first heart sound, often abbreviated as S1, is a critical marker in the cardiac cycle, signaling the closure of the mitral and tricuspid valves at the onset of systole. This sound is best heard at the apex of the heart, where the mitral valve is positioned, and is characterized by a low-pitched, dull “lub” sound. It occurs when the ventricles begin to contract, generating enough pressure to push the mitral and tricuspid valves shut, preventing blood from flowing back into the atria. Understanding S1 is essential for clinicians, as its timing, quality, and intensity provide valuable insights into cardiac function and potential abnormalities.
Analyzing S1 requires a systematic approach. Begin by positioning the stethoscope at the apex, typically in the fifth intercostal space at the midclavicular line. Listen for the distinct “lub” that coincides with the electrocardiogram (ECG) R wave, marking the start of ventricular contraction. A split S1, where the mitral and tricuspid components are audible separately, may indicate conditions like right bundle branch block or atrial enlargement. Conversely, a single, prolonged S1 could suggest stiffened valves or reduced ventricular compliance. Clinicians should correlate these findings with patient history and other diagnostic tools for accurate interpretation.
From a practical standpoint, teaching medical students and trainees to identify S1 involves emphasizing its relationship to systole. A useful mnemonic is “Lub = Systole Starts,” linking the sound to the beginning of ventricular contraction. Encourage learners to practice auscultation on diverse patients, noting variations in S1 based on age, heart rate, and pathology. For instance, children and athletes often exhibit louder S1 due to more vigorous myocardial contraction, while elderly patients may have softer sounds due to valve thickening. Hands-on training with simulated heart sounds can also enhance proficiency before clinical encounters.
Comparatively, S1 differs from the second heart sound (S2) in both timing and physiology. While S1 marks the closure of the atrioventricular valves (mitral and tricuspid), S2 signifies the closure of the semilunar valves (aortic and pulmonary) at the end of systole. This distinction is crucial for differentiating between systolic and diastolic events. For example, a widened splitting of S2 is often associated with delayed closure of the pulmonary valve, as seen in pulmonary hypertension, whereas S1 abnormalities typically reflect issues with ventricular filling or contraction. Recognizing these differences ensures accurate diagnosis and targeted interventions.
In conclusion, the first heart sound (S1) is a fundamental auscultatory finding that marks the transition from diastole to systole, reflecting mitral and tricuspid valve closure. Its characteristics—pitch, duration, and timing—offer clues to underlying cardiac health. By mastering S1 identification and interpretation, healthcare providers can enhance their diagnostic skills, ensuring timely and effective patient care. Regular practice, combined with an understanding of physiological and pathological variations, solidifies S1 as a cornerstone of cardiac auscultation.
Echoes of the Past: Reconstructing the Lost Voices of Extinct Species
You may want to see also
Explore related products






![]()
Second Heart Sound (S2): Indicates aortic/pulmonic valve closure at the end of systole
The second heart sound (S2) is a critical marker in the cardiac cycle, signaling the end of systole with the closure of the aortic and pulmonic valves. This sound is typically described as a sharp, high-pitched "dub" and is best heard at the base of the heart. Clinicians rely on S2 to assess the timing and efficiency of valve function, as abnormalities in its intensity or splitting can indicate conditions such as aortic stenosis or pulmonary hypertension. Understanding S2 is essential for diagnosing cardiovascular issues and ensuring proper heart function.
To auscultate S2 effectively, position the patient in a supine or left lateral decubitus position, using a diaphragm stethoscope placed lightly on the chest. The sound is most distinct at the second right intercostal space (aortic component) and the third left intercostal space (pulmonic component). Note the physiological splitting of S2 during inspiration, where the pulmonic valve closes slightly later than the aortic valve due to increased blood return to the right heart. This splitting disappears during expiration, providing a useful diagnostic clue.
From a comparative perspective, S2 contrasts with the first heart sound (S1), which marks the beginning of systole with mitral and tricuspid valve closure. While S1 is lower-pitched and longer in duration, S2 is shorter and higher-pitched, reflecting the rapid closure of the semilunar valves. This distinction is crucial for differentiating between normal and pathological heart sounds. For instance, a widened or fixed splitting of S2 may suggest left bundle branch block or atrial septal defect, respectively.
Practically, monitoring S2 is particularly important in pediatric and elderly populations, where valve function can be more susceptible to abnormalities. In children, a delayed or absent S2 may indicate congenital heart defects, while in older adults, calcification of the aortic valve can cause a diminished or harsh S2. Regular auscultation, combined with echocardiography, can help track changes over time and guide interventions such as valve replacement or medication adjustments. Mastery of S2 interpretation is thus a cornerstone of cardiovascular care.
Unveiling the Unique Vocalizations: What Sounds Do Raccoons Make?
You may want to see also
Explore related products






![]()
Extra Heart Sounds: Include S3 (early diastole) and S4 (late diastole) in pathologies
Heart sounds beyond the familiar S1 and S2 can signal underlying pathologies, particularly when S3 and S4 gallops emerge. These extra sounds occur during diastole, the heart's relaxation phase, and their presence often indicates increased ventricular stiffness or volume overload. S3, a low-pitched sound in early diastole, is sometimes benign in children and well-trained athletes but raises concern in adults, suggesting conditions like heart failure or mitral regurgitation. S4, a higher-pitched sound in late diastole, typically signifies left ventricular hypertrophy or ischemia, reflecting impaired ventricular compliance.
To identify these sounds, auscultate with the bell of the stethoscope at the apex, positioning the patient in the left lateral decubitus position. S3 is best heard during expiration, while S4 is more prominent during inspiration. Both sounds are soft and require a quiet environment and focused listening. Misidentification is common, so correlate findings with echocardiography or Doppler studies for confirmation. For instance, an S3 in a 60-year-old with dyspnea and elevated BNP levels strongly suggests heart failure with preserved ejection fraction (HFpEF).
Clinicians must differentiate between S3 and S4 to guide management. S3 in heart failure often responds to diuretics and ACE inhibitors, reducing ventricular preload. S4, however, may require beta-blockers or calcium channel blockers to address hypertension or ischemia. In pediatric patients, an S3 is often physiological, but persistent S4 warrants investigation for congenital heart defects or systemic hypertension. Always consider patient age, comorbidities, and hemodynamic status when interpreting these sounds.
A comparative analysis reveals that S3 and S4 share diastolic timing but differ in etiology and management. S3 reflects rapid ventricular filling, while S4 indicates atrial contraction against a stiff ventricle. Both sounds are more common in older adults, particularly those with long-standing hypertension or valvular disease. For example, a 70-year-old with uncontrolled hypertension may exhibit both S3 and S4, highlighting the need for aggressive blood pressure control and serial echocardiograms.
In practice, documenting the presence, timing, and characteristics of S3 and S4 is critical. Use descriptive terms like "soft," "loud," or "rumbling" to aid in diagnosis. Educate patients about the significance of these sounds, emphasizing the importance of medication adherence and lifestyle modifications. For instance, a patient with S4 due to left ventricular hypertrophy benefits from sodium restriction and regular aerobic exercise. By integrating auscultation findings with diagnostic tools, clinicians can tailor interventions to address the root causes of these extra heart sounds.
Adobe's Sound Design: Creative Audio Tools
You may want to see also
Frequently asked questions
Heart sounds occur during the closing and opening of the heart valves. The first heart sound (S1) occurs at the beginning of systole when the mitral and tricuspid valves close, while the second heart sound (S2) occurs at the beginning of diastole when the aortic and pulmonary valves close.
No, heart sounds are not continuous. They occur as brief, distinct sounds corresponding to specific valve movements during systole and diastole, with periods of silence in between.
The third heart sound (S3), if present, occurs in early diastole, shortly after S2. It is associated with rapid filling of the ventricles and is often heard in certain conditions like heart failure or volume overload.
The fourth heart sound (S4), if present, occurs in late diastole, just before S1. It is associated with atrial contraction and is often heard in conditions like hypertension or left ventricular hypertrophy.































