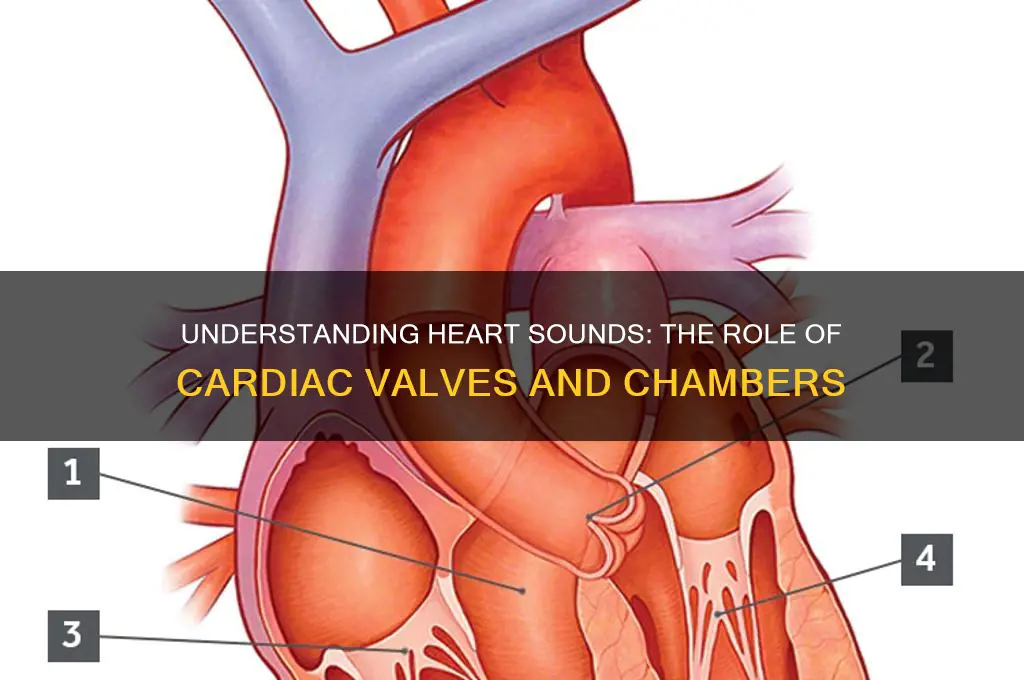
The heart sounds we hear through a stethoscope are primarily created by the movement of the heart valves and the resulting vibrations transmitted through the blood, surrounding tissues, and chest wall. These sounds, often described as lub-dub, correspond to the closing of the atrioventricular valves (mitral and tricuspid) during systole (the first sound, S1) and the closing of the semilunar valves (aortic and pulmonary) during diastole (the second sound, S2). The precise timing and quality of these sounds provide valuable insights into the heart's function and can help diagnose various cardiac conditions.
| Characteristics | Values |
|---|---|
| Structure Responsible for Heart Sounds | Heart valves |
| Specific Valves Involved | Mitral valve, Tricuspid valve, Aortic valve, Pulmonic valve |
| Primary Mechanism | Turbulent blood flow causing vibration of valve leaflets and surrounding structures |
| Number of Heart Sounds | Typically 2 (S1 and S2), but can include S3 and S4 in certain conditions |
| S1 (First Heart Sound) | Caused by closure of the mitral and tricuspid valves at the beginning of systole |
| S2 (Second Heart Sound) | Caused by closure of the aortic and pulmonic valves at the beginning of diastole |
| S3 (Third Heart Sound) | Associated with rapid filling of the ventricles in early diastole (normal in children, pathologic in adults) |
| S4 (Fourth Heart Sound) | Associated with atrial contraction against a stiff ventricle (pathologic, often seen in hypertrophic cardiomyopathy or aortic stenosis) |
| Factors Affecting Heart Sounds | Valve structure, blood flow velocity, ventricular compliance, heart rate |
| Clinical Significance | Abnormalities in heart sounds can indicate valve dysfunction, cardiac disease, or other pathologies |
| Diagnostic Tools | Auscultation with a stethoscope, echocardiography, Doppler ultrasound |
Explore related products





What You'll Learn
- Atrioventricular Valves: Closure of mitral/tricuspid valves causes first heart sound (S1)
- Semilunar Valves: Closure of aortic/pulmonic valves produces second heart sound (S2)
- Blood Turbulence: Abnormal flow creates murmurs, indicating valve issues or defects
- Ventricular Contraction: Generates S1 as valves shut, marking systole start
- Ventricular Relaxation: Allows blood flow, with S2 marking systole end
![]()
Atrioventricular Valves: Closure of mitral/tricuspid valves causes first heart sound (S1)
The rhythmic lub-dub of the heartbeat is a symphony orchestrated by the precise movements of cardiac structures. At the heart of this auditory phenomenon—literally—are the atrioventricular (AV) valves, specifically the mitral and tricuspid valves. Their closure marks the first heart sound, S1, a critical event in the cardiac cycle that signifies the transition from atrial contraction to ventricular systole. This sound is not merely a byproduct of the heart’s function but a vital diagnostic tool, offering clinicians insights into cardiac health.
Consider the mechanics: as the left and right atria contract, blood is propelled into the ventricles. Once the ventricles are filled, the AV valves snap shut to prevent backflow. This abrupt closure creates a low-pitched sound, S1, often described as the "lub" in the heartbeat. The mitral valve, with its two leaflets, guards the left side, while the tricuspid valve, with three leaflets, oversees the right. Their synchronized closure is a testament to the heart’s engineering precision, ensuring unidirectional blood flow. For healthcare providers, auscultating S1 provides immediate feedback on valve integrity and timing, making it a cornerstone of cardiac examination.
From a diagnostic perspective, abnormalities in S1 can signal underlying issues. A split first heart sound, for instance, may indicate delayed closure of the right AV valve compared to the left, often seen in conditions like right bundle branch block. Conversely, a single, prolonged S1 could suggest stiffened or fused valve leaflets. Clinicians often correlate these findings with patient history and imaging studies, such as echocardiography, to pinpoint the cause. For example, a middle-aged patient with a history of rheumatic fever might exhibit mitral stenosis, characterized by a loud, snapping S1. Recognizing these nuances is crucial for timely intervention.
Practical tips for auscultation include using the bell of the stethoscope for low-pitched S1 and positioning it at the apical region for the mitral component and the left sternal border for the tricuspid component. Patients should be in the left lateral decubitus position to optimize sound detection. For learners, correlating auscultation with visual aids, like animated cardiac cycles, can deepen understanding. Remember, S1’s quality, intensity, and timing are as important as its presence—each deviation tells a story about the AV valves’ function.
In essence, the closure of the mitral and tricuspid valves is not just a mechanical event but the genesis of S1, a sound that encapsulates the heart’s efficiency. By mastering its interpretation, healthcare professionals can detect early signs of valve dysfunction, ensuring proactive cardiac care. Whether in a medical student’s training or a seasoned physician’s practice, S1 remains a fundamental cue in the heart’s auditory narrative.
Mastering Digital Sound Editing: Essential Techniques for Perfect Audio
You may want to see also
Explore related products





![]()
Semilunar Valves: Closure of aortic/pulmonic valves produces second heart sound (S2)
The second heart sound, or S2, is a critical auditory marker in cardiac auscultation, signaling the end of ventricular ejection. This sound is primarily produced by the closure of the semilunar valves—the aortic and pulmonic valves. As blood is forcefully ejected from the ventricles during systole, these valves open to allow blood flow into the aorta and pulmonary artery, respectively. Once the pressure in the ventricles drops below that in the arteries, the semilunar valves snap shut, creating the distinct "dub" component of the heartbeat. This closure prevents backflow into the ventricles, ensuring unidirectional blood flow.
To understand the mechanics, consider the timing and pressure dynamics. The aortic valve closes slightly before the pulmonic valve due to the higher pressure in the systemic circulation compared to the pulmonary circulation. This slight delay results in a split second heart sound, often described as an "A2" (aortic closure) followed by a "P2" (pulmonic closure). Clinicians use this split to assess cardiac function and detect abnormalities, such as a widened split in conditions like right bundle branch block or a fixed split in atrial septal defects.
From a practical standpoint, auscultating S2 requires precise technique. Place the diaphragm of the stethoscope over the second intercostal space to the right of the sternum for the aortic component and the left sternal edge for the pulmonic component. Listen for the intensity, timing, and quality of the sound. A loud, widely split S2 may indicate pulmonary hypertension, while a paradoxically split S2 (wider during inspiration) can suggest left bundle branch block. Regular monitoring of S2 can provide early clues to valvular dysfunction or systemic issues.
For medical professionals, understanding the physiology of semilunar valve closure is essential for diagnosing cardiac conditions. For instance, a delayed or absent A2 may indicate aortic valve insufficiency, while a muffled or soft S2 could suggest semilunar valve stenosis. Patients with congenital heart defects, such as tetralogy of Fallot, often exhibit altered S2 characteristics due to anomalous valve structure or function. Incorporating this knowledge into routine assessments can enhance diagnostic accuracy and patient outcomes.
In summary, the closure of the semilunar valves is the definitive source of the second heart sound. This physiological event is not only a marker of cardiac cycle progression but also a diagnostic tool for identifying cardiovascular abnormalities. By mastering the nuances of S2, healthcare providers can better evaluate heart health and tailor interventions to individual patient needs. Whether in a clinical or educational setting, appreciating the role of semilunar valves in heart sounds is indispensable for cardiac care.
Mastering Sleep Sounds: Effective Strategies for a Quieter, Restful Night
You may want to see also
Explore related products






![]()
Blood Turbulence: Abnormal flow creates murmurs, indicating valve issues or defects
The heart's symphony, a rhythmic cadence of lub-dub, is a marvel of precision. Yet, when blood flow deviates from its smooth, laminar path, turbulence arises, manifesting as murmurs—subtle whispers or loud roars that betray underlying valve dysfunction. These abnormal sounds, detected through auscultation, serve as critical diagnostic clues, revealing the heart's hidden struggles.
Consider the mitral valve, a bicuspid structure that prevents backflow from the left ventricle to the left atrium. When stenotic or regurgitant, blood flow becomes chaotic, generating turbulence. This turbulence produces a murmur, typically heard best with the bell of a stethoscope at the apex of the heart. For instance, a low-pitched, rumbling diastolic murmur suggests mitral stenosis, often caused by rheumatic fever, while a high-pitched, blowing systolic murmur may indicate mitral regurgitation, possibly due to prolapse or ischemia.
Diagnosing these murmurs requires precision. Clinicians grade their intensity on a scale of 1 to 6, with grade 1 being faint and grade 6 audible with the stethoscope slightly off the chest. Timing is equally crucial: systolic murmurs occur during ventricular contraction, while diastolic murmurs arise during relaxation. For example, a harsh, systolic ejection murmur in a child could signal aortic stenosis, a congenital defect requiring surgical intervention. Adults, particularly those over 65, may develop murmurs due to calcified valves, a condition exacerbated by hypertension or diabetes.
Practical tips for detection include positioning the patient in the left lateral decubitus position to enhance murmur audibility and using maneuvers like handgrip or squatting to alter preload and afterload, thereby intensifying murmurs. For instance, squatting increases systemic vascular resistance, amplifying a hypertrophic cardiomyopathy-related murmur. Conversely, standing abruptly may diminish a murmur caused by aortic regurgitation.
In conclusion, blood turbulence is more than an acoustic anomaly—it’s a window into the heart’s structural integrity. Recognizing the characteristics of murmurs—their pitch, timing, and response to maneuvers—enables timely intervention, from medication management to surgical repair. By mastering the language of turbulence, clinicians can decode the heart’s silent cries for help, ensuring its rhythm endures.
Exploring the Unique Melody and Charm of an Irish Accent
You may want to see also
Explore related products






![]()
Ventricular Contraction: Generates S1 as valves shut, marking systole start
The heart's symphony begins with a powerful beat, a sound that echoes through the chambers and announces the start of a new cycle. This initial sound, known as S1, is a critical marker in cardiology, indicating the onset of systole and the heart's journey to pump oxygenated blood throughout the body. It is a sound that every medical professional learns to recognize, a fundamental aspect of auscultation.
The Mechanism Unveiled: Ventricular contraction is the maestro behind this auditory cue. As the ventricles contract, a surge of pressure builds, forcing the atrioventricular valves (tricuspid and mitral) to snap shut. This abrupt closure creates a vibration, a low-pitched 'lub' sound, which is the S1 heart sound. It's a precise moment in the cardiac cycle, occurring at the very beginning of systole, when the ventricles start to eject blood. The intensity of this sound can provide valuable insights; a soft S1 may suggest valve issues or a decrease in ventricular contractility, while a loud, palpable S1 could indicate hypertension or increased blood volume.
Clinical Significance: Auscultating S1 is a routine yet vital part of patient assessment. It allows healthcare providers to determine the heart's rhythm and identify potential abnormalities. For instance, a split S1, where the mitral and tricuspid valve closures are heard separately, can be normal in children but may indicate bundle branch block or atrial enlargement in adults. Understanding the nuances of S1 can guide further diagnostic steps, such as echocardiograms or electrocardiograms, to ensure timely interventions.
Practical Tips for Auscultation: To capture S1 effectively, place the diaphragm of the stethoscope on the chest, specifically at the mitral area (5th intercostal space, mid-clavicular line) and the tricuspid area (3rd left intercostal space, close to the sternum). Ask the patient to breathe normally, and listen for the distinct 'lub-dub' sounds. With practice, one can differentiate S1 from S2, the second heart sound, which occurs at the end of ventricular contraction. This skill is particularly useful in pediatrics, where heart sounds are higher pitched and faster, requiring a keen ear and a gentle touch.
In the intricate dance of the heart's valves and chambers, ventricular contraction takes center stage, producing a sound that is both a diagnostic tool and a reminder of the heart's relentless work. S1 is not just a sound; it's a window into the heart's health, a simple yet powerful indicator that guides medical professionals in their quest to understand and heal. This brief moment in the cardiac cycle carries a wealth of information, accessible through the art of auscultation.
Does Spray Foam Insulate Sound? Exploring Acoustic Benefits and Applications
You may want to see also
Explore related products






![]()
Ventricular Relaxation: Allows blood flow, with S2 marking systole end
The heart's symphony is a complex interplay of contractions and relaxations, each phase critical to maintaining blood flow. Ventricular relaxation, often overshadowed by the more dramatic systolic contraction, is a silent hero in this process. As the ventricles relax, they create a low-pressure environment, allowing blood to flow passively from the atria into the ventricles. This phase, known as diastole, is essential for ensuring the heart is adequately filled before the next contraction. Without proper ventricular relaxation, blood flow would be compromised, leading to reduced cardiac output and potential systemic consequences.
Consider the role of the semilunar valves in this context. As the ventricles transition from contraction to relaxation, the aortic and pulmonary valves close, producing the second heart sound (S2). This sound marks the end of systole and the beginning of diastole, serving as an auditory cue for clinicians to assess cardiac function. S2 is split into two components: the closure of the aortic valve (A2) followed by the pulmonary valve (P2). The timing and intensity of these components provide valuable insights into ventricular performance and valve integrity. For instance, a widened split between A2 and P2 can indicate delayed pulmonary valve closure, often seen in conditions like right bundle branch block.
Clinically, understanding ventricular relaxation is crucial for diagnosing and managing heart failure with preserved ejection fraction (HFpEF). In HFpEF, the ventricles may appear to contract normally but fail to relax adequately, impairing diastolic filling. This dysfunction can lead to elevated filling pressures, pulmonary congestion, and symptoms like shortness of breath. Diagnostic tools such as echocardiography, which measures diastolic parameters like E/A ratio and e’ velocity, are essential for identifying impaired relaxation. Treatment strategies often focus on optimizing preload, controlling blood pressure, and using medications like angiotensin receptor neprilysin inhibitors (e.g., sacubitril/valsartan) to improve diastolic function.
From a practical standpoint, optimizing ventricular relaxation involves lifestyle modifications and targeted interventions. Patients are advised to maintain a low-sodium diet to reduce fluid retention, engage in regular aerobic exercise to enhance myocardial compliance, and manage comorbidities like hypertension and diabetes. For older adults, particularly those over 65, age-related stiffening of the ventricles can exacerbate diastolic dysfunction, making early intervention critical. Monitoring S2 during auscultation remains a simple yet powerful tool for detecting abnormalities in ventricular relaxation, underscoring the importance of this often-overlooked phase in cardiac physiology.
In summary, ventricular relaxation is a cornerstone of cardiac function, enabling efficient blood flow and setting the stage for the next systolic contraction. The second heart sound (S2) serves as a vital marker of this transition, offering clinicians a window into ventricular health. By recognizing the significance of this phase and utilizing appropriate diagnostic and therapeutic strategies, healthcare providers can address diastolic dysfunction effectively, improving outcomes for patients with conditions like HFpEF. This nuanced understanding of the heart’s rhythm highlights the elegance and complexity of its design.
Decoding the Audible Fury: What Does Angriness Sound Like?
You may want to see also
Frequently asked questions
Heart sounds are primarily created by the movement of the heart valves and the resulting flow of blood.
The first heart sound (S1) is produced by the closure of the mitral and tricuspid valves, while the second heart sound (S2) is caused by the closure of the aortic and pulmonary valves.
Turbulent blood flow during valve closure and the sudden stopping of blood when valves shut create vibrations, which we hear as heart sounds.
Yes, abnormal heart sounds (murmurs) can arise from issues like septal defects, damaged valves, or turbulent flow through narrowed vessels, though the valves are the primary source of normal heart sounds.