Systole, the phase of the cardiac cycle when the heart contracts and pumps blood, is accompanied by distinct sounds that are crucial for clinical assessment. The primary sound associated with systole is the first heart sound, often described as a low-pitched lub, which occurs when the atrioventricular valves (mitral and tricuspid) close, marking the beginning of ventricular contraction. In certain conditions, such as aortic stenosis or hypertrophic cardiomyopathy, an additional sound known as an ejection click or a fourth heart sound (S4) may be audible during late systole, indicating abnormal turbulence or ventricular stiffness. Understanding these systolic sounds is essential for diagnosing cardiovascular disorders and evaluating heart function.
Explore related products






What You'll Learn
- Heart Valve Sounds: Understanding the role of aortic and mitral valves in systolic sounds
- Murmurs in Systole: Identifying abnormal blood flow noises during ventricular contraction
- Ejection Clicks: Recognizing sharp, high-pitched sounds linked to valve abnormalities
- Systolic Gallop (S3): Detecting the extra heart sound in early diastole
- Innocent Systolic Noises: Differentiating benign sounds from pathological systolic murmurs
![]()
Heart Valve Sounds: Understanding the role of aortic and mitral valves in systolic sounds
The systolic phase of the cardiac cycle is a symphony of sounds, each with a distinct role in diagnosing heart health. Among these, the aortic and mitral valves are the primary conductors, producing audible cues that clinicians rely on to assess cardiac function. The first heart sound (S1) marks the beginning of systole, characterized by the closure of the mitral and tricuspid valves. However, it’s the aortic valve’s performance during this phase that often takes center stage. As the left ventricle contracts, blood is ejected into the aorta, and the aortic valve snaps shut, generating a high-pitched, crisp sound. This sound is typically described as a "lub" and is best heard at the right second intercostal space, where the aortic valve is closest to the chest wall.
In contrast, the mitral valve’s role in systolic sounds is more nuanced. While its closure contributes to S1, abnormalities in its function can produce additional systolic murmurs. For instance, mitral regurgitation, where blood flows backward into the left atrium, creates a holosystolic murmur that radiates to the apex. This murmur is harsh, pansystolic, and often accompanied by a thrill, indicating the severity of the regurgitation. Clinicians use the timing, pitch, and location of these sounds to differentiate between aortic and mitral valve pathologies. For example, an aortic stenosis murmur is late-peaking, crescendo-decrescendo, and heard best at the right second intercostal space, while mitral regurgitation is holosystolic and apical.
To effectively interpret these sounds, auscultation technique is critical. Use a diaphragm for high-pitched aortic sounds and a bell for lower-pitched mitral murmurs. Position the patient in the left lateral decubitus position to enhance sound transmission. For pediatric patients, systolic murmurs may indicate congenital defects like ventricular septal defects or patent ductus arteriosus, requiring age-specific diagnostic approaches. In adults, systolic murmurs often signal acquired valve disease, such as rheumatic heart disease or degenerative calcification.
Practical tips for clinicians include correlating auscultatory findings with imaging studies like echocardiography for confirmation. For instance, a systolic ejection click followed by a murmur in a young patient may suggest bicuspid aortic valve disease, a common congenital anomaly. In older adults, a harsh systolic murmur in the aortic area warrants screening for aortic stenosis, especially if associated with symptoms like angina or syncope. Understanding the unique contributions of the aortic and mitral valves to systolic sounds is not just an academic exercise—it’s a clinical imperative for accurate diagnosis and timely intervention.
Finally, while auscultation remains a cornerstone of cardiac evaluation, it’s essential to recognize its limitations. Systolic sounds can be subtle or masked by background noise, particularly in obese patients or those with lung disease. In such cases, advanced tools like Doppler ultrasound or cardiac MRI may be necessary. However, mastering the art of auscultation ensures that clinicians can detect early signs of valve dysfunction, potentially preventing progression to heart failure or other complications. By focusing on the aortic and mitral valves’ roles in systolic sounds, healthcare providers can refine their diagnostic skills and improve patient outcomes.
Glass Sound Absorption: Understanding Its Acoustic Properties and Impact
You may want to see also
Explore related products






![]()
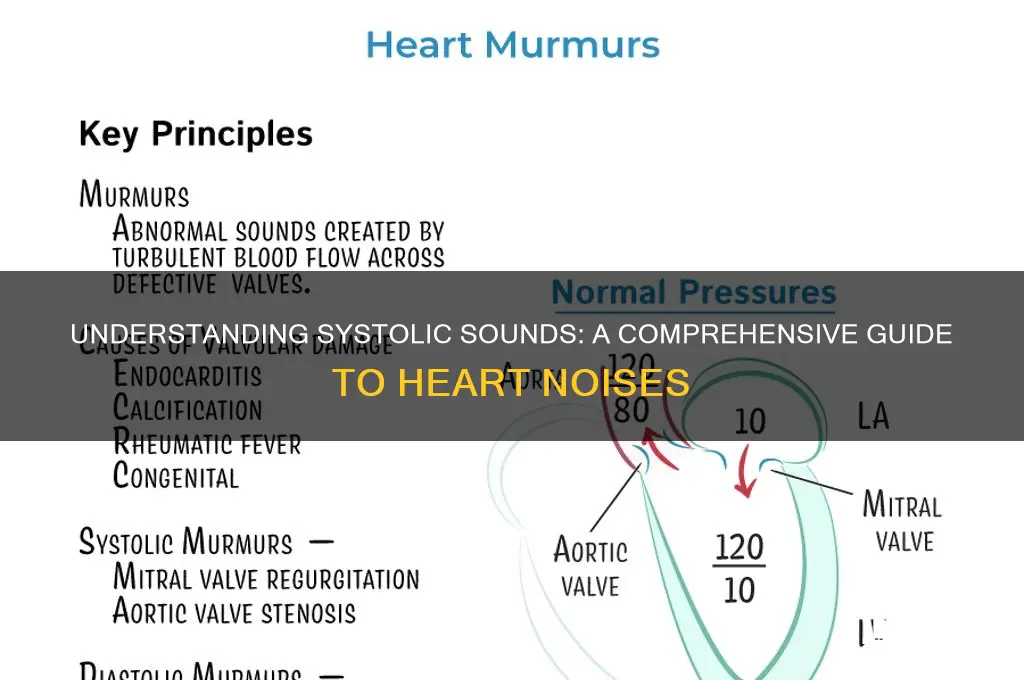
Murmurs in Systole: Identifying abnormal blood flow noises during ventricular contraction
Systolic murmurs are abnormal sounds heard during the contraction phase of the heart, specifically when the ventricles are pumping blood. These murmurs arise from turbulent blood flow, often due to structural abnormalities like valve defects or septal defects. Identifying them requires a systematic approach, combining auscultation skills with an understanding of their characteristics.
Locating the Murmur: Begin by placing the stethoscope over the four heart valve areas: aortic (right second intercostal space), pulmonic (left second intercostal space), mitral (cardiac apex), and tricuspid (left lower sternal border). Systolic murmurs are typically loudest at the site of the affected valve. For instance, a hypertrophic cardiomyopathy-related murmur is best heard at the apex with the patient in the left lateral position.
Characterizing the Sound: Systolic murmurs vary in timing, intensity, pitch, and quality. Use the Levine grading scale (1-6) to quantify loudness, where grade 3 is audible but soft, and grade 6 is heard with the stethoscope slightly off the chest. A harsh, crescendo-decrescendo murmur in mid-systole often indicates aortic stenosis, while a high-pitched, holosystolic murmur may suggest mitral regurgitation.
Clinical Context Matters: Age and comorbidities influence interpretation. For example, innocent systolic murmurs in children are common and benign, often described as "flow murmurs" without associated symptoms. In contrast, a new systolic murmur in an elderly patient with chest pain warrants urgent evaluation for conditions like acute aortic dissection or severe valvular disease.
Diagnostic Next Steps: If a systolic murmur is detected, confirm its presence in multiple positions (supine, sitting, standing) and during maneuvers like the Valsalva or squatting. Echocardiography is the gold standard for visualizing structural abnormalities, while Doppler studies quantify flow velocity and pressure gradients. For instance, a mean gradient >40 mmHg in aortic stenosis indicates severe disease, often requiring valve replacement.
Practical Tips for Clinicians: Always correlate murmur findings with symptoms and physical exam clues. For example, a systolic thrill (palpable murmur) suggests high-velocity flow, as seen in severe aortic stenosis. Teach patients to monitor for red flag symptoms like syncope, angina, or dyspnea, which may indicate progression of underlying pathology. Early referral to a cardiologist is critical for conditions like infective endocarditis, where prompt antibiotic therapy is lifesaving.
Breaking the Sound Barrier: Discovering What's Faster Than Sound
You may want to see also
Explore related products






![]()
Ejection Clicks: Recognizing sharp, high-pitched sounds linked to valve abnormalities
Systolic murmurs and sounds are a cardiologist's window into the heart's function, but among these, ejection clicks stand out as distinct markers of specific valve abnormalities. These sharp, high-pitched sounds occur early in systole and are often associated with conditions like pulmonary stenosis or aortic stenosis, where the valve leaflets are thickened or fused. Recognizing an ejection click is crucial, as it can differentiate between benign and pathologic conditions, guiding further diagnostic steps and treatment plans.
To identify an ejection click, auscultate carefully over the relevant valve area—the second left intercostal space for aortic stenosis or the second right intercostal space for pulmonary stenosis. The sound is brief, resembling a "click," and is immediately followed by a crescendo-decrescendo murmur. In pulmonary stenosis, for instance, the click is best heard with the patient in full inspiration, as this maneuver increases blood flow velocity across the valve, making the sound more pronounced. Practicing with a stethoscope on patients with known valve abnormalities can refine your ability to detect these subtle sounds.
Ejection clicks are not always pathologic; they can occasionally be heard in young, healthy individuals, particularly children and adolescents, due to rapid ventricular ejection. However, in older patients or those with symptoms like chest pain, syncope, or shortness of breath, an ejection click is a red flag. For example, in a 60-year-old with exertional dyspnea, an ejection click followed by a harsh systolic murmur strongly suggests significant aortic stenosis, warranting urgent echocardiography to assess valve morphology and gradient severity.
When teaching medical students or trainees, emphasize the importance of context in interpreting ejection clicks. A 10-year-old with a click and no symptoms likely has a benign finding, whereas a 70-year-old with the same sound may require valve replacement. Pair auscultation with imaging studies like Doppler echocardiography to correlate the click with hemodynamic data, such as a peak gradient of 40 mmHg in pulmonary stenosis or a mean gradient of 40 mmHg in aortic stenosis, which indicate severe disease. This multimodal approach ensures accurate diagnosis and appropriate management.
In summary, ejection clicks are sharp, high-pitched systolic sounds that signal valve abnormalities, particularly in the aortic or pulmonary valves. Mastery of auscultation techniques, understanding patient demographics, and integrating imaging data are essential for distinguishing benign from pathologic clicks. By recognizing these sounds, clinicians can initiate timely interventions, improving outcomes for patients with valve disease.
Unveiling Lincoln's Voice: Reconstructing the President's Authentic Speech Patterns
You may want to see also
Explore related products






![]()
Systolic Gallop (S3): Detecting the extra heart sound in early diastole
The systolic gallop, often referred to as S3, is a subtle yet significant finding in cardiac auscultation. Unlike the typical lub-dub of a healthy heart, S3 introduces an extra sound in early diastole, creating a rhythmic pattern akin to a galloping horse. This sound is best heard with the bell of the stethoscope at the apex of the heart, during expiration, and in the left lateral decubitus position. While it can be a normal finding in children and well-trained athletes, its presence in adults often signals underlying pathology, such as heart failure, myocardial ischemia, or valvular disease. Recognizing S3 requires a keen ear and an understanding of its clinical implications.
To detect S3 effectively, follow these steps: position the patient in the left lateral decubitus position, ask them to exhale slowly, and place the bell of the stethoscope at the cardiac apex. Listen carefully for a low-pitched, brief sound occurring 0.12 to 0.18 seconds after the S2 component. Differentiating S3 from other murmurs or split sounds is crucial; S3 is distinct in its timing and quality. For instance, a mitral regurgitation murmur occurs in systole, while S3 is diastolic. If S3 is suspected, further diagnostic tests, such as echocardiography, may be warranted to assess ventricular function and identify the underlying cause.
From a comparative perspective, S3 stands apart from other gallop rhythms, such as S4, which is also a diastolic sound but occurs later in the cycle and is often associated with stiffer ventricles. While S4 is typically pathologic, S3 can be benign in certain populations but is more frequently a marker of cardiac stress. For example, in heart failure, S3 reflects increased ventricular filling pressures and reduced compliance. Understanding these distinctions is essential for accurate diagnosis and management. Clinicians should remain vigilant, as overlooking S3 could delay intervention in high-risk patients.
Persuasively, the detection of S3 should not be dismissed as a mere auscultatory curiosity. Its presence often correlates with advanced heart failure stages, where early intervention can significantly alter outcomes. For instance, in patients with reduced ejection fraction, the identification of S3 may prompt aggressive titration of guideline-directed medical therapy, including angiotensin-converting enzyme inhibitors, beta-blockers, and mineralocorticoid receptor antagonists. Practical tips include using electronic stethoscopes or recording devices to amplify and analyze sounds, especially in challenging cases. By mastering the art of detecting S3, clinicians can enhance their diagnostic acumen and improve patient care.
Descriptively, the S3 sound is often likened to the "lub-la-dub" of a galloping horse, with the "la" representing the extra vibration. This metaphorical description aids in memorization and recognition. In practice, the sound is soft and low-pitched, requiring a quiet environment and focused listening. Patients with S3 may be asymptomatic or present with nonspecific symptoms like fatigue or dyspnea, making auscultation a critical tool in uncovering hidden pathology. For medical students and trainees, practicing on diverse patient populations and using online auscultation libraries can build confidence in identifying this elusive sound. Ultimately, the systolic gallop is a testament to the richness of cardiac auscultation and its enduring relevance in modern medicine.
Can Loud Noises Aggravate Tinnitus? Understanding Sound's Impact on Ringing Ears
You may want to see also
Explore related products





![]()
Innocent Systolic Noises: Differentiating benign sounds from pathological systolic murmurs
Systolic murmurs, often detected during cardiac auscultation, can be a source of anxiety for both patients and clinicians. However, not all systolic sounds signify pathology. Innocent systolic murmurs, also known as functional or physiologic murmurs, are benign flow sounds that occur in the absence of structural heart disease. Differentiating these from pathological murmurs is crucial to avoid unnecessary investigations and alleviate patient concern.
Understanding the Characteristics
Innocent systolic noises typically present as soft (grade I-II/VI) and are best heard at the left upper sternal border or along the sternum. They often have a musical or vibratory quality, lacking the harshness associated with pathological murmurs. These sounds are usually short, lasting less than the entire systolic phase, and do not radiate to other areas. They are commonly observed in children, pregnant women, and young adults, particularly during periods of increased blood flow, such as fever, anemia, or hyperthyroidism. For instance, a still murmur in a child with a respiratory infection is often innocent, resolving as the underlying condition improves.
Key Differentiating Features
Pathological systolic murmurs, in contrast, are louder (grade III/VI or higher), longer in duration, and may radiate to specific areas (e.g., aortic stenosis radiating to the carotids). They are often associated with structural abnormalities like valvular disease or septal defects. Innocent murmurs lack these features and are not accompanied by signs of heart failure, such as gallop rhythms or hepatomegaly. A practical tip for clinicians is to assess the patient’s hemodynamic stability and examine for peripheral signs like pulses or bruits, which are absent in innocent murmurs.
Clinical Approach and Cautions
When evaluating systolic sounds, consider the patient’s age, medical history, and physical exam findings. In children, innocent murmurs are common and often disappear by adolescence. In adults, particularly those over 50, a new systolic murmur warrants further investigation, such as echocardiography, to rule out pathology. Caution should be exercised in pregnant women, as innocent murmurs may coexist with physiological changes, but persistent or loud murmurs require evaluation to exclude conditions like mitral stenosis.
Practical Takeaway
Differentiating innocent systolic noises from pathological murmurs hinges on recognizing their distinct characteristics and clinical context. Soft, brief, non-radiating murmurs in otherwise healthy individuals are likely benign. However, any murmur associated with symptoms, structural abnormalities, or high-risk features demands thorough evaluation. By mastering this distinction, clinicians can provide accurate diagnoses, avoid over-investigation, and ensure appropriate patient management.
What Does Elgato Sound Do? Exploring Its Features and Benefits
You may want to see also
Frequently asked questions
Systole is the phase of the cardiac cycle when the heart muscle contracts and pumps blood out of the ventricles. The primary sound heard during systole is the first heart sound (S1), often described as a "lub" sound, which occurs when the atrioventricular valves (mitral and tricuspid) close.
Yes, abnormal sounds during systole can include ejection clicks, which are high-pitched sounds associated with conditions like aortic stenosis or pulmonic stenosis. Additionally, a systolic murmur may be heard, indicating turbulent blood flow during ventricular contraction, often due to valve abnormalities or defects.
No, the third (S3) and fourth (S4) heart sounds are associated with diastole, the relaxation phase of the heart. S3 is sometimes called a "ventricular gallop," while S4 is often referred to as an "atrial gallop." Neither occurs during systole.