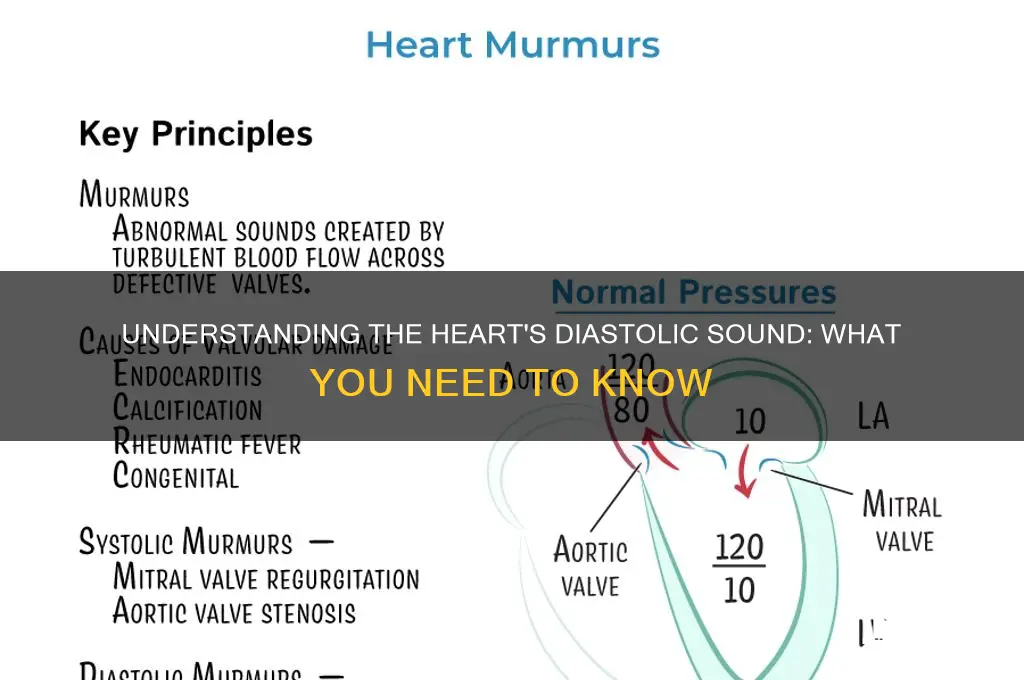
Diastole, the phase of the cardiac cycle when the heart muscle relaxes and the chambers fill with blood, is often associated with a distinct sound that can be heard through a stethoscope. This sound, known as the diastolic murmur, occurs when turbulent blood flow passes through the heart valves or blood vessels during this relaxation phase. Unlike the prominent lub-dub sounds of systole, which are caused by the closing of the heart valves, diastolic sounds are typically softer and may indicate underlying conditions such as valve regurgitation, stenosis, or abnormalities in blood flow. Understanding these sounds is crucial for diagnosing cardiovascular issues, as they provide valuable insights into the heart's function during its resting phase.
| Characteristics | Values |
|---|---|
| Sound Type | Murmurs, specifically diastolic murmurs |
| Timing | Occurs during the diastolic phase of the cardiac cycle (when the heart relaxes and fills with blood) |
| Causes | Associated with abnormalities in heart valves (e.g., aortic regurgitation, mitral stenosis) or structural issues |
| Pitch | Typically low-pitched, rumbling, or blowing in nature |
| Duration | Can be short (early diastolic) or prolonged (mid to late diastolic) |
| Location | Best heard at specific auscultation sites depending on the underlying cause (e.g., aortic area for aortic regurgitation, apical area for mitral stenosis) |
| Intensity | May range from soft to loud, depending on the severity of the condition |
| Associated Symptoms | Fatigue, shortness of breath, chest pain, or palpitations, depending on the cause |
| Diagnostic Tools | Confirmed via auscultation, echocardiography, or other imaging studies |
| Treatment | Depends on the underlying cause (e.g., valve repair/replacement, medication, lifestyle changes) |
Explore related products





What You'll Learn
- Heart Valve Function: Normal vs. abnormal sounds linked to valve opening during diastole
- Mitral Valve Prolapse: Clicking sound caused by valve leaflet displacement during diastolic phase
- Aortic Regurgitation: Murmurs heard in diastole due to blood backflow into the aorta
- Third Heart Sound (S3): Low-pitched ventricular gallop occurring in early diastole
- Pericardial Friction Rub: Triphasic, grating sound sometimes audible during diastole in pericarditis
![]()
Heart Valve Function: Normal vs. abnormal sounds linked to valve opening during diastole
During diastole, the heart’s mitral valve opens to allow blood to flow from the left atrium into the left ventricle. This process is typically silent in a healthy heart, as the valve leaflets move smoothly without obstruction. However, when abnormalities occur, distinct sounds can emerge, signaling potential issues. For instance, a clicking sound before the first heart sound (S1) may indicate mitral valve prolapse, where the valve leaflets bulge back into the atrium. Understanding these nuances is crucial for early detection and intervention in valve dysfunction.
Abnormal sounds during diastole often arise from pathological conditions affecting valve function. Mitral stenosis, for example, can produce a rumbling, low-pitched diastolic murmur heard best at the apex of the heart. This occurs when the mitral valve narrows, restricting blood flow and creating turbulence. In contrast, aortic regurgitation may cause a high-pitched, decrescendo diastolic murmur, as blood flows backward from the aorta into the left ventricle. These sounds are diagnostic clues that guide clinicians in identifying specific valve disorders.
To differentiate normal from abnormal diastolic sounds, auscultation technique is key. Positioning the stethoscope at the appropriate anatomical landmarks—such as the apex for mitral sounds or the third left intercostal space for aortic sounds—enhances detection. Patients with abnormal diastolic murmurs may also report symptoms like fatigue, shortness of breath, or palpitations, which should prompt further evaluation. Echocardiography remains the gold standard for confirming valve pathology, providing visual and quantitative data to complement auditory findings.
Practical tips for healthcare providers include correlating auscultation findings with patient history and risk factors. For instance, a history of rheumatic fever increases the likelihood of mitral stenosis, while hypertension is a common risk factor for aortic regurgitation. Educating patients about the significance of new or changing heart sounds empowers them to seek timely medical attention. Early recognition of abnormal diastolic sounds can lead to interventions such as valve repair, replacement, or medication management, improving long-term outcomes for patients with valve dysfunction.
Exploring the Unique Sonic Signatures of Musical Instruments
You may want to see also
Explore related products






![]()
Mitral Valve Prolapse: Clicking sound caused by valve leaflet displacement during diastolic phase
During the diastolic phase of the cardiac cycle, when the heart relaxes and fills with blood, a distinct clicking sound can signal mitral valve prolapse (MVP). This occurs when one or both leaflets of the mitral valve bulge backward into the left atrium, causing a momentary displacement. Unlike the lub-dub of normal heart sounds, this click is high-pitched and brief, often followed by a late systolic murmur if blood leaks back into the atrium. Clinicians identify this sound through auscultation, typically using a stethoscope placed over the apex of the heart, best heard in the left lateral decubitus position.
To diagnose MVP, healthcare providers follow a systematic approach. First, they assess the patient’s medical history for symptoms like palpitations, fatigue, or chest discomfort. Next, they perform a physical exam, focusing on the timing and quality of the click. Confirmatory tests, such as echocardiography, provide visual evidence of leaflet displacement and assess valve function. For adults, especially those over 50, MVP is often benign and requires no treatment unless complications arise. However, younger patients or those with severe prolapse may need monitoring or medication to manage associated arrhythmias or mitral regurgitation.
The clicking sound in MVP is not just a diagnostic marker but also a reminder of the heart’s intricate mechanics. During diastole, the mitral valve should remain closed, ensuring blood flows efficiently from the left atrium to the ventricle. In MVP, the leaflets’ abnormal movement disrupts this process, creating turbulence and the characteristic click. This sound is more pronounced during expiration and in the standing position, as these conditions reduce intrathoracic pressure, accentuating leaflet displacement. Understanding this physiology helps clinicians differentiate MVP from other diastolic murmurs, such as those caused by aortic regurgitation.
For patients living with MVP, practical management strategies can alleviate symptoms and reduce anxiety. Avoiding stimulants like caffeine and decongestants can minimize palpitations, while beta-blockers or antiarrhythmics may be prescribed for persistent symptoms. Regular exercise, tailored to individual tolerance, strengthens the heart without overloading the valve. Patients should also practice stress-reduction techniques, as anxiety can exacerbate symptoms. Annual or biennial follow-ups with a cardiologist ensure early detection of complications, such as endocarditis, which requires antibiotic prophylaxis before certain dental or surgical procedures.
In summary, the diastolic click of mitral valve prolapse is a unique auditory clue to valve dysfunction, arising from leaflet displacement during the heart’s relaxation phase. Recognizing this sound, understanding its mechanism, and implementing targeted management strategies empower both clinicians and patients to address MVP effectively. While often benign, MVP underscores the importance of precise diagnosis and proactive care to maintain cardiovascular health.
Mastering Sales Speak: Essential Tips to Sound Confident and Savvy
You may want to see also
Explore related products

$29.59 $36.99





![]()
Aortic Regurgitation: Murmurs heard in diastole due to blood backflow into the aorta
During diastole, when the heart relaxes and the aortic valve should remain closed, a distinct murmur can signal aortic regurgitation. This occurs when blood flows backward from the aorta into the left ventricle due to a malfunctioning valve. Unlike systolic murmurs, which coincide with the heart’s contraction, diastolic murmurs in aortic regurgitation are a late-decrescendo sound, often described as high-pitched and blowing. Clinicians typically hear this murmur best at the left sternal border with the patient in the sitting position and leaning forward, using the diaphragm of the stethoscope.
To diagnose aortic regurgitation, it’s crucial to differentiate this murmur from others. For instance, a diastolic murmur in mitral stenosis is low-pitched and rumbling, whereas aortic regurgitation produces a higher-pitched sound. Severity is assessed by duration and intensity: a softer, shorter murmur may indicate mild regurgitation, while a louder, longer one suggests severe backflow. Echocardiography is often used to confirm the diagnosis, measuring the regurgitant volume and left ventricular size, which are key indicators of disease progression.
Patients with aortic regurgitation may remain asymptomatic for years, but symptoms like fatigue, shortness of breath, or chest pain eventually arise, particularly in chronic cases. Management depends on severity. Mild to moderate regurgitation often requires monitoring with annual echocardiograms and blood pressure control (targeting a systolic pressure <120 mmHg) to reduce left ventricular stress. Severe cases, especially with symptoms or left ventricular dilation (end-systolic diameter >50 mm), may necessitate surgical intervention, such as valve repair or replacement.
For those at risk—including individuals with a bicuspid aortic valve, syphilis, or hypertension—early detection is vital. Regular cardiac evaluations, including auscultation and imaging, can prevent complications like heart failure. Lifestyle modifications, such as maintaining a healthy weight and avoiding strenuous lifting, can also reduce strain on the valve. Understanding the diastolic murmur in aortic regurgitation is not just an academic exercise; it’s a practical tool for timely intervention and improved patient outcomes.
Understanding Sound Creation Through Modeling Synthesis Techniques and Process
You may want to see also
Explore related products






![]()
Third Heart Sound (S3): Low-pitched ventricular gallop occurring in early diastole
The third heart sound, often abbreviated as S3, is a distinct auditory phenomenon that occurs during the early phase of diastole, the period when the heart relaxes and fills with blood. Unlike the more commonly recognized first and second heart sounds (S1 and S2), which are higher-pitched and associated with the closing of heart valves, S3 is a low-pitched, brief sound often described as a ventricular gallop. This sound is typically heard best with the bell of a stethoscope placed over the cardiac apex, usually in the fifth left intercostal space, mid-clavicular line. Clinicians often liken the rhythm of S1, S2, and S3 to the cadence of the phrase "Kentucky gallop," emphasizing the additional beat that S3 introduces.
From an analytical perspective, the presence of S3 is not always pathological. In children and young adults, it can be a normal finding, reflecting a hyperdynamic circulatory state where the heart is efficiently filling with blood. However, in older adults or individuals with cardiovascular conditions, S3 often signifies impaired ventricular function. Conditions such as heart failure, myocardial infarction, or volume overload can cause the ventricle to become stiffer or less compliant, leading to increased filling pressures and the emergence of S3. Thus, while S3 in a young athlete might be benign, its detection in a 60-year-old patient with dyspnea warrants further investigation, including echocardiography to assess ejection fraction and diastolic function.
For healthcare providers, recognizing S3 requires both skill and practice. The sound is soft and brief, often lasting less than 0.1 seconds, making it easy to miss. A systematic approach to auscultation is essential: listen carefully during early diastole, ensure the patient is in a left lateral recumbent position, and use a stethoscope with both a bell and a diaphragm. If S3 is suspected, consider having the patient perform the Valsalva maneuver or lie on their left side, as these positions can accentuate the sound. Documenting the finding with precision—noting its timing, pitch, and intensity—is crucial for accurate diagnosis and communication with colleagues.
Comparatively, S3 stands apart from other diastolic sounds, such as the fourth heart sound (S4), which occurs late in diastole and is associated with atrial contraction. While S4 is often described as a high-pitched "atrial gallop," S3’s low-pitched quality and early diastolic timing are unique. This distinction is vital for differential diagnosis: S4 typically indicates stiffer ventricles and is more commonly associated with conditions like hypertension or aortic stenosis, whereas S3 is more closely linked to volume overload or systolic dysfunction. Understanding these nuances allows clinicians to tailor their diagnostic and therapeutic approaches effectively.
In practical terms, the detection of S3 should prompt a focused clinical evaluation. For patients over 50 or those with risk factors for heart disease, a comprehensive workup may include laboratory tests (e.g., BNP or troponin levels), imaging studies (e.g., echocardiogram or chest X-ray), and a detailed symptom assessment. Lifestyle modifications, such as sodium restriction and fluid management, may be recommended, alongside pharmacotherapy like diuretics or ACE inhibitors, depending on the underlying cause. Early recognition and management of S3-related conditions can significantly improve outcomes, underscoring the importance of mastering auscultation skills and understanding the clinical implications of this subtle yet significant sound.
Mastering Frog Calls: A Guide to Identifying Amphibian Sounds
You may want to see also
Explore related products






![]()
Pericardial Friction Rub: Triphasic, grating sound sometimes audible during diastole in pericarditis
A pericardial friction rub is a distinctive, high-pitched, triphasic sound that can be heard during auscultation in patients with pericarditis. This grating or scratching noise occurs as the inflamed pericardial layers rub against each other, most prominently during diastole when the heart relaxes and moves within the pericardial sac. Unlike murmurs, which are typically systolic or continuous, this rub is uniquely tied to the cardiac cycle’s phases, making it a critical diagnostic marker for acute pericarditis.
To identify a pericardial friction rub, clinicians should use a stethoscope with the patient in a seated, leaned-forward position, which maximizes the sound’s audibility. The rub is best heard along the lower left sternal border or in the precordial area. Its triphasic nature—occurring in early systole, midsystole, and early diastole—distinguishes it from other cardiac sounds. However, the diastolic component is often the most pronounced, making it a key focus during auscultation.
While the pericardial friction rub is a hallmark of acute pericarditis, its presence is not universal. Studies suggest it is audible in only 30–80% of cases, depending on the severity of inflammation and timing of auscultation. Patients with viral pericarditis, the most common cause, are more likely to exhibit this finding compared to those with uremic or neoplastic etiologies. Early detection is crucial, as untreated pericarditis can progress to complications like cardiac tamponade.
Clinicians should be cautious not to confuse a pericardial friction rub with other sounds, such as pleural friction rubs or mitral valve prolapse clicks. Pleural rubs are typically absent over the heart and do not follow the cardiac cycle, while mitral clicks are higher-pitched and confined to systole. A detailed patient history, including recent viral illnesses or trauma, can further support the diagnosis. If a rub is suspected, urgent echocardiography is recommended to assess pericardial effusion and cardiac function.
In summary, the pericardial friction rub is a triphasic, grating sound that serves as a diagnostic cornerstone for acute pericarditis, particularly during diastole. Its detection requires careful auscultation, patient positioning, and differentiation from similar sounds. While not always present, its identification prompts immediate management, including anti-inflammatory therapy and monitoring for complications. Mastery of this auscultatory skill is essential for clinicians to ensure timely and accurate diagnosis.
Understanding Sound Wall Organization: Structure, Design, and Implementation Strategies
You may want to see also
Frequently asked questions
The second heart sound (S2) occurs with diastole, often described as a "dub" sound, and is associated with the closing of the aortic and pulmonic valves.
Yes, the third heart sound (S3), also known as a ventricular gallop or "protodiastolic gallop," can occur in early diastole, though it is not always present and may indicate certain cardiac conditions.
Diastolic murmurs can occur during diastole, such as those caused by aortic regurgitation or mitral stenosis, and are characterized by abnormal blood flow sounds during this phase.
Diastole is typically associated with quieter heart sounds compared to systole, primarily featuring the second heart sound (S2) and, in some cases, a third heart sound (S3) or diastolic murmurs.