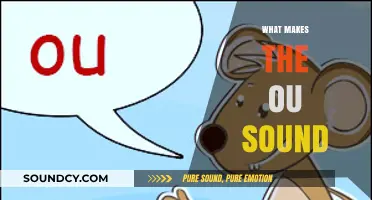
The human heartbeat is a symphony of physiological processes, orchestrated by the rhythmic contraction and relaxation of the heart muscles. This sound, often described as lub-dub, is produced by the closing of the heart valves as blood is pumped through the chambers. The first sound, or lub, occurs when the atrioventricular valves (tricuspid and mitral) close, preventing blood from flowing backward into the atria. The second sound, or dub, is generated when the semilunar valves (aortic and pulmonary) close, ensuring blood flows out of the heart into the arteries. These sounds are amplified by the resonance of blood and surrounding tissues, making them audible through a stethoscope or even by placing an ear against the chest. Understanding the mechanics behind these sounds not only highlights the heart's efficiency but also serves as a vital diagnostic tool in assessing cardiovascular health.
Explore related products






What You'll Learn
- Heart Valves Function: Valves open/close, creating lub-dub sounds as blood flows through chambers
- Blood Flow Dynamics: Turbulent or laminar flow affects sound intensity and quality
- Heart Rate Impact: Faster rates shorten sounds; slower rates prolong them
- Cardiac Muscle Contraction: Atrial and ventricular contractions produce distinct sound phases
- Abnormal Sounds (Murmurs): Irregular blood flow causes whooshing or extra sounds
![]()
Heart Valves Function: Valves open/close, creating lub-dub sounds as blood flows through chambers
The rhythmic lub-dub of the heartbeat is a symphony orchestrated by the heart’s four valves: the tricuspid, pulmonary, mitral, and aortic. Each sound corresponds to the precise opening and closing of these valves as blood flows through the heart’s chambers. The "lub" occurs when the mitral and tricuspid valves close, preventing blood from flowing backward into the atria. The "dub" follows as the aortic and pulmonary valves shut, ensuring blood moves forward into the arteries. This mechanical process is essential for maintaining unidirectional blood flow, a cornerstone of cardiovascular health.
To visualize this, imagine a one-way street system. The valves act as gates, opening to allow traffic (blood) to pass and closing to prevent backflow. For instance, when the ventricles contract, the aortic and pulmonary valves open, permitting oxygen-rich blood to exit the heart. If these valves malfunction—say, due to stenosis (narrowing) or regurgitation (leakage)—the lub-dub rhythm becomes irregular, potentially leading to murmurs or other audible anomalies. Regular cardiac check-ups, especially for individuals over 50 or those with a family history of heart disease, can detect such issues early.
From a practical standpoint, understanding valve function can guide lifestyle choices. High blood pressure, for example, forces the heart to work harder, straining the valves over time. Maintaining a blood pressure below 120/80 mmHg through diet, exercise, and medication (if prescribed) can reduce this strain. Similarly, avoiding smoking and limiting alcohol intake protects valve integrity. For those with known valve issues, anticoagulants like warfarin (5–10 mg daily, adjusted by INR levels) may be recommended to prevent clot formation, a common complication of valve dysfunction.
Comparatively, the heart’s valves are akin to the doors in a well-designed house. Just as doors control the flow of people, valves regulate blood flow. However, unlike doors, valves operate autonomically, requiring no conscious effort. This seamless function is a marvel of biology, yet it’s vulnerable to wear and tear. Conditions like rheumatic fever or age-related calcification can damage valves, underscoring the importance of preventive care. Annual echocardiograms for at-risk individuals can monitor valve health, ensuring timely intervention if abnormalities arise.
In conclusion, the lub-dub sounds are more than just auditory cues—they’re indicators of valve efficiency. By understanding this mechanism, individuals can take proactive steps to preserve heart health. Whether through lifestyle modifications, medication adherence, or regular screenings, safeguarding valve function is key to a steady, rhythmic heartbeat. After all, the heart’s symphony is one worth preserving.
When Do Kids Master the S Sound? A Developmental Guide
You may want to see also
Explore related products





![]()
Blood Flow Dynamics: Turbulent or laminar flow affects sound intensity and quality
The heart's rhythmic sounds are not merely a beat but a symphony of fluid dynamics. Blood flow through the heart and vessels can be either laminar, where blood moves in smooth, parallel layers, or turbulent, characterized by chaotic, irregular patterns. This distinction is critical because it directly influences the intensity and quality of the sounds produced. Laminar flow, typical in healthy, unobstructed vessels, generates minimal noise, while turbulent flow, often a sign of obstructions or abnormalities, creates distinct, audible disturbances. Understanding this relationship is key to diagnosing cardiovascular issues through auscultation.
Consider the analogy of water flowing through a pipe. When the pipe is smooth and wide, water flows quietly and efficiently—akin to laminar blood flow in a healthy artery. However, if the pipe narrows or becomes rough, the water churns and gurgles, producing noise. Similarly, turbulent blood flow occurs when blood encounters obstacles like valve stenosis, atherosclerotic plaques, or sudden changes in vessel diameter. This turbulence amplifies sound intensity, often manifesting as murmurs or bruits during auscultation. For instance, a turbulent flow across a stenotic aortic valve produces a harsh, crescendo-decrescendo murmur, distinct from the softer, benign sounds of laminar flow.
Clinicians can leverage this knowledge to differentiate pathological from physiological sounds. For example, a turbulent flow in children with innocent heart murmurs often resolves as the heart grows, while persistent turbulence in adults may indicate valve disease. Practical tips for auscultation include using a stethoscope with high acoustic sensitivity, focusing on specific heart valves, and noting the timing, pitch, and duration of sounds. For instance, a systolic murmur heard best at the left sternal border suggests turbulent flow across the pulmonary valve, whereas a diastolic murmur at the apex points to mitral valve issues.
To quantify these dynamics, the Reynolds number (Re) is a useful metric, calculated as Re = (density × velocity × diameter) / viscosity. Laminar flow typically occurs at Re < 2000, while turbulent flow begins at Re > 3000. In clinical practice, while direct measurement of Re is impractical, understanding this threshold helps interpret auscultation findings. For instance, increased blood velocity due to hypertension or anemia can elevate Re, promoting turbulence and louder murmurs. Managing these conditions—such as controlling blood pressure or addressing anemia—can reduce turbulence and improve sound quality.
In conclusion, the interplay between turbulent and laminar flow is a cornerstone of cardiac auscultation. By recognizing how flow dynamics influence sound intensity and quality, healthcare providers can better diagnose and manage cardiovascular conditions. Whether in a pediatric clinic or an adult cardiology ward, this knowledge transforms the stethoscope into a powerful tool for deciphering the heart's acoustic narrative.
Unveiling Bulbasaur's Unique Vocalizations: What Does This Pokémon Sound Like?
You may want to see also
Explore related products





![]()
Heart Rate Impact: Faster rates shorten sounds; slower rates prolong them
The rhythm of the heart is a symphony of sounds, each beat a testament to the intricate dance of valves and chambers. Among the factors influencing this auditory signature, heart rate stands out as a key conductor. A faster heart rate compresses the time between beats, resulting in shorter, more abrupt sounds. Conversely, a slower rate allows each phase of the cardiac cycle to elongate, producing prolonged, drawn-out tones. This phenomenon is not merely a curiosity but a critical diagnostic tool, offering insights into cardiovascular health and physiological states.
Consider the practical implications for healthcare professionals. During auscultation, a rapid heart rate may manifest as a staccato sequence of lub-dub sounds, making it challenging to discern subtle abnormalities. For instance, tachycardia (heart rate >100 bpm) often shortens the duration of S1 and S2 heart sounds, potentially masking murmurs or valve dysfunctions. In contrast, bradycardia (heart rate <60 bpm) stretches these sounds, providing a clearer window into the heart’s mechanics. Clinicians must account for this rate-dependent acoustic shift when interpreting findings, especially in patients with conditions like atrial fibrillation or heart block.
For individuals monitoring their own heart health, understanding this relationship can empower proactive self-care. Wearable devices often report heart rate alongside sound-based metrics, but users rarely connect the two. For example, a sudden increase in heart rate during exercise may correlate with shorter heart sounds, while meditation-induced slowing may yield longer, more relaxed tones. Tracking these changes over time can reveal patterns indicative of stress, fitness gains, or underlying issues. Practical tip: Pair heart rate data with audio recordings (using apps like Heart Sounds) to observe how your cardiac rhythm evolves under different conditions.
A comparative analysis highlights the evolutionary advantage of this mechanism. In high-stress scenarios, such as fight-or-flight responses, a faster heart rate and abbreviated sounds optimize blood circulation efficiency, prioritizing survival over acoustic clarity. Conversely, during rest or recovery, slower rates and prolonged sounds reflect a state of metabolic conservation and repair. This duality underscores the heart’s adaptability, where form follows function—even in the realm of sound production.
Finally, technological advancements are leveraging this principle to enhance diagnostics. AI algorithms now analyze heart sound duration alongside rate variability to predict conditions like heart failure or arrhythmias with greater precision. For instance, a study in the *Journal of the American College of Cardiology* demonstrated that combining heart rate data with sound duration metrics improved detection accuracy by 25%. As these tools become more accessible, both clinicians and patients can harness the subtle interplay between rate and sound to safeguard cardiac well-being.
Factors Influencing Speed of Sound
You may want to see also
Explore related products






![]()
Cardiac Muscle Contraction: Atrial and ventricular contractions produce distinct sound phases
The heart's rhythmic symphony is a result of the intricate dance of cardiac muscle contractions, each movement contributing to the familiar 'lub-dub' sound. This auditory signature is not a random occurrence but a precise sequence of events, where atrial and ventricular contractions play distinct roles. Understanding these phases is crucial for deciphering the language of the heart.
The Atrial Contraction Phase: Imagine a well-choreographed ballet, where the atria, the heart's upper chambers, initiate the performance. As they contract, blood is propelled into the ventricles, creating the first sound, often described as 'lub'. This phase is swift, lasting approximately 0.1 seconds in a healthy adult heart. The intensity of this sound can vary; for instance, in children, it may be softer due to the smaller size of their hearts, while in athletes, the force of contraction might produce a more pronounced 'lub'.
Ventricular Contraction's Impact: The subsequent 'dub' sound is a powerful statement made by the ventricles. When these lower chambers contract, they generate a pressure wave, forcing the semilunar valves (aortic and pulmonary) to close. This action prevents blood from flowing backward, ensuring a unidirectional flow. The duration of this phase is slightly longer, around 0.3 seconds, allowing for a more sustained sound. Interestingly, the pitch of the 'dub' can provide insights into blood pressure; a higher-pitched sound may indicate increased pressure, while a lower pitch could suggest the opposite.
A Delicate Balance: The timing and coordination between these contractions are critical. A healthy heart ensures that the atria and ventricles work in harmony, with a brief delay between their contractions. This delay is essential, allowing the ventricles to fill adequately before pumping blood to the body. For instance, in a resting adult, the heart rate is typically 60-100 beats per minute, providing a consistent rhythm. However, during exercise, the rate can increase to 140-160 beats per minute, requiring precise coordination to maintain efficient blood circulation.
Clinical Implications: Recognizing these distinct sound phases is not merely an academic exercise. It forms the basis of auscultation, a vital diagnostic tool in cardiology. By listening to these sounds, healthcare professionals can identify abnormalities. For example, a splitting of the second heart sound (S2) may indicate a delay in aortic valve closure, potentially signaling a cardiac issue. Moreover, the intensity and quality of these sounds can guide treatment decisions, such as adjusting medication dosages or recommending lifestyle changes to optimize heart function.
In essence, the heart's sounds are a window into its mechanical operations, where each contraction phase contributes to a unique auditory signature. This knowledge empowers medical professionals to diagnose and treat cardiac conditions effectively, ensuring the heart's symphony continues to play harmoniously.
The Science Behind Bell Sounds: How Vibrations Create Ringing Tones
You may want to see also
Explore related products






![]()
Abnormal Sounds (Murmurs): Irregular blood flow causes whooshing or extra sounds
The human heart, a marvel of biological engineering, produces a symphony of sounds that can reveal much about its health. Among these, murmurs stand out as abnormal sounds caused by irregular blood flow, often manifesting as whooshing or extra noises between the characteristic "lub-dub" beats. These sounds are not part of the normal cardiac cycle and can be indicative of underlying issues, ranging from benign conditions to serious cardiovascular problems. Understanding murmurs is crucial for early detection and intervention, as they can be the first audible clue of heart valve dysfunction, congenital defects, or other structural abnormalities.
To identify a murmur, healthcare providers use a stethoscope to listen carefully during a physical examination. Murmurs are classified based on their timing (systolic or diastolic), intensity (graded on a scale of 1 to 6), location (where they are best heard), and quality (e.g., harsh, blowing, or musical). For instance, a systolic murmur occurs during the heart’s contraction phase, while a diastolic murmur happens when the heart relaxes. The intensity scale helps determine severity—a grade 1 murmur is faint and only audible in quiet conditions, whereas a grade 6 murmur is so loud it can be felt as a thrill through the stethoscope. Recognizing these characteristics is essential for differentiating benign ("innocent") murmurs from pathological ones.
Innocent murmurs, often found in children and pregnant women, are harmless and result from normal blood flow dynamics rather than structural issues. They typically resolve on their own and do not require treatment. In contrast, pathological murmurs signal problems such as valve stenosis (narrowing), regurgitation (leakage), or septal defects. For example, a harsh, systolic murmur heard at the left sternal border may indicate aortic stenosis, while a blowing, diastolic murmur at the apex could suggest mitral regurgitation. Early diagnosis through echocardiography or other imaging tests is vital to prevent complications like heart failure or arrhythmias.
Practical tips for patients include monitoring symptoms such as chest pain, shortness of breath, fatigue, or dizziness, which may accompany significant murmurs. Lifestyle modifications, such as maintaining a healthy weight, exercising regularly, and avoiding smoking, can support heart health. For those diagnosed with pathological murmurs, adherence to prescribed medications (e.g., beta-blockers or diuretics) and regular follow-ups with a cardiologist are critical. In severe cases, surgical interventions like valve repair or replacement may be necessary to restore normal blood flow and eliminate the abnormal sounds.
In conclusion, abnormal heart sounds or murmurs are more than just auditory anomalies—they are vital indicators of cardiovascular health. By understanding their causes, characteristics, and implications, both healthcare providers and patients can take proactive steps to address underlying issues. Whether benign or pathological, murmurs underscore the importance of listening closely to the heart’s unique language, ensuring timely and effective care for one of the body’s most essential organs.
How Spray Foam Insulation Reduces Noise and Echoes
You may want to see also
Frequently asked questions
The heart sounds are primarily caused by the closing of the heart valves, specifically the mitral and tricuspid valves (first sound, S1) and the aortic and pulmonary valves (second sound, S2).
The "lub" (S1) is produced by the closure of the mitral and tricuspid valves at the beginning of systole, while the "dub" (S2) is caused by the closure of the aortic and pulmonary valves at the start of diastole.
Normal heart sounds are S1 and S2, but additional sounds like S3 or S4, murmurs, or abnormal splitting can indicate underlying heart conditions such as valve disorders, heart failure, or hypertension.
Yes, heart sounds can vary based on age, heart rate, physical activity, and individual anatomy. For example, children often have faster heart rates, and athletes may have a louder S1 sound.
Heart sounds are listened to using a stethoscope, a process called auscultation. Healthcare providers assess the timing, quality, and intensity of the sounds to diagnose potential cardiac issues.