Bronchial breath sounds are a type of lung sound characterized by their high-pitched, hollow, and loud quality, often described as similar to breathing through a large tube. These sounds occur when air moves through the larger airways, such as the bronchi, rather than the smaller alveoli, typically due to consolidation or increased air density in the lungs. Conditions like pneumonia, pulmonary edema, or lung tumors can cause bronchial breath sounds by altering the normal air distribution and tissue density within the lungs. Understanding the mechanisms behind these sounds is crucial for healthcare professionals, as they serve as important diagnostic indicators of underlying respiratory pathologies.
Explore related products






What You'll Learn
- Airflow Dynamics: Increased airflow in bronchi amplifies sound due to reduced impedance and turbulence
- Consolidation: Inflamed or infected lung tissue transmits sounds more efficiently, enhancing bronchial tones
- Location: Sounds are louder over affected areas due to proximity to consolidated lung tissue
- Frequency: Lower-pitched sounds result from larger airway involvement and increased air movement
- Intensity: Loudness increases with greater airflow and reduced resistance in bronchial passages
![]()
Airflow Dynamics: Increased airflow in bronchi amplifies sound due to reduced impedance and turbulence
The intensity of bronchial breath sounds is directly influenced by the dynamics of airflow within the bronchi. When airflow increases, the resulting sound is amplified due to two key physical principles: reduced impedance and increased turbulence. Impedance, in this context, refers to the resistance to airflow within the bronchial tubes. As airflow velocity rises, the air column behaves more like a fluid, reducing resistance and allowing sound waves to propagate more freely. This phenomenon is akin to how a louder sound is produced when air moves rapidly through a flute or whistle.
To understand this better, consider the analogy of water flowing through a pipe. When water flows slowly, it encounters more friction and resistance, dampening any noise. However, as the flow rate increases, the water overcomes friction, creating turbulence and amplifying the sound. Similarly, in the bronchi, higher airflow velocities reduce impedance, enabling sound waves to travel with less attenuation. This principle is particularly evident in conditions like asthma or chronic obstructive pulmonary disease (COPD), where forced exhalation increases airflow, making bronchial sounds more pronounced.
Clinicians can leverage this understanding to assess respiratory health. For instance, during auscultation, a patient’s forced expiration can reveal amplified bronchial sounds, indicating potential airway obstruction or inflammation. Practical tips for healthcare providers include instructing patients to exhale deeply and steadily while listening with a stethoscope over the bronchi. This technique enhances the detection of abnormal sounds, such as wheezing or rhonchi, which are often associated with increased airflow and turbulence.
A comparative analysis of normal versus pathological airflow dynamics further highlights the importance of this concept. In healthy individuals, airflow is balanced, producing moderate bronchial sounds. In contrast, conditions like bronchitis or pneumonia can increase airflow due to inflammation, leading to louder, more turbulent sounds. Recognizing these differences is crucial for accurate diagnosis and treatment planning. For example, in children aged 5–12, amplified bronchial sounds may suggest acute bronchitis, while in adults over 65, it could indicate COPD exacerbation.
In conclusion, the amplification of bronchial breath sounds due to increased airflow is a critical diagnostic marker. By understanding the role of reduced impedance and turbulence, healthcare providers can better interpret auscultation findings and tailor interventions. Practical applications, such as guided breathing techniques during examination, enhance the utility of this knowledge in clinical settings. This insight not only deepens our understanding of respiratory physiology but also improves patient care through more precise assessments.
Crafting Sonic Art: A Beginner's Guide to Creating Sound Collages
You may want to see also
Explore related products






![]()
Consolidation: Inflamed or infected lung tissue transmits sounds more efficiently, enhancing bronchial tones
Inflamed or infected lung tissue, a condition known as consolidation, alters the way sound travels through the lungs. Normally, air-filled alveoli act as insulators, dampening the transmission of breath sounds. However, when inflammation or infection fills these air spaces with fluid or pus, the tissue becomes denser. This increased density enhances the conduction of sound waves, amplifying bronchial breath sounds during auscultation. Clinicians often describe these sounds as louder, more hollow, and resembling the noise made when breathing through a cardboard tube.
Consider the analogy of tapping on a drum. A tight, unbroken drumhead produces a clear, resonant sound. Conversely, a drumhead with holes or loose areas muffles the sound. Similarly, healthy lung tissue, with its air-filled alveoli, acts like the compromised drumhead, dampening breath sounds. Consolidated lung tissue, however, behaves like the tight drumhead, transmitting sounds more efficiently. This principle underlies why bronchial breath sounds become more pronounced in conditions like pneumonia, where consolidation is a hallmark feature.
To identify consolidation-related bronchial breath sounds, follow these steps during auscultation: First, ensure the patient is seated upright and relaxed. Place the diaphragm of the stethoscope firmly on the chest wall, starting at the anterior chest and moving posteriorly. Listen for breath sounds that are louder than normal, with a quality that seems to originate from deeper within the lung. Compare the sounds bilaterally, as asymmetry can be a key indicator of localized consolidation. Remember, these sounds are typically heard over areas of the lung affected by infection or inflammation, so correlate your findings with the patient’s symptoms and medical history.
While consolidation enhances bronchial breath sounds, it’s crucial to differentiate these from other abnormal lung sounds. For instance, wheezes are high-pitched and musical, often associated with asthma or COPD, whereas crackles (formerly called rales) suggest fluid in the alveoli or small airways. Bronchial breath sounds in consolidation are distinct in their increased intensity and hollowness. If you’re uncertain, consider using a recording device to capture the sounds for review or consultation with a colleague. Early recognition of these sounds can prompt timely diagnostic imaging, such as a chest X-ray or CT scan, to confirm consolidation and guide treatment.
Finally, understanding the mechanism behind consolidation-enhanced bronchial breath sounds has practical implications for patient care. For example, in a patient with suspected pneumonia, the presence of these sounds can support the diagnosis and influence antibiotic selection. Additionally, monitoring changes in breath sounds over time can help assess treatment efficacy. For healthcare providers, mastering this auscultation skill is essential, as it provides a non-invasive, cost-effective method to evaluate lung health. Pairing this knowledge with a systematic approach to physical examination ensures a comprehensive assessment of respiratory conditions.
Effective Sound Insulation Costs: A Comprehensive Guide to Quieter Spaces
You may want to see also
Explore related products





![]()
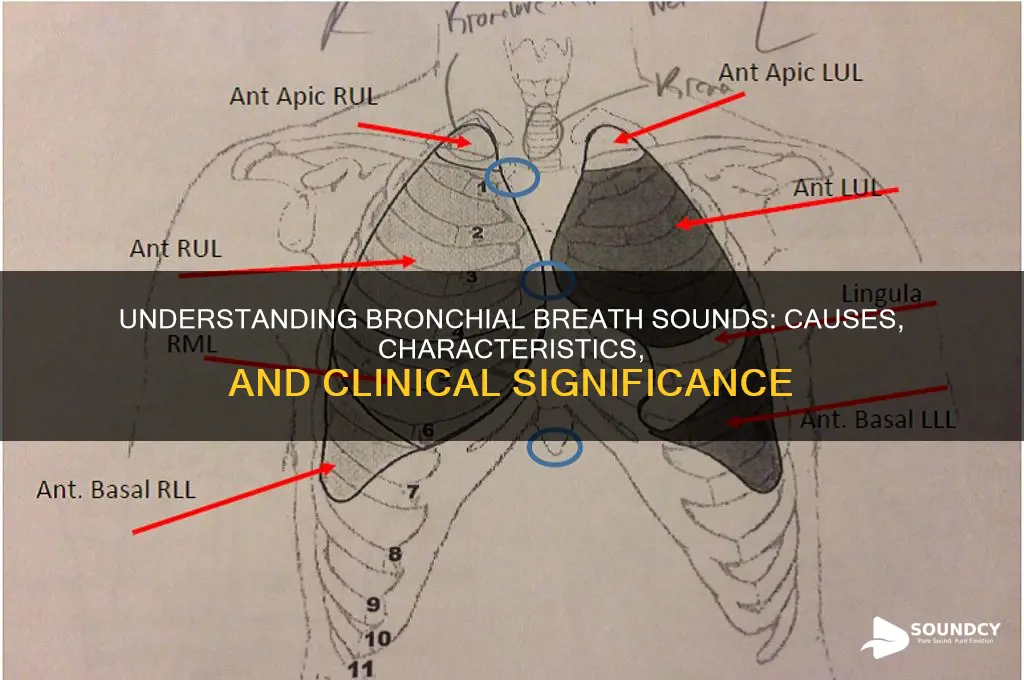
Location: Sounds are louder over affected areas due to proximity to consolidated lung tissue
Bronchial breath sounds are amplified in specific areas of the chest due to their proximity to consolidated lung tissue, a phenomenon that serves as a critical diagnostic clue. When pneumonia, pulmonary edema, or lung tumors cause consolidation, the air passages become surrounded by denser, fluid-filled or solid tissue. This anatomical shift reduces the distance between the bronchi and the chest wall, allowing the transmission of sound with greater intensity. Clinicians can exploit this principle by using a stethoscope to identify louder breath sounds over affected regions, pinpointing the extent and location of the pathology.
To effectively utilize this principle, auscultate systematically, comparing the volume of breath sounds across lung fields. Begin by dividing the chest into quadrants or specific anatomical zones, such as the upper and lower lobes. Note areas where breath sounds are disproportionately loud, as these may correspond to consolidated tissue. For instance, in a patient with right lower lobe pneumonia, bronchial breath sounds will be most prominent in the infrascapular region. Pairing this technique with percussion (which reveals dullness over consolidated areas) enhances diagnostic accuracy, particularly in distinguishing between conditions like pneumonia and chronic obstructive pulmonary disease (COPD).
The louder bronchial breath sounds over consolidated areas are not merely a passive observation but a direct consequence of altered lung mechanics. In healthy lungs, air-filled alveoli act as insulators, dampening the transmission of sound from the bronchi to the chest wall. However, consolidation replaces air with denser material, creating a conductive pathway for sound. This principle is akin to hearing a conversation more clearly in a room with carpet (consolidated tissue) versus one with thick curtains (normal lung parenchyma). Understanding this mechanism transforms auscultation from a rote task into a dynamic, problem-solving tool.
Practical tips for optimizing detection include ensuring proper stethoscope placement, with the diaphragm firmly pressed against the skin to minimize air gaps. Encourage patients to breathe deeply and slowly, as this maximizes the audibility of bronchial breath sounds. For pediatric or uncooperative patients, correlate findings with chest radiographs or point-of-care ultrasound, which can visualize consolidation directly. Remember, louder bronchial breath sounds are not inherently pathological; they must be interpreted in the context of other clinical signs, such as fever, cough, or leukocytosis, to confirm an infectious or inflammatory etiology.
How to Identify a Ripe Watermelon by Its Sound and Feel
You may want to see also
Explore related products






![]()
Frequency: Lower-pitched sounds result from larger airway involvement and increased air movement
The pitch of bronchial breath sounds is a critical diagnostic clue, with lower frequencies indicating involvement of larger airways. This phenomenon occurs because air moving through wider passages creates vibrations at a slower rate, producing deeper, more resonant sounds. For instance, a healthy individual’s breath sounds are typically higher-pitched and softer, originating from smaller alveoli and bronchioles. In contrast, conditions like pneumonia, chronic obstructive pulmonary disease (COPD), or consolidation can cause air to move through larger, more central airways, resulting in the characteristic low-pitched bronchial sounds. Auscultation reveals these as prolonged, louder expiratory phases, often described as “tubular” or “hollow.”
To identify these sounds effectively, clinicians should focus on both the frequency and quality of the breath sounds. Lower-pitched bronchial sounds are best detected using a stethoscope’s bell, which is more sensitive to deeper frequencies. Positioning the patient in an upright or slightly leaned-forward posture can enhance sound transmission, as this reduces chest wall interference. For pediatric patients, particularly those under 5 years old, larger airway involvement is more common due to their naturally smaller bronchial anatomy, making lower-pitched sounds a frequent finding even in mild respiratory conditions.
A comparative analysis highlights the importance of context in interpreting these sounds. While lower-pitched bronchial sounds in a patient with a history of COPD may indicate acute exacerbation, the same finding in a child with viral bronchitis could be a normal variant. Clinicians must correlate auscultatory findings with symptoms, imaging, and patient history to avoid misdiagnosis. For example, a chest X-ray confirming consolidation in a pneumonia patient reinforces the significance of low-pitched sounds, whereas their presence in asthma without consolidation may suggest excessive airway turbulence rather than infection.
Practical tips for differentiating bronchial sounds include comparing bilateral lung fields to identify asymmetry, a key indicator of localized pathology. Additionally, encouraging the patient to breathe deeply and slowly amplifies sound intensity, making subtle changes more detectable. For novice practitioners, recording auscultation findings immediately after examination ensures accuracy, as memory of sound nuances fades quickly. Understanding the relationship between airway size and sound frequency transforms auscultation from a passive skill to an active, diagnostic tool, enabling precise localization of respiratory abnormalities.
Exploring Alechmy Sound Libraries: A Comprehensive Guide to Audio Innovation
You may want to see also
Explore related products






![]()
Intensity: Loudness increases with greater airflow and reduced resistance in bronchial passages
Bronchial breath sounds are louder than normal lung sounds due to increased airflow and reduced resistance in the bronchial passages. This phenomenon is a key characteristic that distinguishes bronchial sounds from other respiratory sounds, such as vesicular or crackling sounds. The intensity of these sounds is directly proportional to the airflow velocity and the diameter of the airways. When air moves rapidly through a large, unobstructed bronchial tube, it creates a higher-pitched and louder sound, often described as "tubular" or "hollow."
To understand this concept, consider the physics of sound production in the respiratory system. As air flows through the bronchial passages, it causes the walls of the airways to vibrate. The frequency and amplitude of these vibrations determine the pitch and loudness of the resulting sound. In the case of bronchial breath sounds, the increased airflow and reduced resistance allow for more vigorous vibrations, leading to a louder and often higher-pitched sound. This is particularly noticeable during inspiration, when the airflow is more rapid and forceful.
Practical Application: Clinicians can use the intensity of bronchial breath sounds as a diagnostic tool. For instance, in patients with conditions like chronic obstructive pulmonary disease (COPD) or asthma, the loudness of bronchial sounds may vary depending on the degree of airway obstruction. During an asthma exacerbation, the increased resistance in the airways can lead to decreased intensity of bronchial sounds. Conversely, in COPD patients with hyperinflated lungs and reduced airflow resistance, the bronchial sounds may be louder and more pronounced. Auscultation should be performed with a stethoscope, focusing on the anterior and posterior chest walls, and comparing the sounds between different lung fields to identify abnormalities.
Comparative Analysis: The intensity of bronchial breath sounds can be compared to the sound of air flowing through a large pipe versus a narrow straw. In the case of the pipe, the air moves freely with minimal resistance, producing a loud, clear sound. Similarly, in bronchial passages with reduced resistance, the airflow generates a louder sound. Conversely, when air flows through a narrow straw, the increased resistance dampens the sound, analogous to the reduced intensity of bronchial sounds in obstructed airways. This comparison highlights the importance of airflow dynamics in determining the loudness of respiratory sounds.
Takeaway and Tips: For healthcare professionals, recognizing the intensity of bronchial breath sounds is crucial for assessing respiratory health. To optimize auscultation, ensure the patient is in a comfortable position, preferably sitting upright, as this facilitates better airflow. Use a high-quality stethoscope and apply gentle pressure to the chest wall to enhance sound transmission. In pediatric patients, particularly those under 5 years old, bronchial breath sounds may be more difficult to distinguish due to smaller airway diameters and higher respiratory rates. In such cases, focus on the upper lung fields, where bronchial sounds are more likely to be audible. By mastering the interpretation of bronchial sound intensity, clinicians can improve their diagnostic accuracy and patient care.
Mastering the Art of Authentic Spanish Guitar Techniques and Tone
You may want to see also
Frequently asked questions
Bronchial breath sounds are lung sounds characterized by their high-pitched, hollow, and loud quality, typically heard over the trachea but can be abnormal when heard over other lung areas.
Bronchial breath sounds over the lungs are often caused by the consolidation of lung tissue, as seen in conditions like pneumonia, where air-filled alveoli are replaced by solid material, transmitting sounds more efficiently.
Normal breath sounds are softer and have a lower pitch, while bronchial breath sounds are louder, higher-pitched, and more tubular, resembling breathing through a hollow pipe.
Abnormal bronchial breath sounds are associated with conditions like pneumonia, lung abscess, pulmonary edema, and consolidation due to tuberculosis or tumors.
Bronchial breath sounds are diagnosed through auscultation using a stethoscope. Their presence, location, and characteristics are evaluated alongside patient history, physical exam, and imaging studies like chest X-rays to determine the underlying cause.