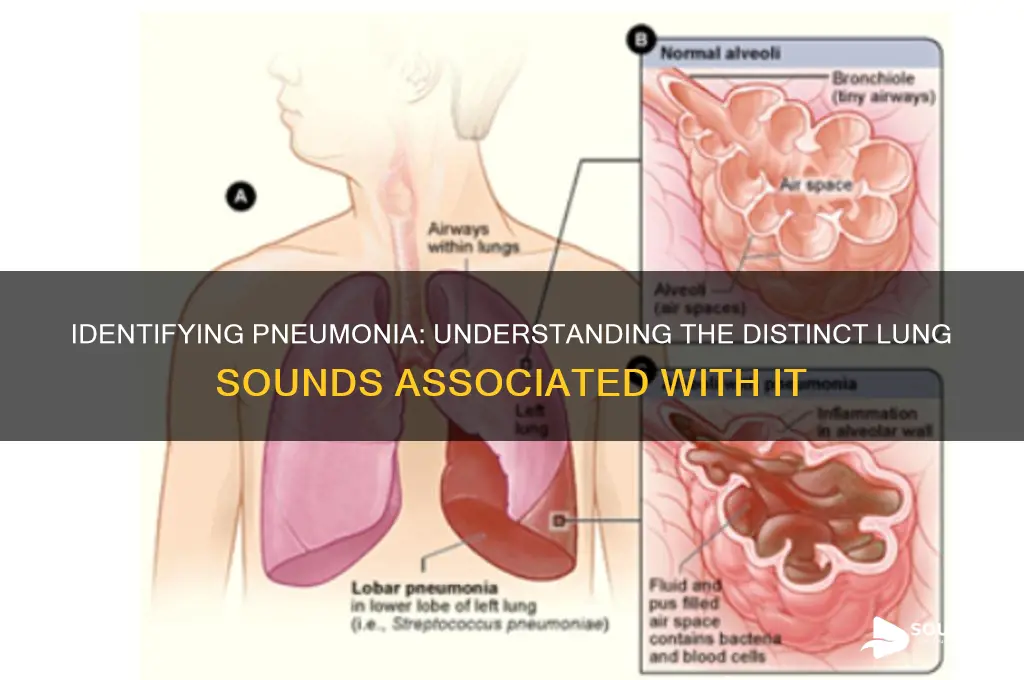
Pneumonia, an infection that inflames the air sacs in one or both lungs, often produces distinct lung sounds that aid in its diagnosis. One of the most characteristic sounds associated with pneumonia is crackles, also known as rales. These are discontinuous, high-pitched, bubbling or rattling sounds that occur during inhalation, caused by the movement of air through fluid-filled alveoli or airways. Crackles are typically heard in the affected area of the lung and can vary in intensity depending on the severity of the infection. Additionally, bronchial breath sounds may be audible, which are louder and more pronounced than normal breath sounds, indicating consolidation of the lung tissue. These auscultatory findings, combined with other clinical symptoms like cough, fever, and shortness of breath, help healthcare providers identify pneumonia and determine its extent.
| Characteristics | Values |
|---|---|
| Type of Lung Sound | Crackles (formerly called rales) |
| Description | Short, discontinuous, bubbling or popping sounds during inspiration |
| Mechanism | Caused by the opening of small airways filled with fluid or secretions |
| Location | Often heard in the bases of the lungs but can be diffuse |
| Associated Conditions | Pneumonia, pulmonary edema, interstitial lung disease, bronchiectasis |
| Timing | Typically heard during inspiration |
| Intensity | Can range from fine (soft) to coarse (loud) |
| Clinical Significance | Indicates alveolar or small airway involvement in pneumonia |
| Differential Diagnosis | Distinguish from wheezes (continuous musical sounds in asthma/COPD) |
| Diagnostic Tool | Auscultation with a stethoscope |
| Treatment Implication | Presence of crackles suggests need for further evaluation and management |
Explore related products






What You'll Learn
![]()
Crackles (fine or coarse)
Crackles, often described as the popping or crackling sounds heard during inhalation, are a hallmark of pneumonia, particularly in its early stages. These sounds occur when air moves through airways filled with fluid, mucus, or pus, causing the small airways to snap open. Fine crackles, high-pitched and brief, are typically heard at the end of inspiration and are associated with conditions like pneumonia, where fluid accumulates in the alveoli. Coarse crackles, louder and more prolonged, suggest larger airways are involved and can indicate more severe inflammation or consolidation. Recognizing these distinctions is crucial for clinicians to pinpoint the extent and nature of lung involvement in pneumonia.
To auscultate for crackles effectively, position the patient upright and use a stethoscope with firm pressure on the chest wall. Fine crackles may require the patient to take slow, deep breaths, while coarse crackles are often more audible during normal breathing. In pediatric cases, fine crackles are more commonly detected in children under five, as their smaller airways are more susceptible to fluid accumulation. For older adults, coarse crackles may predominate due to age-related changes in lung tissue elasticity. Documenting the location and intensity of crackles helps in monitoring disease progression and response to treatment, such as antibiotics or bronchodilators.
From a diagnostic perspective, crackles serve as a key indicator of pneumonia but must be differentiated from other conditions like heart failure or chronic obstructive pulmonary disease (COPD). Fine crackles in pneumonia are often localized to the affected lobe or segment, whereas in heart failure, they are typically basal and bilateral. Coarse crackles in pneumonia may mimic those in COPD, but the absence of wheezing and the acute onset of symptoms in pneumonia provide important clues. Combining auscultation findings with imaging, such as chest X-rays, and laboratory tests enhances diagnostic accuracy and guides appropriate management.
Practical tips for healthcare providers include using a systematic approach to auscultation, starting from the apical to the basal regions of the lungs. Encourage patients to breathe deeply and slowly to maximize the detection of fine crackles. In resource-limited settings, relying on auscultation becomes even more critical, as advanced imaging may not be readily available. Educating patients about the significance of crackles can also improve adherence to treatment, as understanding the link between lung sounds and pneumonia fosters a sense of urgency in seeking care.
In conclusion, crackles are a vital auditory clue in diagnosing and managing pneumonia, with fine and coarse variants offering insights into the disease’s severity and location. Mastery of auscultation techniques, coupled with clinical context, ensures accurate interpretation of these lung sounds. Whether in a bustling hospital or a remote clinic, recognizing crackles empowers healthcare providers to deliver timely and effective care, ultimately improving patient outcomes in pneumonia.
C-Sounding Letters: Unveiling the Surprising Alphabet Twins in English
You may want to see also
Explore related products






![]()
Bronchial breath sounds
To identify bronchial breath sounds in pneumonia, follow these steps: first, ensure the patient is in a quiet room and breathing normally. Place the stethoscope firmly over the suspected area of consolidation, typically the lower lobes in adults or the right middle lobe in children. Listen for a sound that is louder, higher-pitched, and more prolonged than normal breath sounds. Compare the sound to the unaffected area to highlight the difference. If bronchial breath sounds are present, they may persist throughout both inhalation and exhalation, a key indicator of underlying pathology.
While bronchial breath sounds are a hallmark of pneumonia, they are not exclusive to this condition. They can also occur in other diseases like lung cancer, pulmonary edema, or tuberculosis, where consolidation or fluid accumulation is present. However, in pneumonia, these sounds are often accompanied by additional findings such as crackles (rales) or diminished breath sounds in severe cases. Contextualizing these sounds with patient history, symptoms, and imaging results is crucial for accurate diagnosis.
A practical tip for healthcare providers is to use the "whispered pectoriloquy" test to confirm bronchial breath sounds. Ask the patient to whisper a phrase like "ninety-nine" while you listen with the stethoscope. If the whispered words are clearly audible over the consolidated area, it confirms the presence of bronchial breath sounds. This simple test enhances diagnostic confidence and can be particularly useful in resource-limited settings where advanced imaging is unavailable.
In summary, bronchial breath sounds in pneumonia are characterized by their increased intensity, high pitch, and tubular quality, reflecting the consolidation of lung tissue. Recognizing these sounds requires careful auscultation, comparison with unaffected areas, and consideration of associated clinical findings. While not specific to pneumonia, their presence, especially when confirmed by tests like whispered pectoriloquy, provides valuable insight into the underlying pathology. Mastery of this skill is essential for clinicians to accurately diagnose and manage respiratory conditions.
Discover the Rich, Warm, and Expressive Sound of the Viola
You may want to see also
Explore related products






![]()
Rhonchi (coarse rattling)
Rhonchi, often described as a coarse rattling sound, are a hallmark of certain respiratory conditions, including pneumonia. These sounds occur when air moves through airways narrowed by mucus, inflammation, or secretions. Unlike fine crackles, which are brief and high-pitched, rhonchi are continuous, low-pitched, and resemble snoring. They are typically heard during both inspiration and expiration, though they may be more prominent during expiration. Identifying rhonchi is crucial for clinicians, as they provide valuable insight into the underlying pathology and guide treatment decisions.
To detect rhonchi, healthcare providers use a stethoscope during auscultation, focusing on areas of the lung where consolidation or mucus accumulation is suspected. The sound’s intensity and location can vary depending on the severity of the condition. For instance, rhonchi in pneumonia often localize to the affected lobe or segment, reflecting the site of infection and inflammation. Patients may also exhibit symptoms such as cough, fever, and shortness of breath, which, when combined with auscultatory findings, strengthen the diagnosis. Early recognition of rhonchi can prompt timely interventions, such as chest physiotherapy or bronchodilators, to clear airways and improve oxygenation.
From a comparative perspective, rhonchi differ significantly from other lung sounds associated with pneumonia. Wheezes, for example, are high-pitched and musical, typically linked to asthma or chronic obstructive pulmonary disease (COPD), whereas rhonchi are deeper and more guttural. Fine crackles, another common finding in pneumonia, are short and discontinuous, often likened to the sound of walking on snow. Understanding these distinctions is essential for accurate diagnosis and management. Rhonchi specifically indicate the presence of substantial airway obstruction, often requiring targeted therapies to address the underlying cause.
For patients and caregivers, recognizing rhonchi can be a practical tool for monitoring respiratory health. If a coarse rattling sound is heard, especially in the context of fever, cough, or respiratory distress, seeking medical attention is imperative. Home management strategies, such as staying hydrated and using a humidifier, may provide temporary relief but should not replace professional care. Clinicians may prescribe mucolytics or perform chest physiotherapy to mobilize secretions and alleviate rhonchi. In severe cases, hospitalization for oxygen therapy or intravenous antibiotics may be necessary to treat the underlying pneumonia.
In conclusion, rhonchi serve as a critical auditory clue in the assessment of pneumonia, signaling airway obstruction due to mucus or inflammation. Their distinctive coarse rattling quality sets them apart from other lung sounds, making them a key diagnostic feature. By understanding their characteristics, healthcare providers and patients alike can take proactive steps to manage symptoms and address the root cause. Early detection and appropriate intervention are vital to improving outcomes and preventing complications in pneumonia cases accompanied by rhonchi.
Does Gypsum Board Effectively Block Noise? Soundproofing Facts Revealed
You may want to see also
Explore related products






![]()
Diminished breath sounds
To identify diminished breath sounds, healthcare providers should systematically auscultate all lung fields, comparing symmetry between corresponding areas on both sides. In pneumonia, these sounds are often more pronounced in the affected lobe or segment. For instance, a patient with right lower lobe pneumonia may exhibit decreased breath sounds over that region, accompanied by dullness to percussion and egophony. It is essential to differentiate this from other conditions like atelectasis or pleural effusion, which may present similarly but require distinct management approaches. Proper technique, including adequate stethoscope placement and patient positioning, is crucial for accurate assessment.
From a practical standpoint, documenting the extent and location of diminished breath sounds is vital for monitoring disease progression and response to treatment. For example, in a 65-year-old patient with community-acquired pneumonia, serial auscultation may reveal gradual improvement in breath sounds as antibiotics reduce inflammation and consolidation resolves. Conversely, persistent or worsening diminution could indicate complications such as abscess formation or empyema, necessitating advanced imaging or intervention. Nurses and physicians should communicate these findings clearly in the medical record and during handoffs to ensure continuity of care.
While diminished breath sounds are a hallmark of pneumonia, they are not pathognomonic and must be interpreted in the context of other clinical data. For instance, a history of fever, cough, and purulent sputum, coupled with chest X-ray findings of consolidation, strengthens the diagnosis. However, in immunocompromised patients or those with atypical pathogens, the presentation may be less classic, requiring a higher index of suspicion. Integrating auscultatory findings with laboratory results, imaging, and patient history provides a comprehensive understanding of the disease process, enabling tailored treatment strategies.
In conclusion, diminished breath sounds serve as a key auscultatory clue in pneumonia, reflecting the pathophysiological changes occurring within the lung parenchyma. Mastery of this finding enhances diagnostic accuracy and informs clinical decision-making. By combining meticulous auscultation with a holistic approach to patient assessment, healthcare providers can optimize outcomes for individuals with pneumonia, ensuring timely and effective management of this common yet potentially severe condition.
Understanding Vibrations: The Science Behind How They Create Sound Waves
You may want to see also
Explore related products






![]()
Egophony (changed voice resonance)
Egophony, a high-pitched, nasal quality to the voice during auscultation, is a distinctive lung sound often associated with pneumonia. This phenomenon occurs when inflamed or consolidated lung tissue alters the transmission of vocal vibrations, resulting in a sound reminiscent of the "E" in "say." Clinicians detect egophony by asking the patient to repeat a sustained vowel sound, such as "E," while listening with a stethoscope over the affected lung area. The presence of this sound is a valuable diagnostic clue, particularly in pneumonia, where it indicates localized consolidation or fluid accumulation in the lung parenchyma.
To identify egophony, follow these steps: instruct the patient to take a deep breath and sustain the "E" sound while you auscultate over the suspected area. Compare the sound to that produced over healthy lung tissue, noting any heightened pitch or nasal resonance. Be cautious not to confuse egophony with other adventitious sounds, such as wheezing or crackles, which have different characteristics and implications. For example, wheezing is musical and suggests airway obstruction, while crackles are brief, popping sounds often linked to fluid in the alveoli. Egophony’s unique quality lies in its vocalized, resonant nature, making it a specific marker for pneumonia-related consolidation.
From a comparative perspective, egophony stands out among other lung sounds due to its direct relationship with vocalization. Unlike rhonchi or stridor, which are independent of patient speech, egophony requires the patient’s active participation. This makes it both a diagnostic tool and a dynamic indicator of lung tissue changes. For instance, in children aged 5–12, egophony may be more pronounced due to smaller airway diameters and higher vocal pitch, whereas in older adults, it may be subtler but equally significant. Recognizing this sound can expedite diagnosis, particularly in resource-limited settings where advanced imaging is unavailable.
Practically, egophony serves as a bedside diagnostic aid, but its interpretation requires clinical context. For example, a patient with fever, cough, and unilateral egophony is highly suggestive of lobar pneumonia. However, egophony can also occur in conditions like pulmonary edema or lung abscess, so additional findings (e.g., dullness to percussion, increased tactile vocal fremitus) should be considered. To enhance accuracy, combine auscultation with other physical exam techniques and patient history. For instance, in a 45-year-old smoker with egophony and hemoptysis, tuberculosis or lung cancer may be differential diagnoses, necessitating further investigation.
In conclusion, egophony is a nuanced yet critical lung sound in pneumonia diagnosis, offering insights into the extent and location of lung consolidation. Its reliance on vocalization distinguishes it from other adventitious sounds, making it a unique tool in the clinician’s arsenal. By mastering its detection and interpretation, healthcare providers can improve diagnostic precision, particularly in settings where advanced imaging is inaccessible. Remember, while egophony is highly suggestive of pneumonia, it is not pathognomonic, and a comprehensive approach to patient assessment remains essential.
Understanding the Concept of a Sound Foot: A Comprehensive Guide
You may want to see also
Frequently asked questions
Crackles (also known as rales) are the most common lung sound associated with pneumonia.
Crackles occur due to fluid or mucus accumulation in the small airways, which is a hallmark of pneumonia.
Yes, wheezing can occur in pneumonia, especially if there is bronchial inflammation or airway narrowing.
Yes, diminished breath sounds can occur in pneumonia due to consolidation or reduced air movement in affected lung areas.
Yes, lung sounds can vary; for example, lobar pneumonia often presents with crackles, while bronchopneumonia may include wheezing or rhonchi.