Speech sound development refers to the process by which children learn to produce and articulate the sounds of their native language accurately and clearly. This developmental journey typically begins in infancy with cooing and babbling, progresses to the formation of first words around one year of age, and continues through early childhood as children refine their ability to produce complex sounds and sound combinations. By age 8, most children have mastered the full range of speech sounds in their language, though the timeline can vary. Speech sound development is influenced by factors such as hearing, oral motor skills, cognitive abilities, and linguistic exposure, making it a critical aspect of communication and language acquisition. Challenges in this area may lead to speech sound disorders, which can impact a child’s ability to be understood and their overall communication confidence.
| Characteristics | Values |
|---|---|
| Definition | Speech sound development refers to the process by which children learn to produce and use speech sounds (phonemes) accurately and appropriately in their native language. |
| Age Range | Typically begins at birth and continues through early childhood, with most sounds mastered by age 8. |
| Stages | 1. Cooing and Gooing (0-6 months): Early vocalizations. 2. Babbling (6-10 months): Repetitive syllables like "ba-ba." 3. First Words (12-18 months): Single words emerge. 4. Word Combinations (18-36 months): Two-word phrases. 5. Complex Sentences (3-5 years): Longer sentences with more accurate sounds. |
| Key Sounds | Sounds are acquired in a predictable order, e.g., /p/, /b/, /m/, /d/, /n/, /h/, /w/, /t/, /k/, /g/, /f/, /v/, /ch/, /j/, /s/, /z/, /sh/, /l/, /r/, /th/. |
| Influences | Affected by factors like hearing, oral motor skills, cognitive development, and language exposure. |
| Disorders | Delayed or disordered speech sound development may indicate conditions like articulation disorders, phonological disorders, or childhood apraxia of speech. |
| Assessment | Evaluated through standardized tests, speech samples, and observation by speech-language pathologists. |
| Intervention | Early intervention, speech therapy, and home practice are common strategies to support development. |
| Cultural Factors | Speech sound development varies across languages and cultures, influenced by the phonemic inventory of the native language. |
Explore related products





What You'll Learn
- Phonological Milestones: Key ages for acquiring speech sounds in typical development
- Speech Sound Disorders: Types, causes, and identification of articulation/phonological delays
- Phonemic Inventory: Development of sound repertoire in children over time
- Stimulation Strategies: Techniques to encourage correct speech sound production
- Assessment Tools: Methods for evaluating speech sound development in children
![]()
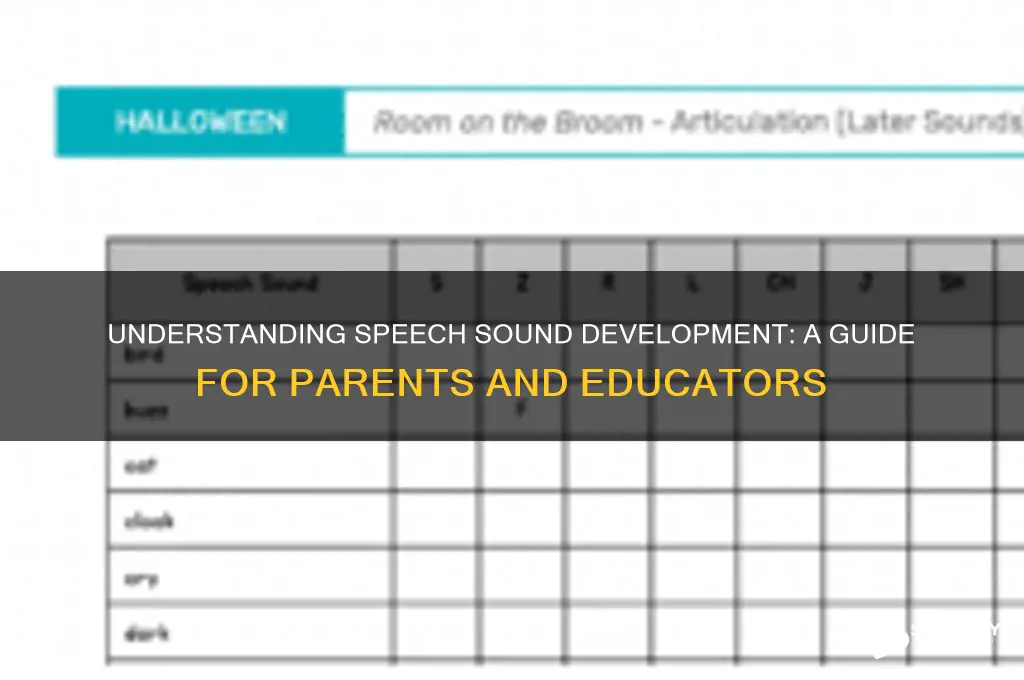
Phonological Milestones: Key ages for acquiring speech sounds in typical development
Speech sound development is a fascinating journey, marked by predictable milestones that reflect a child’s growing ability to produce and differentiate sounds. By age 3, most children can say the p, b, m, h, w, d, n, t, k, g sounds clearly, laying the foundation for intelligible speech. This early stage is critical, as it sets the stage for more complex sounds and word combinations. Parents and caregivers can support this process by engaging in simple, repetitive speech activities like singing nursery rhymes or labeling objects during play.
Between ages 3 and 4, children typically master additional sounds such as f, v, sh, zh, ch, j, and y. This period is a leap forward in phonological complexity, enabling children to articulate words like "fish," "juice," and "yellow." Mispronunciations like substituting "w" for "r" (e.g., "wabbit" for "rabbit") are common and often resolve naturally. However, if a child’s speech remains less than 50% intelligible to unfamiliar listeners by age 4, consulting a speech-language pathologist is advisable. Encouraging storytelling and reading aloud can enhance sound awareness during this phase.
The 5- to 7-year-old range is when children refine their speech, tackling more challenging sounds like s, z, l, r, and th. By age 7, most children can produce all speech sounds correctly, though some, like "r" and "th," may persist until age 8. Peer interactions and school environments play a significant role here, as children mimic and practice sounds in conversation. Parents can foster progress by gently correcting errors without causing self-consciousness and by incorporating games that emphasize specific sounds, such as tongue-twisters.
While these milestones provide a general roadmap, individual variation is normal. Late bloomers may take longer to reach certain markers, and bilingual children may follow a slightly different trajectory. The key is consistent exposure to clear speech models and opportunities for practice. Monitoring progress and celebrating small victories can make the process enjoyable for both child and caregiver, ensuring a positive and supportive environment for speech sound development.
Sound Healing and Catholicism: Exploring Spiritual Compatibility and Concerns
You may want to see also
Explore related products






![]()
Speech Sound Disorders: Types, causes, and identification of articulation/phonological delays
Speech sound development is a critical aspect of a child's communication skills, typically following a predictable sequence. By age 3, most children can produce the majority of speech sounds, though mastery continues until age 8. However, when this process stalls or deviates significantly, it may indicate a speech sound disorder (SSD). These disorders fall into two primary categories: articulation disorders and phonological disorders, each with distinct characteristics and implications for intervention.
Articulation disorders involve difficulties producing specific sounds, often due to physical challenges like tongue thrusting or improper jaw positioning. For instance, a 5-year-old might consistently substitute /w/ for /r/, saying "wabbit" instead of "rabbit." Identification often relies on error patterns: distortions, omissions, substitutions, or additions. Speech-language pathologists (SLPs) assess these errors against age-appropriate norms, such as the expectation that /s/ and /z/ should be mastered by age 6. Early intervention is key, as persistent articulation errors can lead to social stigma or reading difficulties. Practical tips for parents include modeling correct sounds during conversations and avoiding corrective feedback that may discourage the child.
Phonological disorders, in contrast, involve systematic errors in sound patterns, reflecting an underlying rule-based issue rather than motor difficulties. For example, a child might delete final consonants ("ca" for "cat") or front all sounds ("tate" for "kate"). These errors are not random but follow a consistent pattern, suggesting a breakdown in the child’s phonological system. SLPs analyze these patterns to determine the specific phonological processes at play, such as syllable reduction or stopping. Unlike articulation disorders, phonological disorders often require structured therapy targeting the child’s phonological system rather than individual sounds.
Causes of SSDs are multifaceted, ranging from neurological factors like childhood apraxia of speech to environmental influences, such as limited language exposure. Hearing loss, oral motor deficits, and cognitive delays are also common contributors. For instance, a child with untreated ear infections may develop articulation errors due to impaired auditory feedback. Identifying the root cause is crucial for tailored intervention, as treatments vary widely. For example, a child with apraxia requires intensive motor planning therapy, while one with hearing loss may benefit from hearing aids and auditory training.
Identification of SSDs begins with monitoring developmental milestones. Parents and caregivers should be alert to red flags, such as a 4-year-old who is still unable to produce early-developing sounds like /p/, /m/, or /b/. Formal assessment involves standardized tests like the Articulation for Phonology Screening Test (APST) or the Goldman-Fristoe Test of Articulation-3 (GFTA-3). SLPs also analyze speech samples to identify error patterns and determine whether the issue is articulatory or phonological. Early identification is critical, as untreated SSDs can impact academic performance, social interactions, and self-esteem. For example, a child struggling with /s/ and /z/ sounds may avoid reading aloud, hindering literacy development.
In conclusion, understanding the types, causes, and identification methods for speech sound disorders empowers parents, educators, and clinicians to address these challenges effectively. By recognizing the difference between articulation and phonological disorders, and by identifying underlying causes, targeted interventions can be implemented to support a child’s speech sound development. Whether through home strategies or professional therapy, early and informed action is essential for fostering clear communication and confidence.
Mastering the Art of Producing the N Sound: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Phonemic Inventory: Development of sound repertoire in children over time
Children begin life with a remarkable capacity to distinguish nearly every sound across all languages, a skill that fades as their native language shapes their auditory focus. By 6 months, infants start to hone in on the phonemes of their primary language, a process that marks the beginning of their phonemic inventory development. This inventory refers to the set of speech sounds a child can produce, which expands and refines over time. Initially, babbling encompasses a wide range of sounds, but by 12 months, children typically produce their first words, often using a limited set of phonemes like /p/, /b/, /m/, and /d/. This early stage lays the foundation for more complex sound production.
As children progress from 1 to 3 years, their phonemic inventory grows significantly, though errors are common. By age 3, most children can produce about 80% of phonemes correctly, with sounds like /k/, /g/, /n/, and vowels becoming more consistent. However, more challenging sounds, such as /r/, /l/, /s/, and /z/, often remain difficult. For instance, a 3-year-old might say "tat" for "cat" or "thoon" for "spoon." These errors are typical and reflect the ongoing development of articulatory precision. Parents and caregivers can support this process by modeling clear speech and engaging in activities like singing, rhyming, and reading aloud, which reinforce sound awareness.
Between ages 4 and 6, children’s phonemic inventories approach those of adults, with most mastering all phonemes by age 6. Sounds like /s/, /z/, /l/, and blends (e.g., "stop," "train") become more accurate during this period. However, some children may still struggle with specific sounds, particularly /r/ and /th/. Speech therapists often recommend targeted exercises, such as practicing words with the /r/ sound in isolation (e.g., "red," "rabbit") before moving to phrases and sentences. Early intervention is key; if a child’s speech is significantly unintelligible by age 4, consulting a speech-language pathologist can prevent long-term difficulties.
The development of a child’s phonemic inventory is not just about adding sounds but also about refining their production in different word positions and contexts. For example, a child might correctly say "sun" but struggle with "miss" or "measure." This refinement continues into the school years, with most children achieving adult-like speech by age 8. Encouraging activities like storytelling, tongue-twisters, and word games can enhance phonemic awareness and articulation. Understanding this developmental timeline helps caregivers set realistic expectations and provide appropriate support, ensuring children build a robust sound repertoire for clear communication.
Exploring Prince William Sound, Alaska
You may want to see also
Explore related products






![]()
Stimulation Strategies: Techniques to encourage correct speech sound production
Speech sound development is a complex process that unfolds in predictable stages, but some children may need extra support to master certain sounds. Stimulation strategies play a crucial role in encouraging correct speech sound production, particularly for those who struggle with articulation or phonological disorders. These techniques are designed to create a supportive environment where children can practice and refine their speech skills effectively.
One effective stimulation strategy is auditory bombardment, which involves repeated exposure to the target sound in various contexts. For instance, if a child is working on the /r/ sound, incorporate words like "rabbit," "car," and "star" into daily conversations, stories, or songs. Research suggests that consistent exposure to the sound in different words and sentences helps the child’s brain internalize its correct production. Pair this with visual aids, such as flashcards or pictures, to reinforce the auditory input. This method is particularly beneficial for children aged 4–7, when speech sound development is most active.
Another powerful technique is tactile-kinesthetic cueing, which uses physical prompts to guide the child’s articulators (lips, tongue, jaw) into the correct position. For example, to teach the /s/ sound, gently place your hand under the child’s chin to prevent jaw drop while they attempt the sound. For the /k/ sound, lightly touch the back of their tongue with a tongue depressor to encourage proper placement. This method is especially useful for children who struggle with motor planning for speech. However, be cautious not to apply too much pressure, as it may cause discomfort or discourage practice.
Phonics-based activities are also highly effective, particularly for school-aged children (6–9 years). Incorporate games or worksheets that focus on the target sound, such as word searches, rhyming activities, or minimal pairs exercises (e.g., "bat" vs. "cat"). These activities not only reinforce the sound but also improve phonological awareness, a critical skill for reading and spelling. For instance, a child working on the /th/ sound could practice saying and identifying words like "this," "that," and "the" in a sentence.
Finally, modeling and feedback are essential components of any stimulation strategy. Demonstrate the correct production of the target sound clearly and exaggeratedly, then have the child imitate you. Provide immediate, specific feedback, such as, "Great job rounding your lips for the /w/ sound!" or "Try keeping your tongue behind your teeth for the /l/ sound." Positive reinforcement, like praise or a sticker chart, can motivate children to keep practicing. For younger children (ages 3–5), keep sessions brief (5–10 minutes) and engaging, using toys or play to make learning fun.
In conclusion, stimulation strategies require patience, consistency, and creativity. By combining auditory bombardment, tactile-kinesthetic cueing, phonics-based activities, and effective modeling with feedback, caregivers and speech-language professionals can create a tailored approach to support each child’s unique needs. The key is to make practice enjoyable and integrated into daily routines, ensuring steady progress in speech sound development.
Unraveling the Mystical Hoots: How to Describe an Owl's Sound
You may want to see also
Explore related products




![]()
Assessment Tools: Methods for evaluating speech sound development in children
Speech sound development is a critical aspect of a child's communication skills, typically unfolding in a predictable sequence from infancy to early childhood. By age 3, most children can produce many sounds clearly, and by age 8, they should articulate all sounds correctly. However, identifying delays or disorders early is essential for timely intervention. Assessment tools play a pivotal role in this process, offering structured methods to evaluate a child’s speech sound development accurately.
Standardized Tests: The Gold Standard for Precision
One of the most reliable methods for evaluating speech sound development is through standardized tests. Tools like the *Arthur Assessment for Children (GFTA-3)* or the *Pronunciation Test for Children* provide norm-referenced scores, allowing clinicians to compare a child’s performance against age-matched peers. These tests typically involve a list of words or phrases the child is asked to repeat, with errors analyzed based on sound omissions, substitutions, or distortions. For instance, a 4-year-old should correctly produce /p/, /b/, and /m/, while struggles with /r/ or /th/ might be developmentally appropriate. Standardized tests are ideal for children aged 2–12 and require 15–30 minutes to administer, offering quantifiable data for tracking progress.
Language Sampling: Capturing Speech in Context
For a more naturalistic approach, language sampling involves recording a child’s spontaneous speech during play or conversation. Clinicians analyze a 5–10 minute sample, noting phonological processes (e.g., final consonant deletion in "ca" for "cat") and sound inventories. This method is particularly useful for children under 3, who may not cooperate with structured tests. For example, a clinician might observe a 2-year-old saying "tat" for "cat," indicating a typical fronting error. While less structured, language sampling provides insights into a child’s speech in real-world contexts, though it requires expertise to interpret accurately.
Parent and Teacher Reports: Harnessing Everyday Observations
Informal assessment tools, such as parent and teacher questionnaires, complement formal evaluations by capturing a child’s speech across various settings. Instruments like the *Early Language Milestone Checklist* or *Speech Sound Disorders Screener* ask caregivers to rate a child’s clarity or identify specific sound errors. For instance, a parent might note that their 5-year-old frequently says "wabbit" instead of "rabbit." These reports are quick to administer and cost-effective but rely on subjective observations. They are best used as screening tools, flagging potential issues for further evaluation by a professional.
Technology-Based Assessments: Modernizing Evaluation
Advancements in technology have introduced innovative tools like speech recognition software and mobile apps. Apps such as *Speech Tutor* or *Articulation Station* provide interactive exercises and automated feedback on sound production. While not replacements for clinical judgment, these tools engage children in the assessment process, making it more enjoyable. For example, a 6-year-old might practice /s/ blends through a game, with the app analyzing accuracy. These methods are particularly effective for older children (ages 5–10) and can supplement traditional assessments, though they require calibration to ensure reliability.
In conclusion, evaluating speech sound development requires a multifaceted approach, combining standardized tests, naturalistic observations, caregiver insights, and technological aids. Each method has strengths and limitations, and clinicians often use a combination to ensure a comprehensive understanding of a child’s needs. Early and accurate assessment is key to fostering clear communication, a foundation for academic and social success.
How Fast Does Sound Travel in Miles Per Hour?
You may want to see also
Frequently asked questions
Speech sound development refers to the process by which children learn to produce and use the sounds of their native language accurately and appropriately.
Children typically begin producing their first speech sounds, such as cooing and babbling, around 6 months of age, with more recognizable words emerging between 12 and 18 months.
The stages include phonological awareness (understanding sounds), babbling, first words, consonant and vowel production, and eventually mastering complex sound combinations, usually by age 8.
Difficulties can arise due to factors like hearing impairments, developmental delays, articulation disorders, or limited language exposure, though some errors are normal in early stages.
Parents can support development by engaging in conversations, reading aloud, modeling correct pronunciation, and seeking professional help if concerns arise about their child’s speech clarity.