The second heart sound (S2) is a crucial component of the cardiac cycle, representing the closure of the aortic and pulmonary valves at the beginning of diastole. It is typically described as a sharp, high-pitched dub sound and is best heard at the base of the heart. S2 marks the end of ventricular ejection and the transition to the relaxation phase of the heart, ensuring proper blood flow through the circulatory system. Understanding S2 is essential for diagnosing cardiovascular conditions, as abnormalities in its timing, intensity, or splitting can indicate valve disorders, hypertension, or other cardiac issues.
| Characteristics | Values |
|---|---|
| Definition | The second heart sound (S2) is one of the heart sounds heard through a stethoscope, marking the end of ventricular systole and the beginning of diastole. |
| Cause | Closure of the aortic (A2) and pulmonic (P2) valves as blood flow from the ventricles to the aorta and pulmonary artery ceases. |
| Timing | Occurs at the end of ventricular systole, after the first heart sound (S1). |
| Components | Consists of two main components: A2 (aortic valve closure) and P2 (pulmonic valve closure). |
| Normal Split | A physiological split S2 is heard in inspiration due to increased blood flow to the right heart, delaying P2 slightly relative to A2. |
| Intensity | P2 is typically softer than A2 in adults, but may be louder in children or certain conditions. |
| Location | A2 is best heard at the 2nd right intercostal space (aortic area), while P2 is best heard at the 2nd left intercostal space (pulmonic area). |
| Pathological Changes | Wide or paradoxical splitting, fixed splitting, or a single S2 can indicate conditions like bundle branch block, hypertension, or valvular disease. |
| Clinical Significance | Abnormalities in S2 can help diagnose valvular disorders, pulmonary hypertension, or conduction system diseases. |
Explore related products


$83.47 $71.99




What You'll Learn
- Components: Aortic and pulmonary valve closures create the second heart sound (S2)
- Timing: S2 occurs at the end of ventricular systole, marking its conclusion
- Characteristics: S2 is typically louder and higher pitched than the first heart sound
- Physiology: Reflects the closure of semilunar valves, separating ventricles from arteries
- Abnormalities: Split, wide, or paradoxical S2 may indicate valve or cardiac issues
![]()
Components: Aortic and pulmonary valve closures create the second heart sound (S2)
The second heart sound (S2) is a critical marker in cardiac auscultation, often described as the "dub" in the classic "lub-dub" rhythm. This sound is not a singular event but a composite of two distinct components: the closure of the aortic valve and the closure of the pulmonary valve. These closures occur at slightly different times, creating a split sound that can provide valuable insights into cardiovascular health. Understanding the mechanics behind S2 is essential for clinicians to diagnose conditions like valve disorders or pulmonary hypertension.
Analytically, the aortic valve closure typically precedes the pulmonary valve closure, resulting in a physiological splitting of S2. During inspiration, the intrathoracic pressure decreases, causing the pulmonary valve to close slightly later than the aortic valve, which is more pronounced in children and young adults. Conversely, during expiration, the split narrows or disappears. This dynamic is crucial for differentiating normal physiology from pathological conditions. For instance, a widened or fixed split S2 may indicate right bundle branch block or pulmonary stenosis, while a paradoxical split (wider during expiration) can suggest left bundle branch block or severe left-sided heart disease.
Instructively, to auscultate S2 effectively, place the diaphragm of the stethoscope over the second intercostal space along the left sternal border (aortic area) and the third left intercostal space (pulmonic area). Listen carefully for the timing and quality of the sound. Normal S2 is higher pitched than the first heart sound (S1) and reflects the end of ventricular systole. Clinicians should note any changes in intensity, splitting, or merging of the components, as these can indicate underlying issues. For example, a soft or muffled S2 may suggest aortic stenosis, while a loud, snapping sound could point to pulmonary hypertension.
Persuasively, mastering the nuances of S2 is not just an academic exercise but a practical skill that can save lives. Early detection of abnormalities in valve closures can lead to timely interventions, such as medication adjustments, surgical repairs, or lifestyle modifications. For instance, a patient with a widened split S2 might benefit from further diagnostic tests like an electrocardiogram (ECG) or echocardiogram to rule out significant cardiac pathology. Ignoring these subtle cues could delay treatment and worsen outcomes, particularly in vulnerable populations like the elderly or those with pre-existing heart conditions.
Comparatively, while S1 is primarily associated with mitral and tricuspid valve closures, S2’s complexity lies in its dual origins. The aortic component is usually louder and occurs earlier, while the pulmonary component is softer and slightly delayed. This contrast highlights the importance of precise auscultation techniques. Unlike S1, which is relatively constant, S2’s variability makes it a more sensitive indicator of hemodynamic changes. For example, in patients with atrial septal defects, the increased blood flow to the right heart can accentuate the pulmonary component of S2, making it disproportionately loud compared to the aortic component.
Descriptively, imagine S2 as a symphony where the aortic and pulmonary valves are the lead instruments. The aortic valve’s closure is the sharp, crisp note, while the pulmonary valve’s closure adds a softer, more lingering tone. Together, they create a harmonious sound that signifies the end of systole and the transition to diastole. However, when one instrument falls out of tune—perhaps due to stenosis, regurgitation, or hypertension—the entire melody is disrupted. By listening closely to this auditory signature, clinicians can identify discordance early and restore the heart’s rhythm to its natural cadence.
Unveiling the Mystery: Is the Sound Village a Real Place?
You may want to see also
Explore related products






![]()
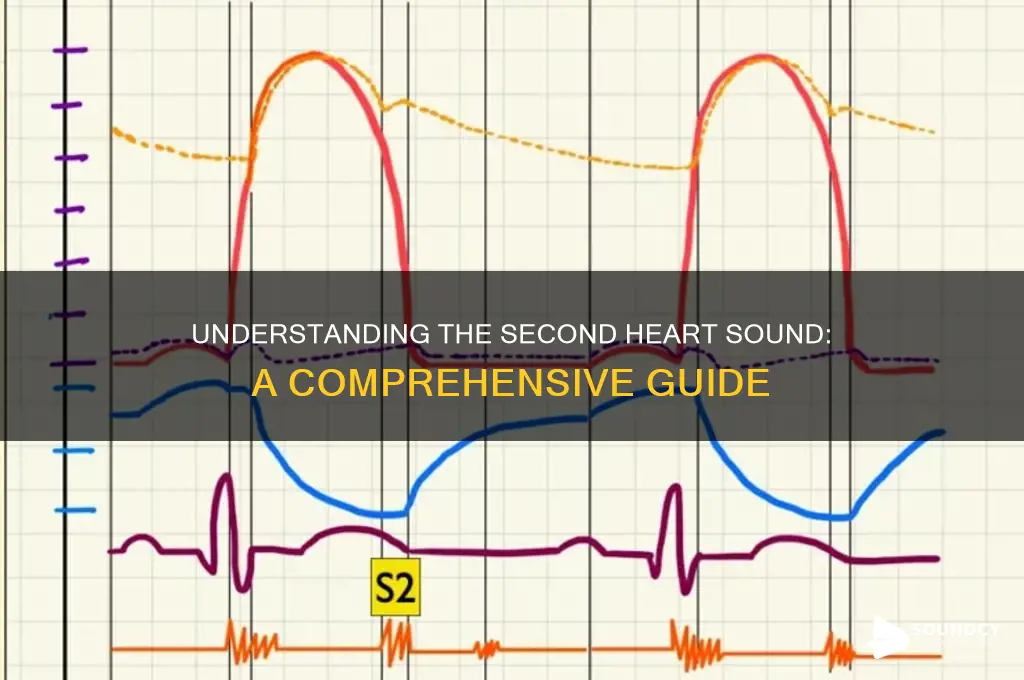
Timing: S2 occurs at the end of ventricular systole, marking its conclusion
The second heart sound (S2) is a critical marker in the cardiac cycle, and its timing is as precise as a Swiss watch. It occurs at the end of ventricular systole, the phase when the heart’s ventricles contract to pump blood into the aorta and pulmonary artery. This moment is not arbitrary; it coincides with the closure of the aortic and pulmonic valves, creating the distinctive "dub" sound audible through a stethoscope. Understanding this timing is essential for clinicians, as deviations can signal valve dysfunction or other cardiac abnormalities. For instance, a widened splitting of S2 may indicate delayed closure of the pulmonic valve, often seen in conditions like pulmonary hypertension.
To appreciate S2’s timing, consider the cardiac cycle as a choreographed dance. Systole begins with the opening of the mitral and tricuspid valves, followed by the forceful ejection of blood during isovolumetric contraction. As systole concludes, blood flow from the ventricles slows, and pressure in the aorta and pulmonary artery exceeds ventricular pressure. This pressure reversal causes the aortic and pulmonic valves to snap shut, generating S2. This sequence is so consistent that even slight alterations in timing—measured in milliseconds—can be clinically significant. For example, a delayed S2 in a young adult might prompt further investigation into left ventricular hypertrophy or aortic stenosis.
Clinicians rely on S2’s timing to differentiate between normal and pathological conditions. In children and young adults, S2 typically splits physiologically during inspiration due to increased blood flow to the lungs. However, a paradoxical splitting (widening during expiration) or a fixed splitting (no change with respiration) can indicate congenital heart defects or chronic lung disease. To assess S2 accurately, place the stethoscope at the second right intercostal space (aortic area) and the third left intercostal space (pulmonic area). Note the intensity, quality, and timing of the sound relative to respiration, as these details provide critical diagnostic clues.
Practical tips for evaluating S2 include ensuring the patient is in a quiet environment to minimize ambient noise and asking them to breathe deeply to accentuate splitting. For pediatric patients, distraction techniques like toys or storytelling can help obtain accurate auscultation. In older adults, where calcification of valves is more common, S2 may be softer or muffled, requiring increased concentration. If S2 is consistently abnormal, consider referring the patient for echocardiography to visualize valve function and structure. Mastering the timing of S2 not only enhances diagnostic accuracy but also reinforces the clinician’s ability to interpret the cardiac cycle as a dynamic, interdependent process.
Mastering the V Sound: Articulatory Techniques and Tongue Placement Explained
You may want to see also
Explore related products






![]()
Characteristics: S2 is typically louder and higher pitched than the first heart sound
The second heart sound (S2) is a distinct auditory marker in the cardiac cycle, often described as the "dub" in the "lub-dub" rhythm. Its characteristic loudness and higher pitch compared to the first heart sound (S1) are not arbitrary; they stem from the abrupt closure of the aortic and pulmonary valves, which occurs under higher pressure and with greater force. This physiological mechanism results in a sharper, more pronounced sound that is easily discernible during auscultation. Clinicians rely on this distinction to assess the timing and integrity of valve function, making S2 a critical component of cardiac evaluation.
To appreciate why S2 is louder and higher pitched, consider the hemodynamics involved. During systole, blood is ejected from the ventricles into the aorta and pulmonary artery, creating significant pressure. When the ventricles finish contracting, this pressure causes the aortic and pulmonary valves to slam shut, producing S2. The rapidity and force of this closure generate a higher frequency sound wave, which the human ear perceives as higher pitched. In contrast, S1, which results from the closure of the mitral and tricuspid valves, occurs under lower pressure and is thus softer and lower in pitch.
Auscultation techniques can enhance the detection of S2’s unique characteristics. Positioning the stethoscope at the second right intercostal space (aortic area) or the third left intercostal space (pulmonic area) optimizes S2’s audibility. For pediatric patients, lighter pressure and a more dynamic approach are necessary, as their heart sounds are higher pitched and softer overall. Adults with hypertension or aortic stenosis may exhibit a widened or split S2, requiring careful differentiation between the aortic and pulmonary components. Mastering these nuances ensures accurate diagnosis and monitoring of cardiac conditions.
The practical implications of S2’s loudness and pitch extend beyond auscultation. In echocardiography, Doppler studies often correlate S2’s intensity with valve function, providing a non-invasive method to assess stenosis or regurgitation. For instance, a paradoxically split S2 in a patient with left bundle branch block indicates delayed aortic valve closure, a critical finding in managing heart failure. Recognizing these patterns allows healthcare providers to tailor interventions, such as adjusting medication dosages or scheduling valve replacement surgeries, based on the specific characteristics of S2.
Finally, understanding S2’s acoustic properties can empower patients to participate in their cardiac care. Encouraging individuals to familiarize themselves with the normal "lub-dub" rhythm enables them to report deviations, such as a softer or muffled S2, which could signal valve dysfunction. Simple self-monitoring techniques, like palpating the carotid pulse while listening to heart sounds, can bridge the gap between clinical visits. By demystifying S2’s unique characteristics, both providers and patients can collaborate more effectively in maintaining cardiovascular health.
Wall of Force: Soundproof Barrier or Sonic Vulnerability?
You may want to see also
Explore related products






![]()
Physiology: Reflects the closure of semilunar valves, separating ventricles from arteries
The second heart sound (S2) is a critical marker in the cardiac cycle, distinct from the first heart sound (S1), which signifies the closure of the atrioventricular valves. S2 occurs during the end of systole and is characterized by the closure of the semilunar valves—specifically, the aortic and pulmonary valves. This event is not merely a mechanical process but a physiological phenomenon that ensures unidirectional blood flow from the ventricles into the arteries, preventing backflow. Understanding this mechanism is essential for clinicians and students alike, as it provides insights into cardiovascular health and disease.
From an analytical perspective, the closure of the semilunar valves is a pressure-dependent event. As the ventricles contract during systole, blood is ejected into the aorta and pulmonary artery, causing pressure in these vessels to rise. When ventricular pressure falls below arterial pressure, the semilunar valves snap shut, producing the audible S2. This sound is split into two components: A2 (closure of the aortic valve) and P2 (closure of the pulmonary valve). The timing and intensity of these components can reveal valuable information about valve function, arterial stiffness, and pulmonary pressures. For instance, a widened splitting of S2 may indicate delayed closure of the pulmonary valve, often seen in conditions like pulmonary hypertension.
Instructively, auscultation of S2 is a fundamental skill in clinical practice. To accurately assess this sound, place the diaphragm of a stethoscope over the second right intercostal space (for A2) and the third left intercostal space (for P2). Listen for the higher-pitched, sharper quality of S2 compared to S1. In children and young adults, P2 is typically louder than A2 due to higher pulmonary artery pressures relative to the aorta. However, with age, A2 becomes more prominent as aortic stiffness increases. Practicing on diverse patient populations, including those with congenital heart defects or valvular diseases, can enhance diagnostic accuracy.
Persuasively, recognizing abnormalities in S2 is crucial for early detection of cardiovascular pathology. For example, a paradoxically split S2, where the normal splitting pattern reverses during inspiration, is a hallmark of left bundle branch block or right ventricular volume overload. Similarly, a single, loud S2 may suggest pulmonary stenosis or severe aortic stenosis. By correlating auscultatory findings with other diagnostic tools like echocardiography, clinicians can formulate targeted treatment plans. Ignoring subtle changes in S2 could lead to missed diagnoses, underscoring the importance of mastering this skill.
Descriptively, the closure of semilunar valves is a symphony of precision and force. Imagine the aortic and pulmonary valves as gates that slam shut with a snap, sealing the ventricles from the arteries. This action is so swift and efficient that it produces a sound audible through the chest wall. The split nature of S2, with A2 preceding P2 in most cases, reflects the slight delay in pulmonary valve closure due to lower resistance in the pulmonary circulation. This physiological split becomes more pronounced during inspiration, as intrathoracic pressure drops, increasing venous return to the right heart and delaying P2 further. Such nuances make S2 a rich source of diagnostic information.
In conclusion, the second heart sound is more than just an auditory cue—it is a window into the dynamic interplay between the heart and its vascular system. By understanding the physiology of semilunar valve closure, clinicians can decode vital information about cardiac function and identify early signs of disease. Whether through analytical interpretation, instructive auscultation, persuasive diagnosis, or descriptive visualization, mastering S2 is indispensable in cardiovascular medicine.
Does Russian Sound Like Portuguese? Unraveling the Linguistic Similarities and Differences
You may want to see also
Explore related products






![]()
Abnormalities: Split, wide, or paradoxical S2 may indicate valve or cardiac issues
The second heart sound (S2) is a critical marker of cardiac health, typically heard as a sharp "dub" during auscultation. It signifies the closure of the aortic and pulmonic valves at the beginning of diastole. However, abnormalities in S2, such as splitting, widening, or paradoxical splitting, can serve as red flags for underlying valve or cardiac issues. Recognizing these variations is essential for early diagnosis and intervention.
Splitting of S2 occurs when the aortic and pulmonic components of the sound separate, creating a distinct double sound. Normally, a slight splitting is heard during inspiration in healthy individuals, especially in children and young adults. However, wide splitting—where the separation is exaggerated and persists throughout the respiratory cycle—may indicate right bundle branch block or pulmonary hypertension. Clinicians should note that wide splitting during expiration specifically points to conditions like atrial septal defect, where blood flow dynamics alter valve closure timing.
Paradoxical splitting of S2 is a more concerning finding, where the normal inspiratory splitting reverses, becoming more pronounced during expiration. This abnormality is strongly associated with left bundle branch block or severe left ventricular dysfunction. For instance, in patients with advanced heart failure, the delayed closure of the aortic valve relative to the pulmonic valve causes this reversal. Early detection of paradoxical splitting can prompt further diagnostic tests, such as echocardiography, to assess cardiac function and valve integrity.
When evaluating S2 abnormalities, context matters. Age, respiratory status, and comorbidities influence interpretation. For example, a split S2 in a young athlete may be benign, while the same finding in an elderly patient with dyspnea warrants investigation for pulmonary hypertension. Practitioners should also consider positional changes; having the patient shift from supine to standing can help differentiate physiological from pathological splitting.
In summary, abnormalities in the second heart sound—split, wide, or paradoxical—are not mere auscultatory curiosities but potential indicators of significant cardiac pathology. Mastery of these nuances enables healthcare providers to triage patients effectively, ensuring timely referrals and interventions. Regular auscultation, coupled with a systematic approach to interpreting S2 variations, remains a cornerstone of cardiovascular assessment.
Understanding the MF Sound: Definition, Origins, and Modern Applications
You may want to see also
Frequently asked questions
The second heart sound (S2) is one of the heart sounds heard during auscultation, produced by the closure of the aortic and pulmonic valves at the beginning of diastole.
The second heart sound is caused by the abrupt closure of the aortic and pulmonic valves, which prevents backflow of blood into the ventricles as they begin to relax.
The second heart sound (S2) is higher pitched and shorter in duration compared to the first heart sound (S1), which is produced by the closure of the mitral and tricuspid valves at the start of systole.
A split second heart sound (S2) occurs when the aortic and pulmonic valve closures are not simultaneous, often heard as two distinct components. This can be normal in inspiration or indicate underlying conditions like left bundle branch block or pulmonary hypertension.
Yes, an abnormal second heart sound (S2) can indicate issues such as valve dysfunction (e.g., aortic stenosis or pulmonic regurgitation), hypertension, or other cardiovascular conditions, depending on the specific changes in its quality or timing.