The S1 heart sound, often described as the lub in the familiar lub-dub rhythm, is the first of the two primary heart sounds heard during a cardiac cycle. It occurs at the beginning of systole, the phase when the heart contracts to pump blood, and is produced by the closure of the atrioventricular (AV) valves—the mitral valve on the left side and the tricuspid valve on the right side of the heart. This sound signifies the transition from diastole to systole and is crucial for assessing cardiac function, as its characteristics, such as intensity, pitch, and splitting, can provide valuable insights into the health of the heart valves and overall cardiovascular system.
| Characteristics | Values |
|---|---|
| Definition | The first heart sound, produced by the closure of the atrioventricular (AV) valves (mitral and tricuspid) at the beginning of ventricular contraction (systole). |
| Timing | Occurs at the start of systole, following the P wave and QRS complex on ECG. |
| Pitch | Low-pitched, often described as a "lub" sound. |
| Duration | Typically lasts 0.1-0.12 seconds. |
| Intensity | Louder than S2 (second heart sound) in most cases. |
| Physiology | Marks the beginning of ventricular contraction and the end of diastolic filling. |
| Associated Valves | Mitral (left AV valve) and tricuspid (right AV valve) closure. |
| Clinical Significance | Abnormalities in S1 (e.g., splitting, muffling, or loudness changes) can indicate valve disorders, bundle branch blocks, or other cardiac conditions. |
| Auscultation Location | Best heard at the mitral (apex) and tricuspid (left lower sternal border) areas. |
| ECG Correlation | Corresponds to the onset of the ventricular contraction, visible as the QRS complex. |
Explore related products






What You'll Learn
- Definition: S1 is the first heart sound, caused by AV valves closing
- Mechanism: AV valves shut as ventricles contract, creating low-pitched lub sound
- Timing: Occurs at the start of ventricular systole, marking contraction onset
- Characteristics: Dull, longer duration compared to S2, heard best at mitral area
- Clinical Significance: Abnormal S1 may indicate valve disorders or myocardial issues
![]()
Definition: S1 is the first heart sound, caused by AV valves closing
The first heart sound, denoted as S1, is a fundamental component of the cardiac cycle and plays a crucial role in assessing heart function. Definition: S1 is the first heart sound, caused by AV valves closing. This sound occurs at the beginning of systole, the phase when the heart contracts to pump blood. Specifically, S1 is produced when the atrioventricular (AV) valves—the mitral valve on the left side and the tricuspid valve on the right side—close abruptly. This closure prevents blood from flowing back into the atria as the ventricles begin to contract. The AV valves close due to the sudden increase in pressure within the ventricles, which exceeds the atrial pressure, causing the leaflets of the valves to come together and produce the characteristic sound.
The mechanism behind S1 involves the rapid deceleration of blood flow and the subsequent vibration of the valve leaflets and surrounding structures. When the ventricles contract, the pressure inside them rises sharply, forcing the AV valves to shut tightly. This abrupt closure creates turbulence in the blood flow, generating low-frequency vibrations that are audible through a stethoscope. Clinicians often describe S1 as a "lub" sound, which is typically lower in pitch compared to the second heart sound (S2). The quality, intensity, and timing of S1 provide valuable insights into the integrity and function of the AV valves and the overall cardiac performance.
Understanding the definition of S1—that it is the first heart sound caused by AV valves closing—is essential for auscultation, the process of listening to heart sounds. During auscultation, healthcare professionals place a stethoscope on specific areas of the chest to detect S1 and other heart sounds. S1 is best heard at the mitral and tricuspid areas, which correspond to the anatomical positions of the AV valves. The sound is typically loudest and most distinct in these regions, allowing clinicians to evaluate valve function and identify abnormalities such as stenosis (narrowing) or regurgitation (leakage).
The timing of S1 within the cardiac cycle is another critical aspect of its definition. It marks the transition from diastole (relaxation) to systole (contraction). Electrocardiogram (ECG) readings often accompany auscultation to correlate S1 with the electrical activity of the heart. On an ECG, S1 aligns with the R wave, which represents ventricular depolarization and the onset of contraction. This synchronization between the electrical and mechanical events of the heart reinforces the understanding that S1 is directly linked to the closure of the AV valves.
In summary, Definition: S1 is the first heart sound, caused by AV valves closing, and it is a key indicator of cardiac health. This sound is generated by the abrupt closure of the mitral and tricuspid valves at the start of ventricular contraction, preventing backflow of blood into the atria. Its characteristics, including pitch, intensity, and timing, offer important diagnostic information. By mastering the definition and significance of S1, healthcare providers can effectively assess heart function and detect potential valve disorders through auscultation and related diagnostic techniques.
Is Sound Deadening Worth It? Pros, Cons, and Real-World Benefits
You may want to see also
Explore related products






![]()
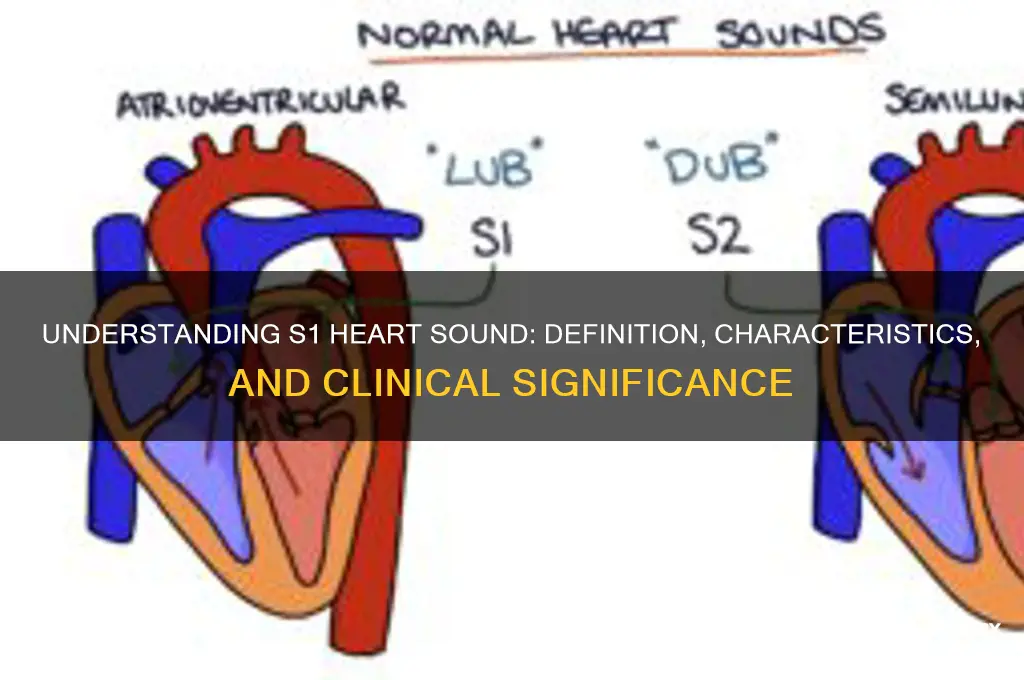
Mechanism: AV valves shut as ventricles contract, creating low-pitched lub sound
The first heart sound, often referred to as S1, is a fundamental component of the cardiac cycle and is primarily associated with the closure of the atrioventricular (AV) valves. This sound is a direct result of the intricate mechanism that occurs during the initial phase of ventricular contraction. As the ventricles begin to contract, a crucial event takes place: the AV valves, consisting of the tricuspid and mitral valves, rapidly shut to prevent the backflow of blood into the atria. This closure is not silent; instead, it generates a distinct auditory phenomenon.
The mechanism behind the S1 sound is a fascinating interplay of cardiac structures. When the ventricles contract, the pressure within these chambers rises rapidly. This increase in pressure causes the AV valves to snap shut, a process that is both swift and powerful. The closure is so abrupt that it creates a vibration within the valve leaflets and the surrounding structures, including the chordae tendineae and papillary muscles. These vibrations are transmitted through the bloodstream and the walls of the heart, ultimately reaching the chest wall, where they can be heard as a sound.
The quality of the S1 sound is characteristic and easily distinguishable. It is typically described as a low-pitched, dull, or muffled sound, often likened to the word "lub." This distinct pitch is a result of the frequency of the vibrations produced during valve closure. The lower frequency is due to the larger mass of the AV valves compared to the semilunar valves, which produce the second heart sound (S2). The "lub" sound of S1 is usually longer in duration than the S2 sound, reflecting the more substantial movement and greater tissue involvement in the AV valve closure.
This heart sound is a critical indicator of the heart's function and timing. It marks the beginning of systole, the phase of the cardiac cycle when the ventricles contract to pump blood. The S1 sound ensures that blood flows in the correct direction, from the atria to the ventricles and then out to the body and lungs. Any abnormalities in the timing or quality of S1 can provide valuable insights into potential cardiac issues, such as valve disorders or problems with ventricular contraction.
In summary, the S1 heart sound is a low-pitched auditory signal generated by the rapid closure of the AV valves at the onset of ventricular contraction. This mechanism is essential for maintaining proper blood flow direction and is a key indicator of the heart's rhythmic performance. Understanding this process is fundamental in cardiology, as it provides a window into the heart's intricate workings and helps in the diagnosis and assessment of various cardiac conditions.
Breath Sounds: Ventilator Use and Normalcy
You may want to see also
Explore related products






![]()
Timing: Occurs at the start of ventricular systole, marking contraction onset
The S1 heart sound is a critical component of the cardiac cycle, and its timing is intimately tied to the onset of ventricular systole. This sound occurs precisely at the beginning of ventricular contraction, marking the moment when the ventricles start to pump oxygenated blood out of the heart. The timing of S1 is a direct consequence of the closure of the atrioventricular (AV) valves, specifically the mitral and tricuspid valves. As the ventricles begin to contract, pressure in these chambers rises, causing the AV valves to snap shut, which produces the audible S1 sound. This event is a clear indicator that the heart has transitioned from diastole to systole, emphasizing the importance of S1 in cardiac auscultation.
Understanding the timing of S1 is essential for clinicians to correlate heart sounds with the underlying physiological processes. The onset of S1 coincides with the electrical signal from the ventricles, known as the QRS complex on an electrocardiogram (ECG). This synchronization between the ECG and heart sounds allows healthcare providers to assess the mechanical function of the heart in relation to its electrical activity. For instance, any delay or abnormality in the timing of S1 can suggest issues with valve function, myocardial contractility, or conduction abnormalities, making it a valuable diagnostic tool.
The precise timing of S1 also highlights its role in the cardiac cycle's efficiency. By occurring at the exact start of ventricular systole, S1 ensures that the atria are no longer contributing blood to the ventricles, preventing backflow. This timing is crucial for maintaining optimal cardiac output, as it allows the ventricles to eject blood effectively into the aorta and pulmonary artery. Any deviation in the timing of S1, such as a split sound, can indicate conditions like bundle branch block or valve disorders, where the synchronization between valve closure and ventricular contraction is disrupted.
Clinically, the timing of S1 serves as a reference point for identifying other heart sounds and murmurs. For example, the interval between S1 and the subsequent S2 sound (marking the end of systole) provides insights into the duration of ventricular contraction and relaxation. By focusing on the timing of S1, healthcare professionals can better evaluate the overall rhythm and function of the heart. This makes the S1 sound not just a marker of ventricular contraction onset but also a foundational element in the comprehensive assessment of cardiac health.
In summary, the timing of the S1 heart sound is a precise and functionally significant event in the cardiac cycle. Occurring at the start of ventricular systole, it marks the onset of contraction and the closure of the AV valves. This timing is crucial for maintaining cardiac efficiency, serves as a diagnostic reference point, and is closely linked to the heart's electrical activity. By understanding and accurately identifying the timing of S1, clinicians can gain valuable insights into the heart's mechanical and electrical integrity, making it an indispensable aspect of cardiovascular evaluation.
Dongle Dilemma: Android Compatibility Explored
You may want to see also
Explore related products






![]()
Characteristics: Dull, longer duration compared to S2, heard best at mitral area
The S1 heart sound is one of the fundamental components of the cardiac cycle, representing the closure of the atrioventricular (AV) valves—the mitral and tricuspid valves. When discussing its characteristics, particularly dullness, longer duration compared to S2, and being heard best at the mitral area, it is essential to understand the underlying physiology and auscultatory nuances. The dull quality of S1 contrasts with the sharper, higher-pitched nature of S2, which is associated with the closure of the semilunar valves (aortic and pulmonary). This dullness is attributed to the lower frequency of S1, typically ranging between 20 to 60 Hz, as the AV valves close more slowly and with less force compared to the semilunar valves. This characteristic makes S1 feel less crisp and more muted to the listener.
The longer duration of S1 compared to S2 is another key feature. While S2 is brief and snaps quickly, S1 persists slightly longer, often lasting 100 to 150 milliseconds. This prolonged duration is due to the sequential closure of the mitral valve (slightly earlier) followed by the tricuspid valve. The mitral component of S1 is typically louder and dominates the sound, especially when auscultated at the mitral area, which is located at the fifth intercostal space in the midclavicular line. The tricuspid component, being softer and lower in pitch, is often overshadowed but contributes to the overall duration of S1.
The mitral area is indeed the optimal location for hearing S1 most clearly. This is because the mitral valve’s closure generates a louder sound due to the higher pressure and volume of blood in the left ventricle compared to the right ventricle. When the stethoscope is placed at the mitral area, the dull, sustained quality of S1 is most pronounced. Clinicians often instruct students to focus on this area to distinguish S1 from other sounds, as its characteristics are most evident here. The dullness and longer duration become more apparent when compared to the sharper, shorter S2 heard at the aortic or pulmonary areas.
It is important to note that the dullness and duration of S1 can vary in certain pathological conditions. For example, in mitral stenosis, S1 may become louder and more prominent due to increased resistance during valve closure. Conversely, in mitral regurgitation, S1 may be softer or less distinct. Understanding these normal characteristics is crucial for identifying abnormalities during auscultation. The longer duration of S1, when compared to the abrupt S2, serves as a reliable marker for differentiating the two sounds, especially in patients with rapid heart rates where the cardiac cycle is compressed.
In summary, the S1 heart sound is characterized by its dull quality, longer duration compared to S2, and optimal audibility at the mitral area. These features are rooted in the physiology of AV valve closure and the hemodynamics of the left ventricle. Mastery of these characteristics is essential for accurate cardiac auscultation and diagnosis, as deviations from the norm can indicate underlying cardiac pathology. By focusing on the mitral area and comparing S1 to S2, clinicians can effectively assess the integrity of the AV valves and the overall cardiac function.
How Catalytic Converters Affect Your Car's Sound
You may want to see also
Explore related products






![]()
Clinical Significance: Abnormal S1 may indicate valve disorders or myocardial issues
The first heart sound, S1, is a crucial component of the cardiac cycle, marking the beginning of systole and resulting from the closure of the atrioventricular (AV) valves—the mitral and tricuspid valves. Normally, S1 is heard as a single, crisp sound, often described as "lub," and is best auscultated at the mitral and tricuspid areas of the chest. Clinically, an abnormal S1 can serve as an early indicator of underlying cardiovascular pathology, particularly valve disorders or myocardial issues. When S1 is muffled, split, or absent, it may suggest dysfunction in the AV valves, such as stenosis or regurgitation. For instance, a softened S1 can occur in mitral stenosis due to restricted valve movement, while a split S1 may indicate conduction abnormalities or right bundle branch block, which affects the synchronous closure of the AV valves.
Valve disorders are a primary concern when evaluating an abnormal S1. Mitral valve prolapse, for example, can cause a clicking sound followed by a murmur, often associated with a prominent S1. Conversely, severe mitral regurgitation may lead to a diminished S1 due to incomplete valve closure. Similarly, tricuspid valve abnormalities, such as tricuspid regurgitation, can alter the intensity or quality of S1. Clinicians must correlate these findings with other diagnostic tools, such as echocardiography, to confirm valve pathology and determine appropriate management. Early detection of valve disorders through auscultation of S1 is critical, as untreated conditions can lead to heart failure, arrhythmias, or other complications.
Myocardial issues can also manifest as abnormalities in S1. In conditions like myocardial infarction or cardiomyopathy, the heart muscle may weaken, leading to poor valve coaptation and a resultant change in S1 quality. For instance, a muffled S1 may be heard in dilated cardiomyopathy due to enlarged ventricular dimensions and reduced contractility. Additionally, ischemia or infarction affecting the papillary muscles can impair valve function, altering the S1 sound. These myocardial abnormalities often require urgent intervention, as they can progress to severe heart failure or life-threatening arrhythmias if left untreated.
The clinical significance of an abnormal S1 extends to its role in diagnosing specific syndromes or conditions. For example, a split S1 is commonly associated with right bundle branch block, where the delay in right ventricular contraction causes the tricuspid valve to close after the mitral valve. This finding, when combined with other clinical data, can guide further electrophysiological evaluation. Similarly, a widely split S1 may indicate complete heart block, a serious condition requiring immediate attention. Recognizing these patterns allows clinicians to initiate timely diagnostic workups and interventions.
In summary, an abnormal S1 is a critical finding that warrants thorough investigation, as it may signal valve disorders, myocardial issues, or other significant cardiovascular conditions. Clinicians must remain vigilant during auscultation, correlating findings with patient history, physical examination, and diagnostic studies to ensure accurate diagnosis and management. Early recognition of S1 abnormalities can lead to better outcomes by enabling prompt treatment of underlying pathologies, thereby preventing disease progression and improving patient prognosis.
Exploring 8mm Film: Did This Vintage Medium Capture Sound?
You may want to see also
Frequently asked questions
S1 heart sound is the first heart sound, which is produced by the closure of the mitral and tricuspid valves at the beginning of ventricular contraction (systole).
The S1 heart sound is caused by the sudden increase in pressure within the ventricles, which forces the mitral and tricuspid valves to close, creating a low-pitched, dull sound.
S1 heart sound differs from S2 heart sound in that S1 occurs at the beginning of ventricular contraction, while S2 occurs at the beginning of ventricular relaxation (diastole) and is produced by the closure of the aortic and pulmonary valves.
An abnormal S1 heart sound, such as a muffled or absent sound, can indicate underlying heart conditions like mitral stenosis, left bundle branch block, or heart failure, and may require further evaluation by a healthcare professional.