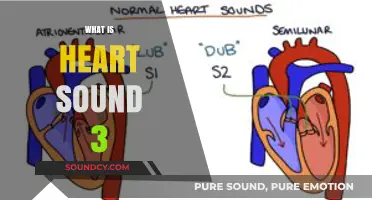
Heart sound physiology is the study of the acoustic phenomena produced by the heart during its normal functioning, primarily resulting from the closing and opening of the heart valves, as well as the movement of blood through the cardiac chambers. These sounds, typically heard as lub-dub through a stethoscope, correspond to the closing of the atrioventricular (mitral and tricuspid) valves and the semilunar (aortic and pulmonary) valves, respectively. Understanding heart sound physiology is crucial for diagnosing cardiovascular conditions, as abnormalities in these sounds can indicate valve dysfunction, structural defects, or other cardiac pathologies. The field integrates principles of physics, anatomy, and physiology to explain how mechanical events within the heart translate into audible signals, providing valuable insights into cardiac health and disease.
Explore related products






What You'll Learn
- Heart Sound Origins: Vibrations from blood flow and heart structures create audible sounds during cardiac cycles
- First Heart Sound (S1): Mitral and tricuspid valves close, marking ventricular systole start
- Second Heart Sound (S2): Aortic and pulmonic valves close, signaling systole end
- Murmurs and Abnormalities: Unusual sounds indicate valve issues, defects, or blood flow problems
- Heart Sound Timing: Linked to ECG waves, helps diagnose cardiac rhythm and function
![]()
Heart Sound Origins: Vibrations from blood flow and heart structures create audible sounds during cardiac cycles
The human heart, a marvel of biological engineering, produces a symphony of sounds with each beat, a phenomenon rooted in the intricate interplay of blood flow and cardiac structures. These heart sounds, often described as "lub-dub," are not mere auditory curiosities but vital indicators of cardiovascular health. The first heart sound (S1), resembling the "lub," occurs when the atrioventricular valves (mitral and tricuspid) close, marking the beginning of systole. This closure is abrupt, creating vibrations as blood flow is halted, much like the sudden stop of a stringed instrument. The second heart sound (S2), the "dub," follows when the semilunar valves (aortic and pulmonary) close at the end of systole, initiating diastole. These sounds are the audible manifestations of the heart’s mechanical efficiency, each vibration a testament to the precision of cardiac function.
To understand the origins of these sounds, consider the physics of fluid dynamics and structural interaction. Blood flowing through the heart encounters resistance at valve closures, generating turbulence that propagates through cardiac tissues. The mitral valve, for instance, closes with greater force than the tricuspid, contributing to the louder component of S1. Similarly, the aortic valve’s closure produces a higher-pitched sound in S2 compared to the pulmonary valve. These variations are not random; they reflect the unique pressures and velocities of blood in different cardiac chambers. Clinicians use stethoscopes to amplify these sounds, distinguishing normal rhythms from pathological murmurs caused by valve defects or structural abnormalities.
Practical application of this knowledge is critical in medical diagnostics. For example, a split S2, where the aortic and pulmonary components are distinctly audible, is normal in children but may indicate left ventricular volume overload in adults. Murmurs, which are additional sounds caused by turbulent blood flow, can signify conditions like mitral stenosis or aortic regurgitation. Auscultation, the act of listening to heart sounds, requires a systematic approach: position the patient in a supine or left lateral decubitus position, use the bell or diaphragm of the stethoscope appropriately, and correlate findings with the cardiac cycle. Mastering this skill enables healthcare providers to detect early signs of heart disease, often before symptoms manifest.
Comparatively, heart sounds offer a non-invasive window into cardiac function, rivaling imaging modalities in certain contexts. While echocardiography provides visual detail, auscultation remains a cost-effective, bedside tool accessible in resource-limited settings. Advances in digital stethoscopes and AI-driven analysis further enhance accuracy, allowing for real-time interpretation of heart sounds. For instance, machine learning algorithms can differentiate innocent murmurs from pathological ones with high precision, reducing unnecessary referrals. This blend of traditional and modern techniques underscores the enduring relevance of heart sound physiology in clinical practice.
In conclusion, the origins of heart sounds lie in the vibrations generated by blood flow and cardiac structures during the cardiac cycle. These sounds are not merely auditory phenomena but critical diagnostic tools that reveal the heart’s mechanical state. By understanding their physiology, healthcare providers can detect abnormalities early, guiding timely interventions. Whether through the classic stethoscope or cutting-edge technology, the study of heart sounds remains a cornerstone of cardiology, bridging the gap between physics and clinical medicine.
Unveiling the Origins: Exploring the Science Behind Sound Creation
You may want to see also
Explore related products





![]()
First Heart Sound (S1): Mitral and tricuspid valves close, marking ventricular systole start
The first heart sound, often abbreviated as S1, is a critical auditory marker in cardiovascular physiology, signaling the beginning of ventricular systole. This sound occurs when the mitral and tricuspid valves close, preventing blood from flowing back into the atria as the ventricles contract. Clinicians rely on S1 to assess cardiac function, as its timing, intensity, and quality provide insights into valve integrity and ventricular performance. For instance, a loud S1 may suggest volume overload in the left ventricle, while a soft or muffled sound could indicate valve dysfunction or hypovolemia. Understanding S1 is essential for diagnosing conditions like mitral stenosis or tricuspid regurgitation, making it a cornerstone of auscultatory practice.
To identify S1 effectively, healthcare providers use a systematic approach during auscultation. Positioning the diaphragm of the stethoscope over the mitral (fifth left intercostal space, midclavicular line) and tricuspid (left lower sternal border) areas allows for clear detection. S1 typically coincides with the carotid pulse, providing a tactile reference point. Patients should be in a supine or left lateral decubitus position to optimize sound transmission. For pediatric patients, particularly those under 12 years old, a higher-pitched S1 is normal due to faster heart rates and smaller valve structures. Practicing auscultation on diverse patient populations enhances the ability to distinguish normal variations from pathological changes.
Comparatively, S1 differs from the second heart sound (S2) in both timing and origin. While S1 marks the start of systole with mitral and tricuspid closure, S2 signifies the end of systole when the aortic and pulmonic valves close. This distinction is crucial for differentiating between systolic and diastolic events. For example, a widened split between S1 and S2 in inspiration suggests right bundle branch block, whereas a paradoxical split may indicate left bundle branch block. Recognizing these patterns requires not only auditory acuity but also an understanding of the underlying hemodynamics, reinforcing the importance of S1 in the diagnostic process.
From a practical standpoint, teaching S1 auscultation involves breaking down the process into manageable steps. Begin by explaining the physiological basis of the sound, emphasizing the role of valve closure. Next, demonstrate proper stethoscope placement and technique, ensuring students correlate S1 with the carotid pulse. Caution against common errors, such as confusing S1 with lung sounds or overlooking positional adjustments. Finally, encourage learners to practice on both healthy individuals and patients with known cardiac conditions to build confidence and competence. Mastering S1 auscultation not only enhances diagnostic skills but also fosters a deeper appreciation for the intricacies of heart sound physiology.
Explore Degrees in Sound Engineering: Programs and Career Paths
You may want to see also
Explore related products






![]()
Second Heart Sound (S2): Aortic and pulmonic valves close, signaling systole end
The second heart sound (S2) is a critical marker in cardiac auscultation, representing the closure of the aortic and pulmonic valves at the end of systole. This sound is often described as a sharp, high-pitched "dub" and is best heard at the base of the heart. Clinicians rely on S2 to assess the timing and efficiency of ventricular ejection, as it signifies the transition from systole to diastole. Understanding its characteristics—such as intensity, splitting, and timing—provides valuable insights into cardiovascular function and potential pathologies.
Analyzing S2 reveals its dynamic nature, particularly in the context of respiratory influence. During inspiration, the pulmonic valve closure component of S2 is delayed due to increased intrathoracic pressure, causing a physiological splitting of the sound. Conversely, expiration narrows the split or makes S2 appear single. This respiratory variation is normal and aids in distinguishing it from pathological conditions like a wide, fixed split, which may indicate a ventricular septal defect or right bundle branch block. Recognizing these nuances is essential for accurate diagnosis and patient management.
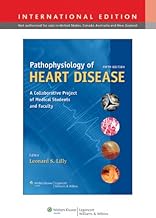
From a practical standpoint, auscultating S2 requires precise technique. Use the diaphragm of the stethoscope for higher-frequency sounds and place it at the second right intercostal space (aortic area) or the third left intercostal space (pulmonic area). Encourage the patient to breathe deeply to observe respiratory changes in S2 splitting. Document the sound’s quality, duration, and relationship to respiration, as these details can differentiate normal physiology from abnormalities like aortic stenosis or pulmonic regurgitation.
Comparatively, S2 stands apart from the first heart sound (S1) in both timing and tone. While S1 marks the closure of the mitral and tricuspid valves at the start of systole, S2 signals its conclusion. The higher pitch of S2, compared to the lower-pitched "lub" of S1, allows for clear differentiation. This contrast underscores the importance of sequential valve closure in maintaining unidirectional blood flow and highlights how disruptions in S2 can indicate significant cardiac issues, such as valve dysfunction or increased afterload.
In conclusion, the second heart sound is more than just an auditory event; it is a window into the heart’s mechanical performance. By mastering its physiology and auscultation techniques, healthcare providers can detect early signs of cardiovascular disease and tailor interventions accordingly. Whether in a routine checkup or critical care setting, S2 remains an indispensable tool in the clinician’s diagnostic arsenal.
Black Hole Sound: Myth or Reality?
You may want to see also
Explore related products






![]()
Murmurs and Abnormalities: Unusual sounds indicate valve issues, defects, or blood flow problems
The human heart, a four-chambered muscular pump, produces distinct sounds—often described as "lub-dub"—that correspond to the closing of its valves. These sounds, known as S1 and S2, are crucial indicators of cardiac function. However, when unusual sounds, such as murmurs, arise, they often signal underlying issues like valve dysfunction, congenital defects, or abnormal blood flow. Murmurs are whooshing or swishing noises that occur between the heart’s normal sounds, graded on a scale of 1 to 6 based on their intensity. For instance, a grade 3 murmur is moderately loud and audible with minimal effort, while a grade 6 murmur is so intense it can be felt as a thrill. Understanding these abnormalities is essential for early diagnosis and intervention, as they can reflect conditions ranging from benign to life-threatening.
To identify murmurs, healthcare providers use a stethoscope to listen for timing, pitch, and location. Systolic murmurs occur during heart contraction, while diastolic murmurs happen during relaxation. For example, a systolic murmur heard best at the left sternal border may indicate aortic stenosis, a condition where the aortic valve narrows, obstructing blood flow. Conversely, a diastolic murmur at the apex could suggest mitral regurgitation, where blood leaks backward through the mitral valve. Age is a critical factor in interpretation; innocent murmurs are common in children and often resolve without treatment, whereas new or changing murmurs in adults warrant further investigation. Echocardiograms and Doppler studies are frequently employed to visualize valve structure and blood flow patterns, providing a definitive diagnosis.
Abnormal heart sounds are not limited to murmurs. Extra sounds, such as S3 or S4, can indicate heart failure or hypertrophy. An S3, often described as a "ventricular gallop," is a low-pitched sound heard in early diastole and may signify volume overload. An S4, a presystolic sound, suggests stiffened ventricles, commonly seen in hypertension or left ventricular hypertrophy. These additional sounds, combined with murmurs, create a symphony of clues for clinicians. For instance, a patient with an S3 and a grade 4 holosystolic murmur at the apex is likely experiencing severe mitral regurgitation with resultant heart failure. Early recognition of these patterns can guide treatment, from medication to surgical valve repair or replacement.
Practical tips for patients include monitoring symptoms like shortness of breath, chest pain, or fatigue, which often accompany significant murmurs or abnormalities. Regular check-ups are vital, especially for those with risk factors such as hypertension, diabetes, or a family history of heart disease. For healthcare providers, auscultation skills remain paramount, but integrating technology like handheld ultrasound devices can enhance diagnostic accuracy. Education is key; teaching patients about their heart sounds empowers them to advocate for their health. For example, a patient aware of a new murmur can promptly seek evaluation, potentially preventing complications like arrhythmias or heart failure.
In conclusion, murmurs and abnormalities in heart sounds are critical markers of cardiac health. Their detection requires a blend of clinical acumen and technological tools, with age, symptoms, and risk factors guiding interpretation. By understanding these unusual sounds, both patients and providers can take proactive steps to address underlying issues, ensuring optimal heart function and overall well-being. Whether through routine auscultation or advanced imaging, the goal remains the same: to decode the heart’s unique language and respond effectively to its silent cries for help.
Exploring Binuaral Eating Sounds: A Sensory ASMR Experience
You may want to see also
Explore related products






![]()
Heart Sound Timing: Linked to ECG waves, helps diagnose cardiac rhythm and function
Heart sounds, those rhythmic lub-dubs, are more than just auditory cues—they are precise markers of cardiac function, each tied to specific phases of the heart’s electrical and mechanical activity. The first heart sound (S1) corresponds to the closure of the mitral and tricuspid valves at the start of systole, while the second heart sound (S2) aligns with the closure of the aortic and pulmonary valves at the beginning of diastole. When synchronized with the ECG, these sounds reveal critical insights: S1 typically coincides with the R wave on the ECG, marking ventricular depolarization and contraction, while S2 aligns with the T wave, reflecting ventricular repolarization and relaxation. This timing is not arbitrary—it’s a diagnostic goldmine.
Consider this practical application: In a patient with suspected mitral valve regurgitation, an ECG-phonocardiogram (PCG) overlay can pinpoint abnormal delays or splits in S1 or S2. For instance, a widened split of S2 in a lead II ECG trace may suggest right bundle branch block, where the aortic valve closes earlier than the pulmonary valve. Clinicians can use this linkage to differentiate between innocent murmurs and pathological conditions, such as aortic stenosis, where S2 may be paradoxically split or delayed. For adults over 65, this approach is particularly valuable, as age-related changes in heart sounds can mimic disease states.
To leverage this diagnostic tool effectively, follow these steps: First, ensure simultaneous ECG and PCG recordings for accurate timing correlation. Second, identify the R wave peak as the anchor point for S1 and observe the T wave for S2 alignment. Third, note any discrepancies, such as a displaced S1 or a delayed S2, which could indicate conduction abnormalities or valvular dysfunction. Caution: Ambient noise and poor electrode placement can distort results, so use high-quality equipment and ensure patient cooperation. For pediatric cases, adjust expectations, as heart rates above 100 bpm may compress the timing intervals, requiring careful interpretation.
The persuasive case for integrating heart sound timing with ECG analysis lies in its simplicity and immediacy. Unlike advanced imaging, this method is non-invasive, cost-effective, and provides real-time data. For instance, in emergency settings, a widened or reversed split of S2 on ECG can rapidly flag left ventricular dysfunction, guiding immediate interventions like diuretics or inotropes. Studies show that combining ECG and PCG improves diagnostic accuracy by up to 30% in cases of arrhythmias and valvular disease. This synergy transforms two standalone tools into a powerful diagnostic duo.
Finally, the comparative advantage of this approach becomes clear when juxtaposed with isolated ECG or auscultation. While ECG alone may miss mechanical abnormalities like mitral prolapse, auscultation without timing context can lead to misinterpretation. Together, they offer a holistic view of cardiac rhythm and function. For example, a patient with a third heart sound (S3) gallop, indicative of heart failure, can be cross-verified with ST-segment changes on ECG, strengthening the diagnosis. This integrated strategy is not just theoretical—it’s a practical, actionable framework for clinicians to enhance patient care.
Exploring the Unique and Vibrant Sounds of Parrots in Nature
You may want to see also
Frequently asked questions
Heart sounds are the noises generated by the beating heart and the resultant flow of blood through it. They are typically described as "lub-dub" sounds, which correspond to the closing of the heart valves.
There are primarily four heart sounds, denoted as S1, S2, S3, and S4. S1 and S2 are the most prominent and are heard in every heartbeat, while S3 and S4 are softer and may not be present in all individuals.
The "lub" sound (S1) is caused by the closure of the atrioventricular (AV) valves – the mitral and tricuspid valves – at the beginning of ventricular contraction. The "dub" sound (S2) is caused by the closure of the semilunar (SL) valves – the aortic and pulmonary valves – at the beginning of ventricular relaxation.
Heart sounds provide valuable information about the functioning of the heart valves, chambers, and overall cardiac performance. Abnormalities in heart sounds, such as murmurs, extra sounds, or split sounds, can indicate underlying cardiovascular conditions like valvular heart disease, congestive heart failure, or hypertension.
Yes, heart sounds can be influenced by various factors, including age, body position, respiratory rate, and emotional state. For example, children and young adults may have louder and higher-pitched heart sounds, while elderly individuals may exhibit softer and lower-pitched sounds. Additionally, heart sounds can be affected by conditions like fever, anemia, or hyperthyroidism.