Aortic stenosis is a serious heart condition characterized by the narrowing of the aortic valve, which restricts blood flow from the heart to the rest of the body. One of the hallmark signs of this condition is a distinct heart sound, often described as a harsh, crescendo-decrescendo murmur, typically heard best at the right second intercostal space. This sound occurs during systole, the phase when the heart contracts, and is caused by turbulent blood flow through the narrowed valve. Recognizing this unique sound is crucial for healthcare professionals, as it serves as a key diagnostic indicator of aortic stenosis, prompting further evaluation and timely intervention to prevent complications such as heart failure or sudden cardiac arrest.
| Characteristics | Values |
|---|---|
| Type of Sound | Systolic murmur |
| Timing | Late-peaking (crescendo-decrescendo) |
| Location | Best heard at the right second intercostal space (aortic area) with radiation to the carotids |
| Intensity | Often harsh, loud (grade 3-6/6) |
| Duration | Short to medium (follows the systolic ejection period) |
| Associated Findings | S2 may be diminished or absent (due to severe stenosis), thrill palpable in severe cases |
| Causes | Calcific (most common in adults), congenital bicuspid aortic valve, rheumatic fever (rare) |
| Pathophysiology | Obstruction of blood flow from the left ventricle to the aorta due to narrowed valve area |
| Diagnostic Tools | Echocardiography (gold standard), Doppler ultrasound, chest X-ray (may show calcification) |
| Clinical Significance | Indicates severe AS if symptomatic (angina, syncope, heart failure) or if valve area <1.0 cm² |
Explore related products






What You'll Learn
![]()
Causes of Aortic Stenosis Sound
Aortic stenosis produces a distinctive sound, a crescendo-decrescendo murmur, often likened to the rumble of a steam engine. This sound is a critical diagnostic clue, but understanding its origins requires delving into the underlying causes of the condition. At its core, aortic stenosis is a narrowing of the aortic valve, the gateway between the heart and the aorta. This obstruction disrupts blood flow, creating turbulence that manifests as the characteristic murmur.
Imagine a garden hose with a kink – the water doesn’t flow smoothly, creating noise and pressure. Similarly, a stenotic aortic valve forces the heart to work harder, generating the audible turbulence heard through a stethoscope.
The primary culprit behind this narrowing is often calcification, a process where calcium deposits build up on the valve leaflets, stiffening and restricting their movement. This is particularly common in older adults, with age being a significant risk factor. Think of it as rust accumulating on a hinge, gradually impairing its function. Other causes include congenital defects, where individuals are born with a malformed aortic valve, and rheumatic fever, a complication of untreated strep throat that can scar the valve. Less frequently, radiation therapy to the chest area can also lead to aortic stenosis over time.
Each cause leaves its mark on the valve, ultimately resulting in the same telltale sound – a murmur that whispers of a struggling heart.
Understanding the cause of aortic stenosis is crucial for determining the best course of treatment. For instance, while medication can manage symptoms, surgical valve replacement is often necessary for severe cases, especially those caused by calcification. Early detection through auscultation (listening with a stethoscope) and diagnostic tests like echocardiograms is key to preventing complications like heart failure.
Do You Recognize This Sound? Unraveling the Mystery Behind Familiar Noises
You may want to see also
Explore related products






![]()
Characteristics of the Murmur
The aortic stenosis murmur is a crescendo-decrescendo sound, often described as harsh and diamond-shaped, best heard at the right second intercostal space with the patient in the supine position and the phonoscope tilted slightly toward the left sternal border. This classic murmur reflects the turbulent flow of blood across a narrowed aortic valve, a hallmark of the condition. Its timing is crucial: it begins slightly after the onset of systole, peaks midway, and then tapers off before the second heart sound (S2), distinguishing it from other systolic murmurs like hypertrophic cardiomyopathy, which often has a louder, more forceful quality.
Intensity and radiation patterns further refine the diagnosis. The murmur’s loudness, graded on a 1-6 scale, correlates with stenosis severity, though this is not always linear due to factors like calcification or pressure gradients. Radiation to the carotids is common, but in severe cases, it may extend to the apex or even be audible across the precordium. A notable absence of radiation to the axilla or back helps differentiate aortic stenosis from conditions like bicuspid aortic valve disease. Clinicians should also note that the murmur may diminish in late-stage disease due to reduced stroke volume, a phenomenon known as "burnout."
Dynamic changes during maneuvers provide additional diagnostic clues. Having the patient perform the Valsalva maneuver or squat increases preload, enhancing the murmur’s intensity and duration. Conversely, standing abruptly decreases venous return, causing the murmur to soften or shorten. These responses contrast with mitral regurgitation, where the murmur lengthens with standing. Such maneuvers are particularly useful in borderline cases or when auscultation is challenging due to obesity or lung sounds.
Finally, associated findings complement the murmur’s characteristics. A delayed, soft, or absent S2 reflects impaired aortic valve closure, while a paradoxically split S2 (widening during inspiration) is nearly pathognomonic for severe stenosis. Late-peaking murmurs in patients over 65 should prompt urgent echocardiography, as this age group is at higher risk for calcific aortic stenosis. For younger patients, particularly those with congenital bicuspid valves, a murmur detected before age 50 warrants further evaluation to assess progression and plan interventions like valve replacement or TAVR.
In practice, mastering these murmur characteristics requires repeated auscultation and correlation with imaging. Digital stethoscopes or smartphone apps can aid in visualization and recording, especially for trainees. However, reliance on technology should not replace the skill of recognizing subtle nuances, such as a murmur that softens with worsening stenosis. Ultimately, the aortic stenosis murmur is not just a sound but a dynamic, informative signal that guides clinical decision-making and patient management.
Creative Ways to Customize and Vary Your Horn Sound Effectively
You may want to see also
Explore related products






![]()
Diagnosis Methods for the Sound
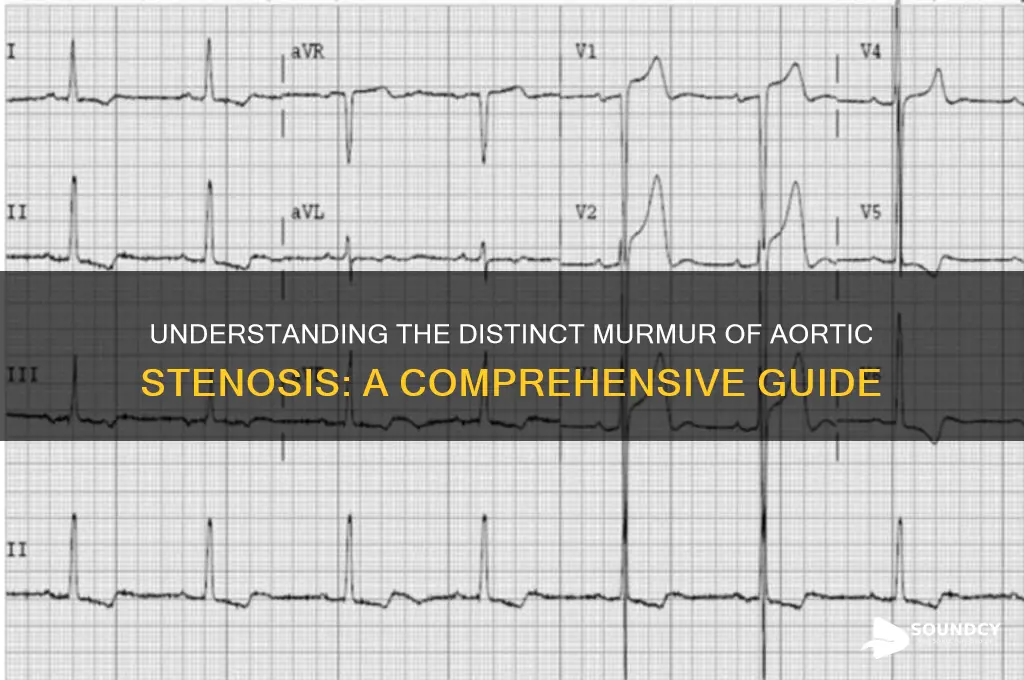
The murmur of aortic stenosis is a crescendo-decrescendo sound, often likened to the closing of an old, creaky door. Its intensity and timing are critical clues for diagnosis. Auscultation, the act of listening to the heart with a stethoscope, remains the cornerstone of identifying this sound. The murmur is typically best heard at the right second intercostal space, radiating to the carotids, and is associated with a delayed or soft second heart sound (S2). This classic presentation, however, can vary depending on the severity and underlying cause of the stenosis.
While auscultation is fundamental, it is not infallible. The subtlety of the murmur in early or mild cases can lead to missed diagnoses, particularly in noisy environments or in patients with obesity or lung disease. This is where adjunctive diagnostic tools become indispensable. Echocardiography, particularly Doppler echocardiography, provides a dynamic, real-time visualization of blood flow across the aortic valve, quantifying the severity of stenosis by measuring the pressure gradient and calculating the valve area. A mean pressure gradient of >40 mmHg or an aortic valve area of <1.0 cm² is diagnostic of severe aortic stenosis, guiding treatment decisions and prognostic assessments.
For patients with inconclusive echocardiographic findings or those unable to undergo standard imaging, cardiac catheterization offers a definitive diagnosis. This invasive procedure involves threading a catheter through the blood vessels to the heart, directly measuring pressures on either side of the aortic valve. While highly accurate, it is reserved for specific cases due to its risks, including bleeding, infection, and contrast-induced nephropathy. The procedure is particularly useful in patients with discrepant non-invasive test results or those with concomitant coronary artery disease requiring angiography.
A less invasive but equally valuable tool is cardiac MRI, which provides detailed anatomical and functional information without radiation exposure. It is particularly useful in patients with contraindications to echocardiography or those requiring precise assessment of left ventricular function and aortic dimensions. However, its longer scan times and higher costs limit its use as a first-line diagnostic modality. Combining these methods ensures a comprehensive evaluation, tailoring the approach to each patient’s unique clinical context.
Finally, emerging technologies such as artificial intelligence (AI) and machine learning are revolutionizing the diagnosis of aortic stenosis sounds. AI algorithms can analyze auscultatory recordings, identifying patterns imperceptible to the human ear and improving diagnostic accuracy, especially in primary care settings. These tools are not yet widely adopted but hold promise for early detection and streamlined referrals. As technology advances, the integration of traditional and innovative methods will redefine the diagnostic landscape for aortic stenosis.
Effective Techniques for Cleaning Your Sound Mixer: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Severity Grading of the Murmur
The intensity and character of the aortic stenosis murmur serve as critical indicators of disease severity, guiding clinical decision-making. Grading the murmur on a scale of 1 to 6, where 1 is barely audible and 6 is loud enough to hear without a stethoscope, provides a standardized framework for assessment. A grade 3 or 4 murmur often signifies moderate stenosis, while grades 5 and 6 typically indicate severe disease. However, murmur intensity alone is not definitive; it must be interpreted alongside other clinical and imaging data. For instance, a soft murmur in a patient with severe calcification on echocardiography may still indicate critical stenosis, as calcified leaflets can impede sound transmission.
Analyzing the murmur’s quality and radiation offers additional insights into severity. A harsh, crescendo-decrescendo murmur radiating to the carotids suggests high-velocity flow across a severely narrowed valve. In contrast, a milder murmur confined to the aortic area may indicate less severe obstruction. Age and comorbidities also influence interpretation; elderly patients with severe stenosis may have softer murmurs due to reduced flow from diminished cardiac output. Conversely, younger patients with dynamic left ventricular function often exhibit louder murmurs, even with moderate stenosis.
Practical tips for accurate grading include positioning the patient in various postures, such as standing or squatting, to augment or diminish the murmur. Standing decreases venous return, reducing murmur intensity, while squatting increases preload, amplifying it. Auscultation should be performed with the diaphragm of the stethoscope over the right second intercostal space, the optimal location for detecting aortic valve sounds. Documenting the murmur’s duration relative to systole (e.g., early-peaking vs. late-peaking) further refines the assessment, as late-peaking murmurs are more indicative of severe stenosis.
Comparing the aortic stenosis murmur to other pathologies highlights its unique characteristics. Unlike the softer, blowing murmur of aortic regurgitation, stenosis produces a harsh, diamond-shaped sound. Hypertrophic cardiomyopathy may cause a similar murmur but is typically louder with the patient in the upright position and decreases with Valsalva maneuvers. Rheumatic valve disease, another differential, often presents with a rough, irregular murmur, whereas aortic stenosis is smooth and consistent. Recognizing these distinctions ensures accurate diagnosis and grading.
In conclusion, severity grading of the aortic stenosis murmur requires a multifaceted approach, integrating intensity, quality, radiation, and contextual factors. While murmur grading is a cornerstone of clinical evaluation, it should always be corroborated with imaging studies like echocardiography for definitive assessment. Mastery of this skill enables clinicians to stratify patient risk, monitor disease progression, and determine optimal timing for intervention, ultimately improving outcomes in this high-stakes condition.
Waterfall Sounds: A Natural Crime Deterrent in Urban Environments
You may want to see also
Explore related products



$35.99 $59.99



![]()
Treatment Options for Aortic Stenosis
Aortic stenosis, characterized by a narrowed aortic valve, produces a distinct, harsh, crescendo-decrescendo murmur best heard at the right second intercostal space. This sound is a critical diagnostic clue, but it’s only the beginning of patient management. Treatment options for aortic stenosis are not one-size-fits-all; they depend on disease severity, symptoms, and patient-specific factors. Here’s a focused guide to navigating these options effectively.
Surgical Aortic Valve Replacement (SAVR) remains the gold standard for severe, symptomatic aortic stenosis, particularly in younger patients (under 65) or those with a longer life expectancy. This open-heart procedure involves removing the damaged valve and replacing it with a mechanical or bioprosthetic valve. Mechanical valves, made of durable materials like carbon, last a lifetime but require lifelong anticoagulation with warfarin (target INR 2.0–3.0). Bioprosthetic valves, often derived from animal tissue, degrade over 10–15 years but eliminate the need for anticoagulation, making them suitable for older adults. Post-operative recovery typically spans 6–12 weeks, with strict activity restrictions in the first month.
Transcatheter Aortic Valve Replacement (TAVR) has revolutionized care for high-risk or inoperable patients, often those over 70 or with comorbidities. This minimally invasive procedure delivers a collapsible valve via a catheter inserted through the femoral artery or a small chest incision. TAVR reduces hospital stays to 2–3 days compared to 7–10 days for SAVR, but it carries risks like vascular complications or valve leakage. Patients must take dual antiplatelet therapy (e.g., aspirin 81 mg daily + clopidogrel 75 mg daily) for 3–6 months post-procedure. While initially approved for severe, symptomatic stenosis, TAVR is now being explored for lower-risk patients due to advancing technology.
For asymptomatic patients with severe aortic stenosis, watchful waiting with regular echocardiograms and clinical evaluations is often recommended. However, this approach requires vigilance, as symptoms can develop rapidly. Once symptoms like chest pain, syncope, or heart failure arise, intervention becomes urgent. Medications like diuretics or beta-blockers may manage symptoms temporarily but do not halt disease progression. Early referral to a cardiothoracic surgeon or interventional cardiologist is critical, as untreated severe stenosis carries a 2-year mortality rate exceeding 50%.
Emerging therapies, such as balloon valvuloplasty, offer palliative relief for select cases, particularly in children or as a bridge to definitive treatment. This procedure uses a balloon catheter to widen the stenotic valve, improving blood flow temporarily. However, restenosis occurs within months, limiting its utility in adults. Clinical trials are also exploring valve repair techniques and novel bioprosthetics, aiming to extend durability and reduce complications. Patients should discuss these options with their healthcare team, weighing risks, benefits, and long-term outcomes.
In summary, treatment for aortic stenosis hinges on timely, individualized intervention. From SAVR and TAVR to watchful waiting and palliative measures, each option addresses specific patient needs. Recognizing the characteristic murmur is the first step; understanding these treatment pathways ensures optimal care for this life-threatening condition.
Discovering Your Unique SoundID: A Guide to Finding References
You may want to see also
Frequently asked questions
The sound of aortic stenosis is a harsh, crescendo-decrescendo (diamond-shaped) murmur that is best heard at the right second intercostal space, radiating to the carotids.
The aortic stenosis murmur is typically late-peaking, reflecting the delayed opening of the stenotic aortic valve, and has a characteristic diamond shape, distinguishing it from other murmurs like mitral regurgitation or aortic regurgitation.
The sound is caused by turbulent blood flow through a narrowed or stenotic aortic valve, which obstructs blood flow from the left ventricle to the aorta.
No, the aortic stenosis sound is a high-pitched murmur that requires a stethoscope to be heard, as it is not audible to the naked ear.
Associated findings may include a delayed or soft S2 heart sound (aortic component), a narrow pulse pressure, and in severe cases, signs of heart failure such as S3 gallop or pulmonary rales.