Croup, characterized by its distinctive barking cough and stridor, is often associated with viral infections in children. However, several other conditions can mimic its symptoms, leading to potential misdiagnosis. Conditions such as epiglottitis, foreign body aspiration, bacterial tracheitis, and even asthma or recurrent respiratory papillomatosis can present with similar respiratory distress, cough, or noisy breathing. Understanding these differential diagnoses is crucial for healthcare providers to ensure accurate assessment and appropriate management, as some of these conditions may require urgent medical intervention.
| Characteristics | Values |
|---|---|
| Conditions | Epiglottitis, Viral Laryngotracheobronchitis, Bacterial Tracheitis, Foreign Body Aspiration, Allergic Laryngitis, Recurrent Respiratory Papillomatosis, Vocal Cord Dysfunction, Gastroesophageal Reflux Disease (GERD) |
| Age Group | Infants, Children (most common), Occasionally Adults |
| Symptoms | Barking cough, Stridor (noisy breathing), Hoarseness, Difficulty breathing, Fever, Retractions (chest wall sinking in), Drooling (in epiglottitis) |
| Onset | Sudden (epiglottitis), Gradual (viral croup), Acute (foreign body) |
| Seasonality | More common in fall and winter (viral croup) |
| Risk Factors | Young age, Viral infections, Allergies, GERD, Immunodeficiency |
| Diagnostic Features | Stridor on inspiration (croup), Stridor on expiration (foreign body), Fever and drooling (epiglottitis), Absence of barking cough (other conditions) |
| Treatment | Humidified air, Steroids (croup), Antibiotics (bacterial tracheitis), Emergency airway management (epiglottitis), Removal of foreign body (aspiration) |
| Prognosis | Usually resolves within 3-7 days (croup), Serious if untreated (epiglottitis, bacterial tracheitis) |
| Prevention | Vaccination (e.g., DTaP, Hib), Avoiding allergens, Proper supervision to prevent foreign body aspiration |
Explore related products






What You'll Learn
- Barking Cough Mimickers: Other conditions like asthma, bronchiolitis, or pneumonia can mimic croup’s distinctive cough
- Foreign Body Aspiration: Inhaled objects can cause stridor and cough, resembling croup symptoms in children
- Viral Laryngotracheitis: Similar to croup, this infection causes inflammation and barking cough in the airway
- Allergic Reactions: Severe allergies can lead to swelling in the throat, producing croup-like stridor
- Epiglottitis: Though rare, this infection causes swelling, stridor, and breathing difficulty, often confused with croup
![]()
Barking Cough Mimickers: Other conditions like asthma, bronchiolitis, or pneumonia can mimic croup’s distinctive cough
The distinctive "barking" cough of croup is often unmistakable, but it’s not the only condition that can produce such a sound. Parents and caregivers must remain vigilant, as other respiratory illnesses can mimic this symptom, leading to potential misdiagnosis. Asthma, bronchiolitis, and pneumonia, for instance, can all present with coughs that resemble croup, especially in young children. Recognizing the nuances between these conditions is crucial for timely and appropriate treatment.
Consider asthma, a chronic condition often triggered by allergens, exercise, or respiratory infections. While asthma typically causes a wheezing sound, it can also produce a barking cough, particularly during acute flare-ups. Unlike croup, which is usually viral and self-limiting, asthma requires long-term management. Key differentiators include a history of recurrent breathing difficulties, family history of asthma, and response to bronchodilators like albuterol. For children over 2 years old, a trial of albuterol may help distinguish between asthma and croup—improvement in symptoms suggests asthma.
Bronchiolitis, another common mimic, primarily affects infants under 2 years old and is often caused by respiratory syncytial virus (RSV). While it typically presents with wheezing and rapid breathing, some cases can produce a barking cough, especially as the illness progresses. Unlike croup, bronchiolitis often includes fever, nasal congestion, and severe respiratory distress. Treatment is largely supportive, focusing on hydration and oxygen therapy if needed. Parents should monitor for signs of dehydration, such as reduced urine output, and seek medical attention if the child struggles to breathe.
Pneumonia, an infection of the lung tissue, can also mimic croup’s cough, particularly in its early stages. However, pneumonia often presents with additional symptoms like high fever, chest pain, and labored breathing. In children, bacterial pneumonia may require antibiotics, while viral cases are managed symptomatically. A chest X-ray is typically needed to confirm the diagnosis. Parents should be aware that pneumonia can progress rapidly, especially in young children, and prompt medical evaluation is essential.
To differentiate these conditions, observe the child’s overall symptoms and behavior. Croup often includes a hoarse voice and a cough that worsens at night, while asthma may be accompanied by chest tightness and a history of allergies. Bronchiolitis typically affects younger infants and includes significant nasal congestion, whereas pneumonia often presents with persistent fever and lethargy. When in doubt, consult a healthcare provider for a thorough assessment, as misidentification can delay appropriate treatment. Practical tips include keeping a symptom diary, using a cool-mist humidifier for croup, and ensuring the child is up-to-date on vaccinations to prevent complications from conditions like pneumonia.
The Revolutionary Birth of Synchronized Sound in Cinema
You may want to see also
Explore related products






![]()
Foreign Body Aspiration: Inhaled objects can cause stridor and cough, resembling croup symptoms in children
Children’s airways are narrow, and their curiosity is boundless—a dangerous combination that makes foreign body aspiration a real risk. Small objects like peanuts, beads, or toy parts can easily slip past their developing swallowing reflexes, lodging in the trachea or bronchi. When this happens, the body’s immediate response is inflammation and irritation, triggering symptoms that eerily mimic croup: a barking cough, stridor (a high-pitched noise during inhalation), and respiratory distress. Unlike croup, however, this condition is a medical emergency requiring swift intervention.
Consider a scenario: a 2-year-old presents with sudden onset stridor and cough after playing with a coin. The parent might assume it’s croup, especially during viral season. But key red flags differentiate the two: foreign body aspiration often follows a choking episode, symptoms are unilateral (one side of the chest may appear less active during breathing), and there’s no preceding viral illness. A careful history is critical—ask about recent eating or play activities involving small objects. For infants under 1, formula or breast milk aspiration can also cause similar symptoms, though less common.
Diagnosis hinges on suspicion and imaging. A chest X-ray may show an opaque object or air trapping, but up to 20% of cases appear normal. If aspiration is suspected, rigid bronchoscopy under general anesthesia is the gold standard for both diagnosis and removal. Delaying this procedure increases the risk of complications like pneumonia or airway obstruction. Parents should be advised to keep high-risk items (popcorn, buttons, balloons) out of reach and supervise snack time closely—children under 4 are particularly vulnerable due to their tendency to mouth objects.
Prevention is paramount, but accidents happen. If a child shows sudden respiratory distress after a choking event, assume foreign body aspiration until proven otherwise. Do not attempt the Heimlich maneuver if the child is breathing; this can dislodge the object further into the airway. Instead, seek immediate medical attention. For healthcare providers, a high index of suspicion is key—what seems like croup could be a life-threatening obstruction waiting to escalate. Quick action saves lives.
HDMI Graphics Cards: Visuals and Audio Combined
You may want to see also
Explore related products






![]()
Viral Laryngotracheitis: Similar to croup, this infection causes inflammation and barking cough in the airway
A barking cough echoing through the house at night can send any parent into a panic, often assuming it’s croup. But viral laryngotracheitis, though less known, shares this hallmark symptom and can easily be mistaken for its more famous counterpart. This infection, typically caused by parainfluenza viruses, targets the larynx and trachea, triggering inflammation that narrows the airway. The result? A cough that sounds like a seal’s bark, fever, and sometimes difficulty breathing. While croup often strikes in the fall and winter, viral laryngotracheitis follows a similar seasonal pattern, adding to the confusion.
Diagnosing viral laryngotracheitis isn’t as straightforward as identifying croup. Unlike croup, which often presents with a distinctive stridor (a high-pitched breathing sound), viral laryngotracheitis may cause more pronounced hoarseness or a complete loss of voice. A healthcare provider might use a stethoscope to listen for wheezing or order a neck X-ray to rule out other conditions. Parents should watch for signs of severe distress, such as rapid breathing, bluish lips, or extreme fatigue, which warrant immediate medical attention.
Treatment for viral laryngotracheitis focuses on symptom relief, much like croup. Cool mist humidifiers can soothe irritated airways, while hydration is key to thinning mucus and easing coughs. For fever or discomfort, acetaminophen (10–15 mg/kg every 4–6 hours) or ibuprofen (10 mg/kg every 6–8 hours) can be administered, following age-appropriate dosing guidelines. Avoid cough suppressants, as coughing helps clear the airway. In severe cases, a healthcare provider might prescribe a short course of oral corticosteroids to reduce inflammation, though this is less common than with croup.
Prevention hinges on the same strategies used to avoid respiratory viruses: frequent handwashing, avoiding close contact with sick individuals, and keeping children up to date on vaccinations. While there’s no specific vaccine for viral laryngotracheitis, the measles-mumps-rubella (MMR) vaccine can prevent complications from related viruses. For parents, the key takeaway is to remain vigilant but not alarmed. Most cases resolve within a week, and with proper care, the barking cough will fade into silence, leaving only a lesson in the nuances of childhood illnesses.
The Shocking Truth: What Does Electrocution Actually Sound Like?
You may want to see also
Explore related products






![]()
Allergic Reactions: Severe allergies can lead to swelling in the throat, producing croup-like stridor
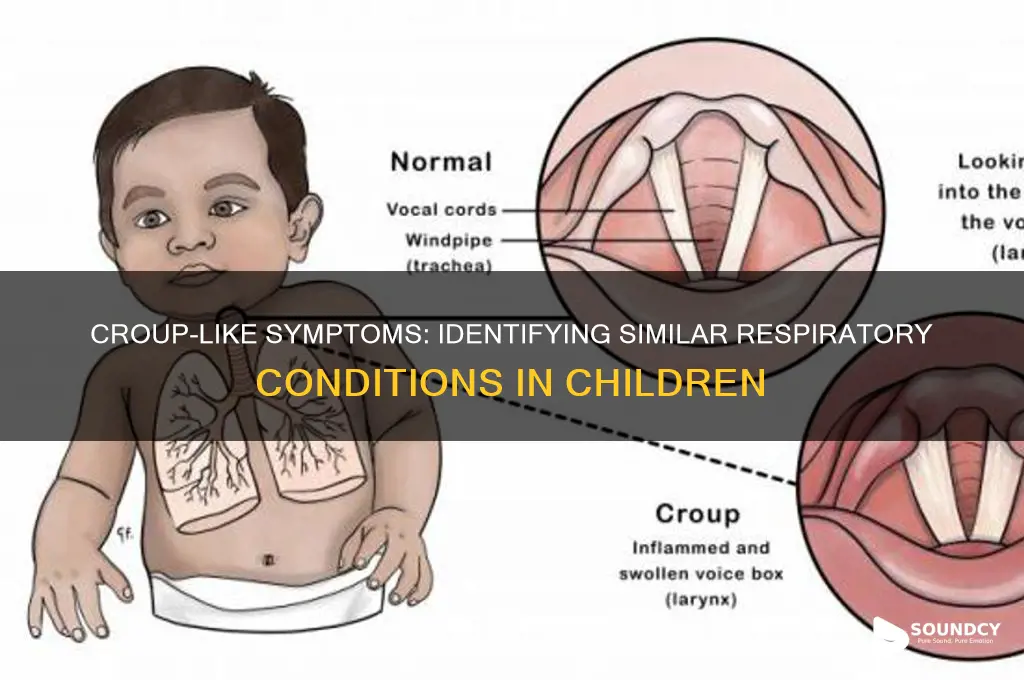
Severe allergic reactions, particularly anaphylaxis, can cause rapid swelling in the throat, leading to a high-pitched, croup-like stridor. This occurs when the body releases histamines and other chemicals in response to an allergen, triggering inflammation in the upper airway. Unlike croup, which is often viral and affects the voice box (larynx) and windpipe (trachea), allergic stridor is a life-threatening emergency requiring immediate intervention. Recognizing the difference is critical: croup typically presents with a barking cough and fever, while allergic stridor is accompanied by hives, difficulty breathing, and a rapid onset after exposure to an allergen like peanuts, bee stings, or medications.
To manage allergic stridor, administer an epinephrine auto-injector (e.g., EpiPen) immediately, delivering 0.15–0.3 mg of epinephrine intramuscularly into the thigh. For children under 30 kg, use a 0.15 mg dose; for older children and adults, use 0.3 mg. Position the person on their back and elevate their legs to maintain blood flow. Call emergency services promptly, as epinephrine’s effects last only 10–20 minutes, and symptoms may recur. Avoid antihistamines or inhalers as primary treatments, as they are insufficient for severe airway swelling.
Prevention is key for those with known severe allergies. Always carry two epinephrine auto-injectors, as 15–20% of anaphylactic reactions require a second dose. Wear medical alert jewelry, and inform caregivers, teachers, or coworkers of the allergy. For children, ensure schools have an anaphylaxis emergency plan and staff trained in epinephrine administration. Regularly check expiration dates on auto-injectors, as potency diminishes over time.
Comparing allergic stridor to croup highlights the importance of context. Croup’s stridor is inspiratory (during inhalation), while allergic stridor may be both inspiratory and expiratory due to severe airway compromise. Croup improves with humidified air or steroids, whereas allergic stridor demands epinephrine. Misdiagnosis can be fatal, so consider allergy history, symptom onset, and associated signs like swelling or hives. When in doubt, treat for anaphylaxis first, as epinephrine is safe even if the cause is viral croup.
In summary, allergic reactions causing croup-like stridor are medical emergencies requiring swift action. Familiarize yourself with anaphylaxis symptoms, carry epinephrine, and act decisively. While croup is manageable with supportive care, allergic stridor demands immediate epinephrine and emergency care. Understanding these distinctions can save lives, ensuring the right treatment is given without delay.
Unveiling the Eerie Howls: What Do Coyotes Sound Like?
You may want to see also
Explore related products





![]()
Epiglottitis: Though rare, this infection causes swelling, stridor, and breathing difficulty, often confused with croup
Epiglottitis, though rare, demands immediate attention due to its life-threatening potential. This bacterial infection causes rapid swelling of the epiglottis, the flap that covers the windpipe during swallowing. The hallmark symptoms—stridor (a high-pitched breathing sound), drooling, and difficulty breathing—often mimic croup, leading to misdiagnosis. Unlike croup, which typically presents with a barking cough and is more common in children aged 6 months to 3 years, epiglottitis can affect any age group, though it’s more severe in children under 5. The urgency here is critical: epiglottitis requires prompt medical intervention, often involving hospitalization, intravenous antibiotics (such as ceftriaxone or vancomycin), and airway management to prevent respiratory failure.
To distinguish epiglottitis from croup, observe the child’s posture and behavior. Children with epiglottitis often sit upright, leaning forward, and may refuse to lie down due to breathing discomfort. They may also exhibit a "tripod position," sitting with their hands on their knees to stabilize their chest. In contrast, croup symptoms are usually less severe, with a characteristic cough that worsens at night. A key diagnostic clue is the absence of fever in croup, whereas epiglottitis often presents with high fever and severe distress. If epiglottitis is suspected, avoid examining the throat, as this can trigger airway obstruction; instead, seek emergency care immediately.
Prevention plays a crucial role in reducing epiglottitis cases. The Haemophilus influenzae type b (Hib) vaccine, introduced in the 1990s, has drastically reduced incidence rates, particularly in vaccinated populations. Ensure children receive the full Hib vaccine series, typically administered at 2, 4, and 6 months, with a booster at 12–15 months. Adults with compromised immune systems or asplenia should also consider Hib vaccination. Despite its rarity today, awareness of epiglottitis remains vital, as delayed treatment can lead to fatal outcomes.
For parents and caregivers, recognizing the differences between croup and epiglottitis is essential. Croup’s barking cough and mild symptoms often resolve with home care, such as humidified air or a cool mist humidifier. Epiglottitis, however, requires urgent medical attention. If a child shows signs of severe respiratory distress, such as stridor at rest, inability to speak or cry, or blue lips, call emergency services immediately. Do not attempt to transport the child without professional assistance, as airway obstruction can worsen during movement. Quick action can save lives, making knowledge of these distinctions invaluable.
Lexus 250 2010 Sound Quality: A Comprehensive Review and Analysis
You may want to see also
Frequently asked questions
Conditions like asthma, bronchiolitis, pneumonia, and viral upper respiratory infections can produce coughs or breathing sounds that resemble croup.
Yes, severe allergies or gastroesophageal reflux disease (GERD) can sometimes trigger a barky cough or noisy breathing similar to croup.
Yes, bacterial infections like epiglottitis or bacterial tracheitis can cause stridor or a barking cough, though they are typically more severe and require immediate medical attention.