The S3 sound, often referred to as a ventricular gallop, is a significant finding in cardiac auscultation that indicates increased ventricular filling and can be a sign of underlying heart conditions. Typically heard during early diastole, it is characterized by an extra heart sound following the S1 and S2 heart sounds, creating a rhythm akin to the word Kentucky. The presence of an S3 sound may suggest conditions such as heart failure, volume overload, or reduced ventricular compliance, making it a critical diagnostic clue for healthcare professionals to assess cardiac function and initiate appropriate interventions.
Explore related products






What You'll Learn
- S3 Gallop Rhythm: Indicates heart failure, fluid overload, or volume expansion, often heard in systole
- Pathological vs. Physiological: Distinguishes between normal (youth, athletes) and abnormal (heart disease) S3 sounds
- Association with Heart Failure: S3 gallop is a key sign of left ventricular dysfunction
- Diagnostic Importance: Helps assess cardiac function, especially in congestive heart failure patients
- Differential Diagnosis: Links S3 to conditions like dilated cardiomyopathy or valvular disease
![]()
S3 Gallop Rhythm: Indicates heart failure, fluid overload, or volume expansion, often heard in systole
The S3 gallop rhythm, a distinct cardiac sound, serves as a critical indicator of underlying cardiovascular issues, particularly heart failure, fluid overload, or volume expansion. This additional heart sound, often described as a low-pitched "ventricular gallop," occurs during the rapid filling phase of the right or left ventricle in early diastole, but it is often perceived as part of systole due to its timing. Clinicians should be vigilant for this sound, as its presence can signal significant cardiac dysfunction, especially in patients with risk factors such as hypertension, diabetes, or a history of myocardial infarction.
To identify an S3 gallop, auscultate the patient in a left lateral decubitus position, focusing on the cardiac apex. The sound is best heard with the bell of the stethoscope and is characterized by a rhythm that resembles the cadence of the phrase "Kentucky Derby." Its detection requires a keen ear, as the S3 is softer and lower in pitch compared to the S1 and S2 heart sounds. Patients with an S3 gallop may also present with symptoms such as dyspnea, fatigue, or peripheral edema, further reinforcing the need for a comprehensive clinical evaluation.
From a pathophysiological perspective, the S3 gallop arises from increased ventricular filling pressures, often due to impaired diastolic relaxation or elevated blood volume. This can occur in conditions like congestive heart failure, where the heart struggles to pump blood effectively, leading to fluid accumulation in the lungs or extremities. In younger patients, particularly athletes, an S3 gallop may be physiological and benign, but in older adults or those with comorbidities, it is almost always pathological. Differentiating between these scenarios is crucial for appropriate management.
Management of patients with an S3 gallop focuses on addressing the underlying cause. For heart failure, guideline-directed medical therapy, including ACE inhibitors, beta-blockers, and diuretics, is essential. Dosages should be individualized based on patient tolerance and renal function, with close monitoring for electrolyte imbalances. Lifestyle modifications, such as sodium restriction (<2,000 mg/day) and regular exercise, can also improve outcomes. In cases of volume overload, diuretics like furosemide (initial dose: 20–40 mg orally) may be prescribed to reduce fluid retention, though caution is advised to avoid over-diuresis.
In conclusion, the S3 gallop rhythm is a vital auscultatory finding that demands prompt recognition and intervention. Its association with heart failure, fluid overload, or volume expansion underscores the importance of early diagnosis and targeted therapy. Clinicians should integrate this knowledge into their practice, ensuring that patients receive timely and effective care to mitigate the progression of cardiac disease. By mastering the detection and management of the S3 gallop, healthcare providers can significantly improve patient outcomes and quality of life.
Mastering Sound Art: Creative Techniques for Aspiring Audio Innovators
You may want to see also
Explore related products





![]()
Pathological vs. Physiological: Distinguishes between normal (youth, athletes) and abnormal (heart disease) S3 sounds
The S3 heart sound, often described as a low-pitched "vibratory" sound, can be a subtle yet crucial indicator of cardiac function. However, its presence isn't always a cause for alarm. Understanding the context—whether the S3 is physiological or pathological—is essential for accurate interpretation.
Physiological S3: A Sign of Vigor, Not Distress
In certain individuals, an S3 sound is a normal finding, reflecting a healthy, robust cardiovascular system. This is particularly true for children and adolescents, where a physiological S3 is common due to increased stroke volume and rapid ventricular filling. Athletes, especially endurance athletes, may also exhibit a physiological S3. Their hearts, adapted to sustained physical stress, demonstrate increased ventricular compliance, allowing for a more pronounced early diastolic filling wave, which manifests as the S3 sound.
This physiological S3 typically disappears with age and is absent during expiration.
Pathological S3: A Red Flag for Underlying Issues
In contrast, an S3 sound in adults, particularly those over 40, or in individuals with risk factors for heart disease, warrants further investigation. A pathological S3 often signifies impaired ventricular function, where the heart struggles to fill adequately during diastole. This can be a hallmark of various conditions, including:
- Heart failure: Both systolic and diastolic heart failure can lead to a pathological S3.
- Ischemic heart disease: Reduced blood flow to the heart muscle can impair its ability to relax and fill properly.
- Valvular heart disease: Conditions like aortic stenosis or mitral regurgitation can disrupt normal blood flow patterns, leading to an S3.
Distinguishing Features: Key to Accurate Diagnosis
Differentiating between physiological and pathological S3 relies on a combination of factors:
- Patient demographics: Age, activity level, and medical history are crucial.
- Timing and characteristics: A physiological S3 is typically soft, occurs in early diastole, and may be present only during inspiration. A pathological S3 is often louder, sustained, and may be audible throughout diastole.
- Associated findings: Presence of other heart sounds, murmurs, or signs of heart failure (e.g., edema, shortness of breath) strongly suggest a pathological cause.
Clinical Implications and Next Steps
Identifying the nature of an S3 sound is crucial for guiding further diagnostic and therapeutic interventions. While a physiological S3 is benign and requires no intervention, a pathological S3 necessitates a thorough workup to identify the underlying cause. This may involve echocardiography, stress testing, or other imaging modalities. Early detection and treatment of the underlying condition can significantly improve patient outcomes and prevent complications.
Business Opportunities on Hobe Sound's Iconic Bridge
You may want to see also
Explore related products




![]()
Association with Heart Failure: S3 gallop is a key sign of left ventricular dysfunction
The S3 gallop, often described as a ventricular gallop or protodiastolic gallop, is a distinct heart sound that signals a critical issue: left ventricular dysfunction. This additional sound, heard as a soft, low-pitched "lub-dub-ta," occurs in early diastole and reflects increased volume or pressure within the left ventricle. While it can be present in healthy individuals, particularly children and young adults, its persistence or onset in adulthood is a red flag, especially when associated with symptoms like fatigue, shortness of breath, or edema. Recognizing this sound is crucial, as it often precedes overt heart failure symptoms and can guide early intervention.
To understand the S3 gallop’s significance, consider the physiology behind it. In a healthy heart, the left ventricle fills passively during early diastole. However, in left ventricular dysfunction, the ventricle becomes stiff or dilated, impairing its ability to relax and fill efficiently. This dysfunction creates a rapid, turbulent blood flow, generating the S3 sound. Conditions like hypertension, ischemic heart disease, or valvular disorders can exacerbate this process, making the S3 gallop a marker of worsening cardiac function. Clinicians often use this sound as a non-invasive tool to assess disease progression and treatment efficacy.
Identifying an S3 gallop requires careful auscultation, typically using a bell-shaped stethoscope over the cardiac apex. The sound is best heard with the patient in the left lateral decubitus position and during expiration. However, interpretation must be cautious, as factors like age, body habitus, and background noise can confound detection. For instance, an S3 gallop in a young athlete may be benign, while the same sound in a 60-year-old with hypertension is concerning. Combining auscultation with diagnostic tools like echocardiography or BNP levels can confirm left ventricular dysfunction and guide management.
From a treatment perspective, addressing the underlying cause of left ventricular dysfunction is paramount. For hypertensive patients, optimizing blood pressure control with medications like ACE inhibitors or beta-blockers can reduce ventricular stress. In ischemic heart disease, revascularization procedures or statin therapy may improve outcomes. Lifestyle modifications, such as sodium restriction and regular exercise, are also critical. Monitoring for an S3 gallop during follow-up visits can help assess treatment response and prevent progression to overt heart failure, emphasizing its role as both a diagnostic and prognostic marker.
In summary, the S3 gallop is more than just an auscultatory finding—it’s a call to action. Its presence in adults, particularly those with risk factors for heart disease, warrants prompt evaluation and intervention. By understanding its association with left ventricular dysfunction, healthcare providers can identify early-stage heart failure, implement targeted therapies, and potentially alter the disease course. This underscores the importance of mastering auscultation skills and integrating clinical findings with advanced diagnostics for optimal patient care.
Boost Your PC's Audio: Simple Tips to Increase Sound Quality
You may want to see also
Explore related products






![]()
Diagnostic Importance: Helps assess cardiac function, especially in congestive heart failure patients
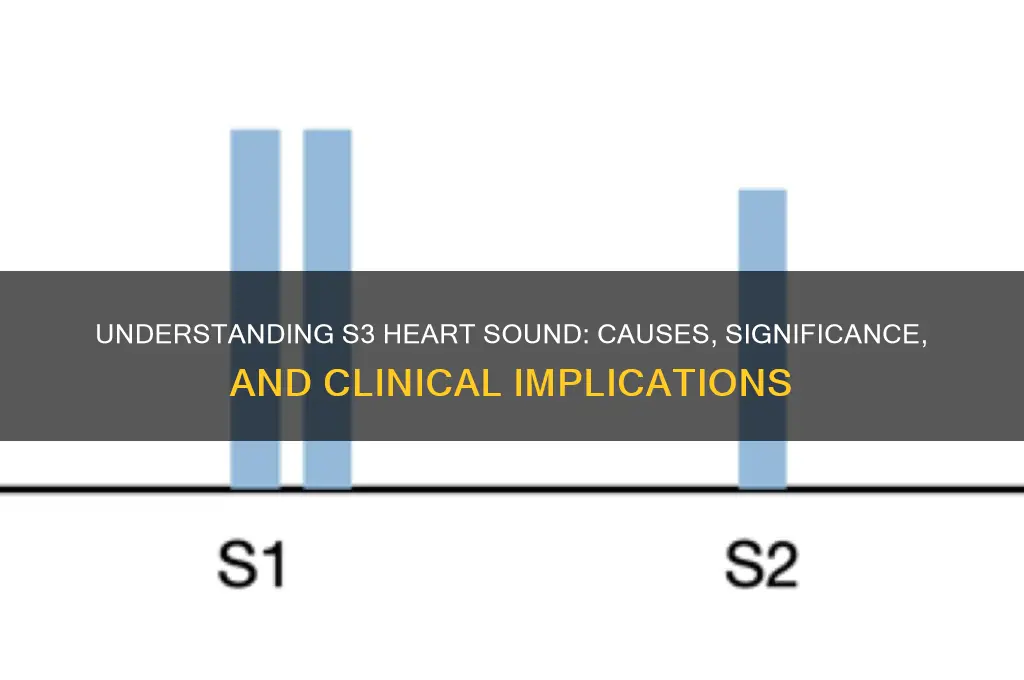
The S3 heart sound, often described as a low-pitched "ventricular gallop," is a critical diagnostic marker for clinicians assessing cardiac function. Its presence can signal increased ventricular filling pressures, a hallmark of congestive heart failure (CHF). Unlike the normal two-component heartbeat (lub-dub), the S3 adds a third sound, creating a rhythm akin to the word "Kentucky." This additional sound typically occurs in early diastole, approximately 0.12 to 0.18 seconds after the S2, and is best heard with the bell of a stethoscope at the apex of the heart. Recognizing the S3 is essential, as it often indicates a decline in cardiac output and can prompt timely intervention in CHF patients.
To effectively utilize the S3 sound in diagnosis, clinicians must follow a systematic approach. Begin by positioning the patient in the left lateral decubitus position, which enhances sound detection. Use firm pressure with the stethoscope bell to filter out higher-pitched noises and focus on lower frequencies. The S3 is most audible in younger patients or those with less severe CHF, as advanced cases may mask the sound due to reduced compliance of the ventricle. Combining auscultation with echocardiography can confirm the diagnosis, as the S3 often correlates with elevated left ventricular end-diastolic pressure (>16 mmHg). This multimodal approach ensures accuracy and provides a comprehensive view of cardiac function.
While the S3 sound is a valuable diagnostic tool, its interpretation requires caution. Not all S3 sounds indicate pathology; benign S3s can occur in children, young adults, and well-trained athletes due to increased ventricular compliance. Differentiating between benign and pathological S3s involves considering patient history, symptoms, and additional diagnostic findings. For instance, a pathological S3 in a 60-year-old with dyspnea and peripheral edema strongly suggests CHF, whereas the same sound in a 20-year-old athlete is likely benign. Clinicians must avoid overdiagnosis by integrating clinical context with auscultatory findings.
The practical implications of identifying an S3 sound in CHF patients are profound. Early detection allows for prompt initiation of guideline-directed medical therapy, such as angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, or diuretics, which can slow disease progression and improve quality of life. For example, in a 55-year-old patient with an S3 and elevated B-type natriuretic peptide (BNP) levels, starting a low-dose ACE inhibitor (e.g., lisinopril 5 mg daily) and titrating upward can reduce ventricular stress and improve symptoms. Regular follow-up auscultation can monitor treatment efficacy, as resolution of the S3 often correlates with improved cardiac function.
In conclusion, the S3 heart sound serves as a vital diagnostic indicator of cardiac dysfunction, particularly in congestive heart failure. Its detection requires skill, context, and corroboration with other diagnostic tools. By mastering the art of auscultation and understanding the nuances of the S3, clinicians can enhance patient care, optimize treatment strategies, and ultimately improve outcomes for those with compromised cardiac function. This simple yet powerful auditory clue underscores the importance of a thorough physical examination in modern cardiology.
Exploring the SNES: Unlocking the Secrets of Its 16-Bit Sound
You may want to see also
Explore related products






![]()
Differential Diagnosis: Links S3 to conditions like dilated cardiomyopathy or valvular disease
The presence of an S3 heart sound, often described as a low-pitched "ventricular gallop," is a critical clinical finding that demands careful differential diagnosis. Unlike the benign S3 sometimes heard in children or athletes, an S3 in adults typically signifies increased ventricular filling pressures, pointing to underlying cardiac pathology. Two conditions prominently linked to this finding are dilated cardiomyopathy (DCM) and valvular disease, each with distinct mechanisms but converging on the pathophysiology of volume overload.
In dilated cardiomyopathy, the ventricle becomes enlarged and compliant, impairing its ability to eject blood effectively. As ejection fraction declines, blood accumulates in the ventricle during diastole, leading to elevated end-diastolic pressures. The S3 in DCM arises from rapid, forceful filling of the distended ventricle early in diastole, creating a palpable and audible third heart sound. Patients with DCM often present with symptoms of heart failure—dyspnea, fatigue, and edema—and may have a history of hypertension, alcohol use, or genetic predisposition. Diagnosis is confirmed via echocardiography, revealing a dilated left ventricle with reduced systolic function. Treatment focuses on symptom management and slowing disease progression, including ACE inhibitors, beta-blockers, and aldosterone antagonists, with dosages titrated based on patient tolerance and renal function.
Valvular disease, particularly mitral or aortic regurgitation, also produces an S3 through a different mechanism. In mitral regurgitation, blood flows backward into the left atrium during systole, increasing atrial and ventricular volumes. This heightened preload causes a rapid, forceful early diastolic filling wave, generating the S3 sound. Aortic regurgitation similarly leads to volume overload, as blood returns to the left ventricle during diastole, increasing wall stress and filling pressures. Patients with valvular disease may exhibit murmurs on auscultation, and echocardiography is essential to assess valve morphology and severity. Surgical intervention, such as valve repair or replacement, may be necessary for severe cases, particularly when medical management fails to control symptoms or prevent ventricular remodeling.
Distinguishing between these conditions requires a systematic approach. In DCM, the S3 is accompanied by signs of systolic dysfunction, whereas valvular disease typically presents with diastolic murmurs and preserved or mildly reduced ejection fraction. Laboratory tests, such as B-type natriuretic peptide (BNP) levels, can aid in assessing volume status, with elevated BNP (>100 pg/mL) suggesting heart failure. However, BNP is nonspecific and must be interpreted in clinical context. Practical tips for clinicians include correlating the S3 with symptoms, physical exam findings, and imaging data to tailor treatment strategies effectively.
In conclusion, an S3 heart sound is a red flag for volume overload, with dilated cardiomyopathy and valvular disease as key differential diagnoses. Understanding the underlying mechanisms—systolic dysfunction in DCM versus valvular regurgitation—guides diagnostic workup and treatment. Early recognition and intervention are critical to prevent disease progression and improve patient outcomes, emphasizing the importance of a meticulous clinical approach to this auscultatory finding.
Understanding the Science Behind How Shakers Create Vibrant Musical Sounds
You may want to see also
Frequently asked questions
An S3 sound, also known as a "ventricular gallop" or "protodiastolic gallop," often indicates decreased ventricular compliance or volume overload, commonly seen in heart failure, myocardial infarction, or severe hypertension.
Not necessarily. An S3 sound can be physiological in children and young adults, but in older individuals or those with risk factors, it typically suggests underlying cardiac dysfunction or strain.
An S3 sound is a low-pitched, brief sound heard in early diastole, best auscultated at the apex with the patient in the left lateral position. It follows the S2 sound and is distinct from the higher-pitched S1 and S2 sounds.