Epiglottitis is a potentially life-threatening condition characterized by severe inflammation of the epiglottis, a flap of tissue at the base of the tongue that prevents food and liquids from entering the windpipe. When inflamed, the epiglottitis can swell, obstructing the airway and causing distinct respiratory symptoms. One of the hallmark signs of epiglottitis is a high-pitched, whistling sound known as stridor, which occurs during inhalation due to the narrowed airway. Patients may also exhibit a muffled or hoarse voice, difficulty breathing, and a unique tripod position where they sit leaning forward with their hands on their knees to optimize airflow. Recognizing these auditory and visual cues is crucial, as prompt medical intervention is essential to prevent respiratory failure.
Explore related products






What You'll Learn
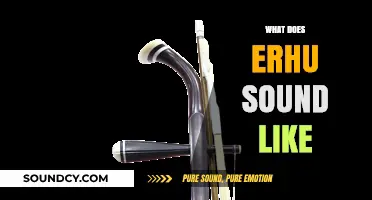
- Stridor in Epiglottitis: High-pitched breathing noise, especially during inhalation, due to upper airway obstruction
- Grunting Sounds: Low-pitched grunting as the body tries to maintain airway pressure against swelling
- Drooling and Muffled Voice: Excessive saliva and a hoarse or muffled voice due to throat swelling
- Respiratory Distress Sounds: Rapid, labored breathing with audible wheezing or gasping for air
- Silent Epiglottitis: Rare cases with minimal noise but severe swelling, requiring immediate medical attention
![]()
Stridor in Epiglottitis: High-pitched breathing noise, especially during inhalation, due to upper airway obstruction
Stridor in epiglottitis is a distinctive, high-pitched breathing noise that signals a critical upper airway obstruction. This sound is most pronounced during inhalation, as the inflamed epiglottis narrows the airway, forcing air through a constricted space. Imagine the whistle of wind through a narrow opening—this is the body’s audible distress signal, demanding immediate attention. In children, particularly those aged 2 to 6, this symptom is a red flag, often accompanied by drooling, difficulty swallowing, and a tripod position (sitting upright, leaning forward, with hands on knees) to optimize breathing.
To identify stridor in epiglottitis, listen for a musical, harsh noise that worsens with inspiration. Unlike the soft, wheezing sound of asthma, which is lower in pitch and often expiratory, stridor is sharp and high-pitched, reflecting the upper airway’s involvement. A key differentiator is the location of the obstruction: epiglottitis affects the supraglottic region, while conditions like croup target the subglottic area, producing a barking cough. If stridor is present, especially in a child with fever and throat pain, assume epiglottitis until proven otherwise, as delays in diagnosis can lead to respiratory failure.
Managing a patient with suspected epiglottitis requires caution and swift action. Avoid examining the throat aggressively, as this can provoke complete airway obstruction. Instead, prioritize oxygenation and airway management. Administer high-flow humidified oxygen via a non-rebreather mask to reduce airway edema, and prepare for potential intubation or tracheostomy if the patient decompensates. In severe cases, heliox (a helium-oxygen mixture) may be used to decrease airway resistance, though this is typically a bridge to definitive airway control. Always involve an otolaryngologist and anesthesiologist early in the management process.
Prevention remains the best strategy, particularly through vaccination. Haemophilus influenzae type b (Hib) vaccination has drastically reduced epiglottitis incidence in vaccinated populations, with a 95% efficacy rate in children. Ensure children receive the Hib vaccine series starting at 2 months of age, with boosters as recommended. For adults, especially those with asplenia or immunocompromised states, consider Hib vaccination if not previously immunized. Recognizing stridor as a hallmark of epiglottitis, coupled with timely intervention and preventive measures, can save lives and prevent long-term complications.
Crafting Subnautica's Immersive Audio: A Deep Dive into Sound Design
You may want to see also
Explore related products






![]()
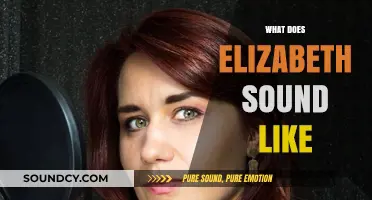
Grunting Sounds: Low-pitched grunting as the body tries to maintain airway pressure against swelling
The body’s struggle to breathe during epiglottitis often manifests as low-pitched grunting, a sound that is both alarming and purposeful. This grunting occurs as the respiratory system works to maintain airway pressure against the swelling of the epiglottis, a flap of tissue that prevents food and liquids from entering the windpipe. Unlike the high-pitched stridor associated with croup, the grunting in epiglottitis is deeper and more labored, reflecting the increased effort required to draw air past the obstruction. This sound is a critical indicator of the condition’s severity and should never be ignored, especially in children, who are more susceptible to rapid airway compromise.
To understand why grunting happens, consider the mechanics of breathing during epiglottitis. As the epiglottis swells, it narrows the airway, forcing the body to generate higher pressure to inhale and exhale. Grunting is a physiological response to this challenge, as the vocal cords partially close during exhalation to create back pressure in the airways. This back pressure helps keep the alveoli in the lungs open, improving oxygen exchange despite the obstruction. While this mechanism is a temporary solution, it is not sustainable and signals an urgent need for medical intervention. Parents and caregivers should be particularly vigilant for this sound in children under 5, as epiglottitis can progress rapidly in this age group.
Recognizing grunting in epiglottitis requires careful observation, as it can be mistaken for other respiratory sounds. Unlike the barking cough of croup or the wheezing of asthma, the grunting here is consistent and low-pitched, often accompanied by drooling, difficulty swallowing, and a tripod position (sitting upright with hands on knees). If you suspect epiglottitis, avoid attempting to examine the throat or administer oral medications, as these actions can worsen the obstruction. Instead, keep the child calm, minimize movement, and seek emergency medical care immediately. Hospitals typically treat epiglottitis with intravenous antibiotics, corticosteroids to reduce swelling, and, in severe cases, intubation to secure the airway.
A practical tip for caregivers is to familiarize themselves with the sounds of common respiratory conditions to differentiate between them. For instance, while croup’s stridor is high-pitched and occurs primarily during inhalation, epiglottitis grunting is low-pitched and persists throughout the breathing cycle. Additionally, monitoring for associated symptoms like fever, restlessness, and cyanosis (blue discoloration of lips or skin) can provide further context. Early recognition of these signs, combined with prompt medical attention, can prevent life-threatening complications. In the case of epiglottitis, time is critical, and grunting serves as a vital auditory cue that demands immediate action.
Effective Steps to Disable Sound Tracker on Your Device Easily
You may want to see also
Explore related products






![]()
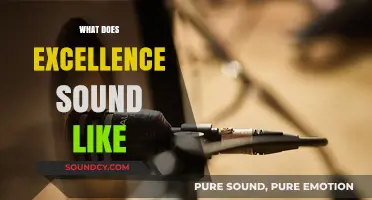
Drooling and Muffled Voice: Excessive saliva and a hoarse or muffled voice due to throat swelling
Epiglottitis often presents with a distinctive combination of symptoms that can be both alarming and indicative of the condition’s severity. Among these, drooling and a muffled voice stand out as key auditory and visual cues. Excessive saliva production, or drooling, occurs because the swelling of the epiglottis and surrounding tissues makes it difficult to swallow. This leads to saliva pooling in the mouth, often resulting in visible drooling, especially in children. Simultaneously, the swelling narrows the airway, causing the voice to become hoarse or muffled, as if speaking through a clogged throat. These symptoms are not merely uncomfortable—they are red flags signaling a potentially life-threatening condition that requires immediate medical attention.
Consider the case of a 4-year-old child with epiglottitis: the child may sit upright, leaning forward slightly, with saliva dripping from their mouth despite attempts to swallow. Their voice, normally clear and high-pitched, becomes distorted, as though they are speaking with a throat full of cotton. This muffled quality is not due to vocal cord damage but rather the obstruction of airflow caused by the swollen epiglottis. Parents or caregivers might notice the child’s voice sounds strained, with words slurred or difficult to articulate. This combination of drooling and voice changes is a critical clue for healthcare providers, who must act swiftly to secure the airway and administer treatment, often starting with intravenous antibiotics and airway management.
To differentiate epiglottitis from other conditions, it’s essential to recognize the context in which these symptoms appear. Unlike drooling caused by teething in infants or a muffled voice from a common cold, epiglottitis symptoms escalate rapidly, often within hours. The drooling is persistent and cannot be controlled, even when the child is at rest. The muffled voice is accompanied by other signs of respiratory distress, such as stridor (a high-pitched breathing sound) and difficulty breathing. For adults, the presentation may be slightly different, with drooling less pronounced but the muffled voice equally concerning. In all cases, the inability to swallow saliva safely and the altered voice quality are telltale signs that demand urgent evaluation.
Practical tips for caregivers include keeping the individual upright to ease breathing and avoiding attempts to examine the throat at home, as this can provoke further swelling. If epiglottitis is suspected, seek emergency care immediately—do not wait for symptoms to worsen. Healthcare providers will typically administer a combination of corticosteroids to reduce swelling, antibiotics to target the infection (commonly *Haemophilus influenzae* type b, or Hib), and, in severe cases, intubation to secure the airway. Early recognition of drooling and a muffled voice can be lifesaving, as prompt treatment significantly improves outcomes and reduces the risk of airway obstruction.
In summary, drooling and a muffled voice in epiglottitis are not isolated symptoms but part of a critical constellation of signs that require immediate action. The excessive saliva and altered voice are direct results of the epiglottis’s swelling, which compromises both swallowing and speech. By understanding these specific manifestations, caregivers and healthcare providers can act swiftly to address the condition, ensuring the best possible outcome for the patient. Recognizing these symptoms is not just about identifying epiglottitis—it’s about responding in time to prevent a medical emergency.
How Does Cabato Bread Sound? Exploring Its Unique Flavor and Texture
You may want to see also
Explore related products






![]()
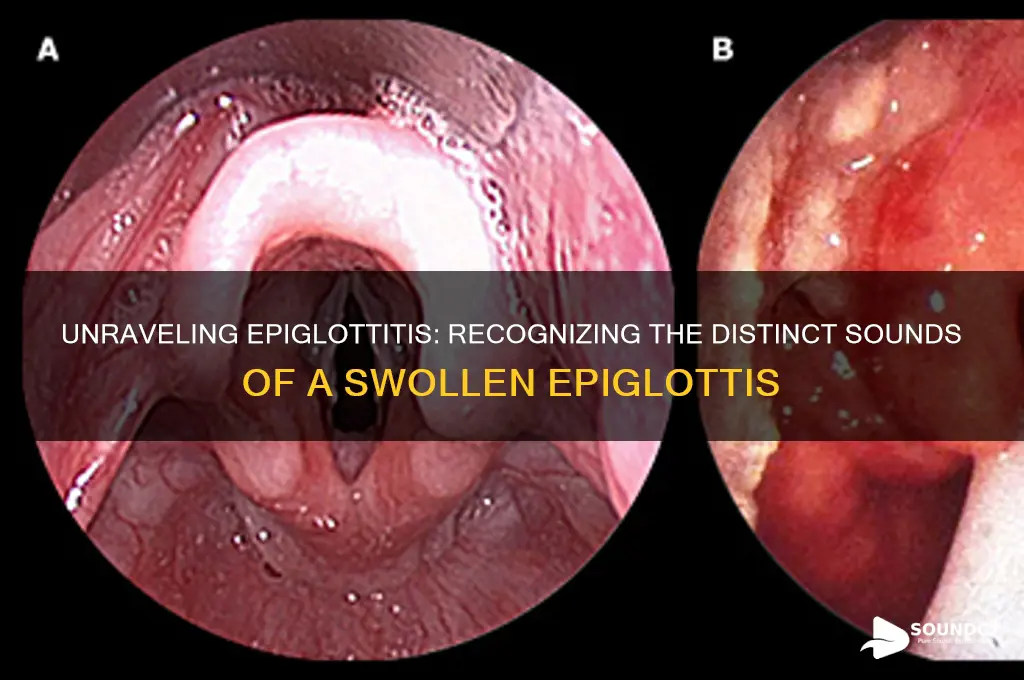
Respiratory Distress Sounds: Rapid, labored breathing with audible wheezing or gasping for air
Epiglottitis, a potentially life-threatening condition, often manifests with distinct respiratory distress sounds that demand immediate attention. Among these, rapid, labored breathing accompanied by audible wheezing or gasping for air is a critical indicator. This combination of symptoms arises from the swelling of the epiglottis, which obstructs the airway, forcing the body to work harder to draw in oxygen. Recognizing these sounds is crucial, as they signal a medical emergency requiring prompt intervention.
In children, particularly those aged 2 to 6, the respiratory distress associated with epiglottitis can be especially pronounced. The rapid breathing, often described as "tripoding" (sitting upright with hands on knees), is a compensatory mechanism to overcome the partial airway blockage. Wheezing, a high-pitched whistling sound, occurs as air struggles to pass through the narrowed passage. Gasping for air, characterized by abrupt, desperate breaths, further underscores the severity of the situation. Parents and caregivers should remain vigilant for these auditory cues, as they often precede more obvious symptoms like drooling or difficulty swallowing.
To differentiate epiglottitis from other respiratory conditions, consider the context and progression of symptoms. Unlike asthma, where wheezing is typically expiratory, epiglottitis often produces inspiratory stridor—a harsh, crowing noise during inhalation. This distinction is vital for healthcare providers during assessment. For instance, a child with epiglottitis may exhibit a "see-saw" pattern of breathing, where the chest retracts with each labored breath. Immediate steps should include keeping the child calm and upright, avoiding any attempts to examine the throat, and seeking emergency medical care without delay.
Practical tips for bystanders include minimizing agitation, as crying or distress can exacerbate airway obstruction. Do not attempt to feed or administer oral medications, as swallowing may become increasingly difficult. Instead, focus on maintaining an open airway and monitoring breathing patterns. For healthcare professionals, early administration of oxygen, corticosteroids to reduce swelling, and antibiotics to address potential bacterial causes are critical interventions. Timely recognition of these respiratory distress sounds can be the difference between a successful outcome and a tragic one.
In summary, the respiratory distress sounds of epiglottitis—rapid, labored breathing with audible wheezing or gasping for air—are a red flag requiring immediate action. Understanding these auditory cues, particularly in high-risk age groups, empowers both caregivers and medical professionals to respond effectively. By staying informed and prepared, we can mitigate the risks associated with this urgent condition and ensure swift, life-saving treatment.
Unveiling the Science Behind Birds' Melodic Vocalizations and Sounds
You may want to see also
Explore related products



![]()
Silent Epiglottitis: Rare cases with minimal noise but severe swelling, requiring immediate medical attention
Epiglottitis, typically characterized by a distinct, high-pitched inspiratory stridor, can occasionally present in a deceptive form known as "silent epiglottitis." Unlike its noisy counterpart, this rare variant produces minimal to no audible symptoms, making it a diagnostic challenge. The absence of stridor, often a red flag for airway obstruction, can lead to delayed recognition and potentially life-threatening complications. This silent progression underscores the importance of recognizing other clinical signs, such as severe throat pain, drooling, and tripod positioning, especially in children and immunocompromised adults.
Consider a case study of a 6-year-old child presenting with fever, difficulty swallowing, and restlessness. Despite the absence of stridor, the child’s neck was visibly swollen, and they were unable to lie flat without distress. Immediate lateral neck X-rays revealed a "thumbprint sign," indicative of epiglottitis. This example highlights how silent epiglottitis demands a high index of suspicion, particularly when typical auditory cues are absent. Clinicians must rely on visual and behavioral indicators, such as muffled voice, agitation, or refusal to eat, to initiate prompt intervention.
The management of silent epiglottitis follows the same urgent protocol as its symptomatic counterpart. Secure airway management is paramount, often requiring intubation in a controlled setting, such as an operating room, to avoid precipitating complete obstruction. Intravenous antibiotics, typically a combination of ceftriaxone (50 mg/kg/day) and vancomycin (40 mg/kg/day), should be administered promptly to target Haemophilus influenzae type b, the most common bacterial culprit. Steroids, like dexamethasone (0.6 mg/kg/dose), may be considered to reduce swelling, though their role remains debated.
Parents and caregivers play a critical role in early detection. Educating them to recognize subtle signs, such as a child’s preference for sitting upright or refusal to swallow, can expedite medical evaluation. In adults, particularly those with comorbidities like diabetes or HIV, unexplained throat pain or respiratory distress warrants immediate attention. Silent epiglottitis serves as a reminder that not all emergencies announce themselves loudly—some require a keen eye and a proactive approach to avert disaster.
In summary, silent epiglottitis defies the auditory stereotypes of this condition, emphasizing the need for a multifaceted diagnostic approach. By focusing on visual, behavioral, and systemic clues, healthcare providers and caregivers can ensure timely intervention, even in the absence of telltale stridor. Awareness of this rare presentation is crucial, as it bridges the gap between silent symptoms and severe consequences, ultimately saving lives.
Customizing PC Audio: Controlling Hardware Sound Modules
You may want to see also
Frequently asked questions
Epiglottitis often causes a high-pitched, muffled sound when breathing, known as stridor, due to swelling of the epiglottis obstructing the airway.
Yes, children with epiglottitis may exhibit stridor, drooling, and a "tripod position" (sitting upright with hands on knees) to ease breathing, along with a muffled or absent cough.
No, epiglottitis typically causes stridor and difficulty breathing, while croup is characterized by a barking cough and a distinct "seal-like" sound when inhaling.