Anisocoria, a condition characterized by unequal pupil sizes, is not something that sounds like anything, as it is a visual phenomenon rather than an auditory one. However, when discussing anisocoria, the focus is typically on its appearance and underlying causes. The condition can result from various factors, including neurological issues, trauma, or medication side effects, and it often requires medical evaluation to determine its origin. While it doesn't produce a sound, understanding anisocoria is crucial for identifying potential health concerns, as it can sometimes indicate serious conditions such as Horner’s syndrome or third nerve palsy.
Explore related products






What You'll Learn
![]()
Normal vs. Abnormal Anisocoria
Anisocoria, the condition where the pupils are different sizes, is often silent—it’s a visual phenomenon, not an auditory one. Yet, understanding its nuances requires a metaphorical "sound check" to distinguish normal from abnormal cases. Normal anisocoria, present in 20% of the population, is subtle and consistent, with a size difference of less than 1 millimeter. It’s like a steady background hum, unremarkable and harmless, often genetic or developmental. Abnormal anisocoria, however, is the alarm bell—sudden, pronounced, or asymmetrical, with a size difference exceeding 1 millimeter. It demands attention, as it may signal underlying issues like nerve damage, trauma, or even a brain aneurysm.
To assess anisocoria, think of it as tuning an instrument. Measure pupil size in both bright and dim light; normal anisocoria remains stable, while abnormal cases may shift dramatically. For instance, a patient with Horner’s syndrome might show anisocoria alongside a drooping eyelid and decreased sweating on one side of the face—a triad that "sounds" distinctly abnormal. Conversely, a simple genetic variation might present as a barely noticeable size difference, akin to a faint off-key note in an otherwise harmonious melody.
Practical tips for differentiation include the "swinging flashlight test." Shine a light into each eye, alternating quickly. In normal anisocoria, both pupils react similarly, like a well-rehearsed duet. In abnormal cases, one pupil may dilate sluggishly or fail to constrict, signaling a disrupted rhythm. For example, Adie’s tonic pupil, a cause of abnormal anisocoria, shows delayed constriction to light, akin to a delayed beat in a song.
Age and medical history are critical context clues. In older adults, mild anisocoria may emerge due to natural pupil atrophy, a soft, gradual change. In younger individuals, especially after head trauma or with symptoms like headache or vision loss, it’s a red flag. For instance, a 30-year-old with sudden anisocoria and severe headache could be experiencing a subarachnoid hemorrhage, requiring immediate medical intervention.
In conclusion, normal anisocoria is the quiet baseline, a benign variation in the body’s design. Abnormal anisocoria, however, is the discordant note that requires investigation. By observing patterns, conducting simple tests, and considering context, you can discern whether the "sound" of anisocoria is a harmless hum or a call to action. Always err on the side of caution—when in doubt, consult a specialist to ensure the melody of health remains unbroken.
Innovative Methods for Efficiently Storing Sound Energy at Home
You may want to see also
Explore related products





![]()
Causes of Unequal Pupil Sizes
Anisocoria, the condition of unequal pupil sizes, can stem from a variety of causes, ranging from benign to life-threatening. Understanding these causes is crucial for accurate diagnosis and timely intervention. One common cause is physiological anisocoria, which affects up to 20% of the population and is typically harmless. In these cases, the size difference between pupils is usually less than 1 millimeter and remains consistent under various lighting conditions. If you notice a slight difference in your pupil sizes that doesn’t change, it’s likely physiological and not a cause for concern.
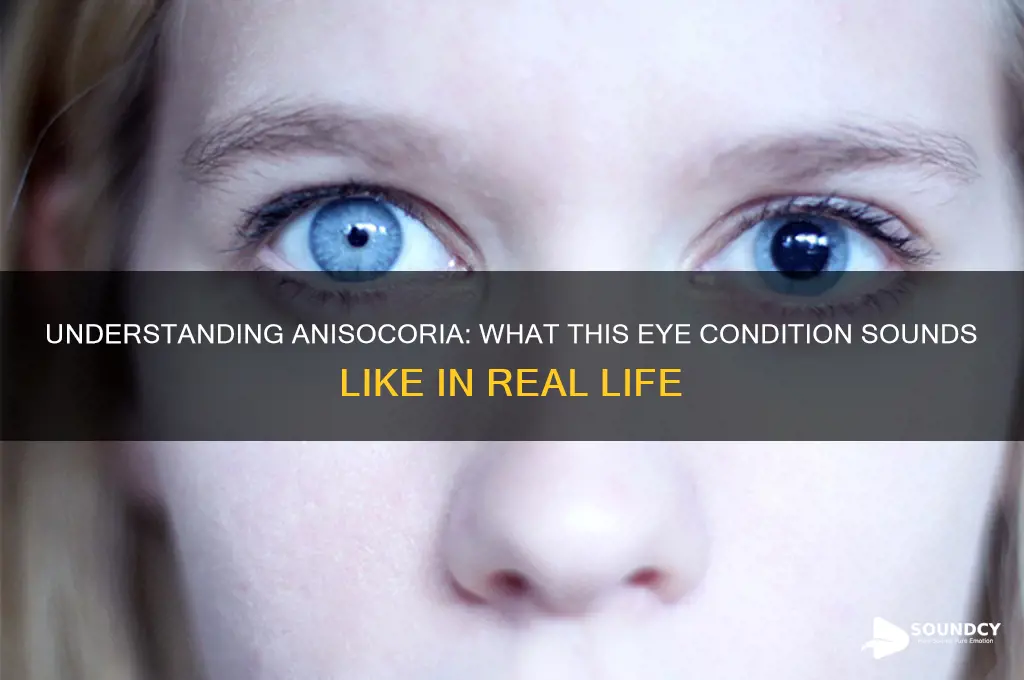
In contrast, pathological anisocoria demands immediate attention, as it may indicate underlying issues such as nerve damage, trauma, or systemic diseases. For instance, Horner’s syndrome, characterized by a smaller pupil on the affected side, can result from damage to the sympathetic nerve pathway. This condition often presents with additional symptoms like ptosis (drooping eyelid) and decreased sweating on the affected side of the face. Another critical cause is third nerve palsy, where damage to the oculomotor nerve leads to a dilated, nonreactive pupil, often accompanied by eyelid drooping and impaired eye movement. If you experience sudden pupil asymmetry alongside these symptoms, seek medical attention promptly.
Medications and substances can also induce anisocoria, making it essential to review your current prescriptions and recent exposures. For example, topical eye drops containing pilocarpine (used for glaucoma) can cause constriction of the pupil, while anticholinergic drugs like atropine may lead to dilation. Even recreational substances, such as cocaine or opioids, can affect pupil size asymmetrically. If you suspect a medication or substance is causing your anisocoria, consult a healthcare provider to adjust your treatment plan or address potential misuse.
Trauma to the eye or head is another significant cause of anisocoria, often resulting from direct injury to the iris sphincter or dilator muscles. In such cases, the pupil on the injured side may appear irregularly shaped or fail to react to light. Immediate evaluation by an ophthalmologist is critical to prevent complications like vision loss or increased intraocular pressure. Protective measures, such as wearing safety goggles during high-risk activities, can reduce the likelihood of traumatic anisocoria.
Finally, systemic diseases like diabetes, multiple sclerosis, or brain tumors can manifest as anisocoria due to their impact on cranial nerves or the autonomic nervous system. For instance, diabetic neuropathy may affect the nerves controlling pupil size, while a brainstem tumor can compress the Edinger-Westphal nucleus, leading to pupillary abnormalities. Regular health screenings and monitoring of chronic conditions can help detect these underlying causes early. If anisocoria develops alongside symptoms like headaches, vision changes, or neurological deficits, it warrants urgent medical evaluation to rule out serious conditions.
Mastering Squirrel Sounds: Techniques to Mimic Their Unique Vocalizations
You may want to see also
Explore related products






![]()
Symptoms and Red Flags
Anisocoria, the condition where the pupils are different sizes, often raises concerns due to its association with underlying health issues. While it may sound like a minor visual discrepancy, the symptoms and red flags demand careful attention. One immediate red flag is sudden onset anisocoria, particularly if accompanied by severe headache, vision changes, or loss of consciousness. These symptoms could signal a neurological emergency, such as a brain aneurysm or stroke, requiring immediate medical intervention.
Analyzing the presentation of anisocoria reveals key distinctions between physiological and pathological causes. Physiological anisocoria, affecting up to 20% of the population, is benign and often consistent in size difference (usually <1 mm). In contrast, pathological anisocoria may exhibit a larger disparity, fluctuating sizes, or reactivity changes to light. For instance, a pupil that fails to constrict in bright light (mydriasis) or dilates excessively in dim light (miosis) warrants investigation. Practitioners should use a penlight to assess pupillary response, noting any asymmetry in constriction or dilation.
Instructively, patients and caregivers should monitor for associated symptoms that escalate concern. These include eye pain, colored halos around lights, reduced vision, or facial drooping. For example, anisocoria paired with ptosis (drooping eyelid) and decreased sweating on the same side of the face suggests Horner’s syndrome, often linked to nerve damage or tumors. Conversely, anisocoria with a fixed, dilated pupil and no reactivity to light may indicate Adie’s tonic pupil, typically benign but requiring confirmation through pharmacological testing.
Persuasively, early recognition of red flags can prevent misdiagnosis and ensure timely treatment. For instance, traumatic anisocoria following a head injury or fall necessitates urgent imaging to rule out intracranial hemorrhage. Similarly, anisocoria in children, especially infants, should never be dismissed, as it could signify congenital conditions like neuroblastoma or retinoblastoma. Parents should document pupil size differences with a flashlight and seek pediatric evaluation if asymmetry persists beyond 3 mm or appears suddenly.
Comparatively, pharmacological causes of anisocoria highlight the importance of medication review. Topical eye drops, such as cyclopentolate or pilocarpine, can induce temporary pupil dilation or constriction, respectively. Systemic medications like anticholinergics or opioids may also affect pupillary size. Patients should inform healthcare providers of recent drug use, including over-the-counter remedies, to differentiate between iatrogenic and organic causes. A detailed history, combined with pupillary examination, remains the cornerstone of diagnosis.
Descriptively, the clinical approach to anisocoria involves a systematic evaluation. Begin with a thorough history, noting onset, duration, and associated symptoms. Follow with a physical exam, including the swinging flashlight test to assess pupillary reactivity. If red flags are present, proceed with neuroimaging (CT or MRI) and laboratory tests to identify underlying conditions. Practical tips include using a ruler to measure pupil size accurately and documenting changes over time. Early intervention, guided by symptom recognition and red flag awareness, can transform a seemingly innocuous finding into a life-saving diagnosis.
Exploring the Phonetic Breakdown of the Word 'Cute' and Its Sounds
You may want to see also
Explore related products






![]()
Diagnostic Tests for Anisocoria
Anisocoria, the condition where the pupils are unequal in size, often raises concerns due to its association with underlying health issues. To determine the cause, a series of diagnostic tests is essential. These tests are designed to differentiate between physiologic anisocoria (benign) and pathologic anisocoria (potentially serious), ensuring appropriate management. Here’s a focused guide on the diagnostic approach.
Step 1: Measure Pupil Size and Reactivity
Begin by measuring both pupils in dim and bright light using a millimeter ruler or a pupillometer. Document the size difference and assess pupillary reactivity to light. Normal physiologic anisocoria typically shows a size difference of less than 1 mm, with both pupils reacting symmetrically to light. If the difference exceeds 1 mm or reactivity is asymmetric, further testing is warranted. For children, age-specific norms apply; for instance, newborns may have pupils ranging from 2 to 4 mm, while older children’s pupils should resemble adult sizes (3–4 mm in ambient light).
Step 2: Perform the Pharmacologic Pupil Test
Administer 1 drop of 1% cocaine or 10% phenylephrine to each eye, observing the pupillary response. In Horner’s syndrome, the affected pupil will dilate minimally or not at all due to sympathetic nerve disruption. Conversely, in Adie’s tonic pupil, the affected pupil will constrict poorly to light but may show slight dilation with cocaine. This test helps localize the lesion to the parasympathetic (Adie’s) or sympathetic (Horner’s) pathways. Note: Cocaine testing is contraindicated in patients with cocaine sensitivity or glaucoma.
Step 3: Assess for Afferent Pupillary Defect (APD)
Use the swinging flashlight test to evaluate for an APD, which suggests optic nerve or retinal pathology. In a dark room, shine a light briefly into one eye, then quickly swing it to the other. In a normal response, both pupils constrict equally. If one pupil dilates instead, it indicates an APD in the eye with the dilating pupil. This test is crucial for identifying conditions like optic neuritis or retinal detachment, which can cause anisocoria secondary to afferent pathway disruption.
Cautions and Considerations
Always consider the patient’s medical history, medications, and recent eye trauma, as these can mimic or exacerbate anisocoria. For example, anticholinergic or cholinergic drugs can alter pupil size and reactivity. In pediatric cases, congenital anomalies like iris coloboma must be ruled out. If pharmacologic testing is inconclusive, neuroimaging (MRI or CT) may be necessary to identify structural abnormalities, such as a brainstem lesion or aneurysm.
Capturing the Explosive Symphony: Describing the Unique Sounds of Fireworks
You may want to see also
Explore related products





![]()
Treatment and Management Options
Anisocoria, the condition where the pupils are unequal in size, often raises concerns about its underlying causes rather than its auditory implications. Since anisocoria itself is silent—a visual phenomenon—the focus shifts to addressing the root issues that may accompany it, such as neurological or ocular disorders. Treatment and management options vary widely depending on the cause, severity, and associated symptoms, requiring a tailored approach for each patient.
Step 1: Identify the Underlying Cause
The first critical step in managing anisocoria is diagnosing its origin. This involves a thorough medical history, neurological examination, and imaging studies like CT or MRI scans. Common causes include Horner syndrome, Adie’s tonic pupil, or third nerve palsy. For instance, Horner syndrome, often linked to a droopy eyelid and decreased sweating, may stem from a tumor or stroke, necessitating urgent intervention. Adie’s tonic pupil, more benign, typically resolves with time but may require cycloplegic eye drops like cyclopentolate 1% to alleviate blurred vision.
Cautions in Treatment
Not all anisocoria cases warrant aggressive treatment. Physiological anisocoria, affecting up to 20% of the population, is harmless and requires no intervention. However, sudden-onset anisocoria, especially when accompanied by headache, eye pain, or vision changes, demands immediate attention. Misdiagnosis or delayed treatment can lead to complications such as permanent vision loss or undiagnosed life-threatening conditions like aneurysms. Avoid self-medication; always consult an ophthalmologist or neurologist for proper evaluation.
Practical Management Tips
For patients with chronic anisocoria, focus shifts to symptom management and quality of life. Tinted glasses or contact lenses can reduce light sensitivity, a common complaint. In cases of Adie’s pupil, reading glasses may improve near vision. Patients with Horner syndrome may benefit from ptosis crutches or surgical intervention for severe eyelid drooping. Regular follow-ups are essential to monitor progression and adjust treatment plans accordingly.
Treating anisocoria is not one-size-fits-all. It requires a blend of diagnostic precision, targeted therapy, and patient education. While the condition itself is silent, its management speaks volumes about the importance of individualized care. By addressing the root cause and alleviating symptoms, healthcare providers can ensure patients not only see better but live better.
Do Skunks Meow? Unraveling the Surprising Sounds of Skunks vs. Cats
You may want to see also
Frequently asked questions
Anisocoria is a visual condition where the pupils of the eyes are unequal in size, so it does not produce a sound. It is observed through physical examination, not heard.
No, anisocoria itself does not cause any audible symptoms. It is a visual condition and does not affect hearing or produce sounds.
No, there is no sound associated with the diagnosis of anisocoria. Diagnosis is based on visual observation of pupil size differences, not auditory cues.
No, anisocoria does not affect speech or how a person sounds. It is a condition related to pupil size and does not impact vocal or auditory functions.