Heart sounds are the audible vibrations produced by the closing and opening of the heart valves, as well as the contraction and relaxation of the heart muscle. These sounds, typically heard through a stethoscope, are crucial in assessing cardiac function and health. The primary heart sounds, S1 and S2, correspond to the closure of the atrioventricular (mitral and tricuspid) and semilunar (aortic and pulmonary) valves, respectively. Additional sounds, such as S3 and S4, may indicate underlying conditions like heart failure or hypertrophy. Understanding these sounds helps healthcare professionals diagnose valvular disorders, arrhythmias, and other cardiovascular issues, making them a fundamental component of clinical cardiac evaluation.
| Characteristics | Values |
|---|---|
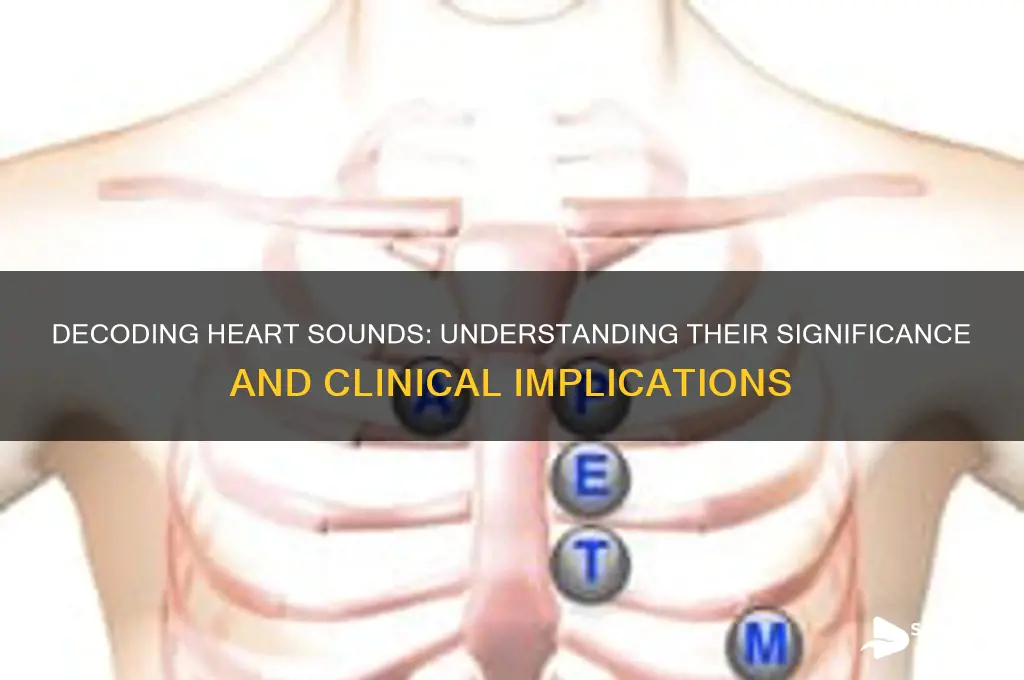
| S1 (First Heart Sound) | Marks the beginning of systole; caused by closure of mitral (M1) and tricuspid (T1) valves; often described as "lub" |
| S2 (Second Heart Sound) | Marks the beginning of diastole; caused by closure of aortic (A2) and pulmonary (P2) valves; often described as "dub"; normally splits into A2 and P2 during inspiration |
| S3 (Third Heart Sound) | Low-pitched, brief sound heard in early diastole; represents rapid filling of ventricles; normal in children, but pathological in adults (e.g., heart failure) |
| S4 (Fourth Heart Sound) | Low-pitched sound heard in late diastole; represents atrial contraction against a stiff ventricle; pathological (e.g., hypertrophic cardiomyopathy, aortic stenosis) |
| Murmurs | Abnormal sounds caused by turbulent blood flow; can be systolic, diastolic, or continuous; graded by intensity (1-6) and described by timing, location, and quality |
| Clicks | Sharp, high-pitched sounds; associated with valve abnormalities (e.g., mitral stenosis, aortic stenosis) |
| Rubs | High-pitched, scratching sounds; indicate pericardial inflammation (pericarditis) |
| Gallop Rhythms | Presence of S3 or S4 creates a triple (S3) or quadruple (S4) rhythm; e.g., S1-S2-S3 ("lub-dub-ta") or S1-S4-S2 ("ta-lub-dub") |
| Split S2 | Normal physiological split during inspiration (A2 and P2 separate); wide or paradoxical splitting indicates pathology (e.g., right bundle branch block, pulmonary hypertension) |
| Ejection Clicks | Heard in systole; associated with valve abnormalities (e.g., aortic stenosis, pulmonary stenosis) |
| Opening Snaps | Heard in diastole; associated with mitral stenosis |
| Timing | S1: onset of systole; S2: onset of diastole; S3: early diastole; S4: late diastole |
| Duration | S1 and S2 are short; murmurs vary in duration; S3 and S4 are brief |
| Pitch | S1 and S2 are medium-pitched; S3 and S4 are low-pitched; murmurs vary (high, medium, or low) |
| Location | S1 best heard at apex (mitral); S2 best heard at base (aortic and pulmonary); murmurs depend on underlying cause |
Explore related products






What You'll Learn
- First and Second Heart Sounds: Represent atrial and ventricular contractions, indicating heart chamber activity during the cardiac cycle
- Murmurs and Abnormal Sounds: Signal valve issues, blood flow turbulence, or structural heart abnormalities requiring medical evaluation
- S3 and S4 Heart Sounds: Indicate ventricular dysfunction, often linked to heart failure or increased filling pressures
- Timing and Pitch Variations: Reflect heart rate, rhythm, and valve competence, aiding in diagnosing arrhythmias or stenosis
- Extra Heart Sounds: Clicks, snaps, or rubs may represent valve abnormalities, pericardial issues, or prosthetic valve function
![]()
First and Second Heart Sounds: Represent atrial and ventricular contractions, indicating heart chamber activity during the cardiac cycle
The rhythmic lub-dub of the heart is more than just a soundtrack to life—it’s a diagnostic goldmine. The first and second heart sounds (S1 and S2) are the cornerstone of cardiac auscultation, each representing distinct phases of the cardiac cycle. S1 corresponds to the closure of the mitral and tricuspid valves, marking the onset of ventricular contraction (systole). S2, on the other hand, signifies the closure of the aortic and pulmonary valves, indicating the end of ventricular ejection and the start of diastole. These sounds are not mere noises; they are audible markers of atrial and ventricular activity, providing critical insights into the heart’s mechanical function.
To appreciate the significance of S1 and S2, consider their timing and quality. S1 is typically low-pitched and prolonged, often described as a "lub," while S2 is higher-pitched and shorter, the "dub." Their split during inspiration in a healthy adult is normal, reflecting the slight delay in pulmonary valve closure compared to the aortic valve. However, a widened or fixed split may indicate conditions like right bundle branch block or atrial septal defect. Clinicians use these nuances to differentiate between physiological variations and pathological abnormalities, making auscultation a vital skill in cardiology.
For healthcare providers, mastering the interpretation of S1 and S2 is essential but requires practice. Start by using a high-quality stethoscope and positioning it correctly over the mitral (fifth intercostal space, midclavicular line) and aortic (second intercostal space, right sternal edge) areas. Listen for the intensity, duration, and splitting of these sounds. For example, a soft S1 may suggest mitral stenosis, while a loud S2 could indicate pulmonary hypertension. Pairing auscultation with other diagnostic tools, such as echocardiography, enhances accuracy, especially in complex cases.
Patients can also benefit from understanding these sounds, as they demystify the cardiac exam process. For instance, explaining that S1 and S2 reflect the heart’s pumping action can alleviate anxiety during a checkup. Parents of children with congenital heart defects can learn to recognize abnormal rhythms, enabling early intervention. While self-diagnosis is never recommended, awareness fosters collaboration between patients and providers, improving overall cardiac care.
In summary, the first and second heart sounds are not just auditory phenomena—they are windows into the heart’s dynamic activity. By representing atrial and ventricular contractions, they offer a non-invasive means to assess cardiac health. Whether you’re a clinician refining your auscultation skills or a patient seeking to understand your heartbeat, S1 and S2 are indispensable tools in the pursuit of cardiovascular wellness.
Memory Foam and Sound Absorption: Fact or Fiction?
You may want to see also
Explore related products






![]()
Murmurs and Abnormal Sounds: Signal valve issues, blood flow turbulence, or structural heart abnormalities requiring medical evaluation
Heart murmurs and abnormal sounds are not merely background noise in a cardiac exam; they are critical indicators of underlying issues that demand attention. These sounds, often described as whooshing or swishing, occur when blood flow through the heart becomes turbulent. Unlike the steady, rhythmic lub-dub of normal heart sounds, murmurs can signal problems such as valve dysfunction, structural abnormalities, or disrupted blood flow. For instance, a systolic murmur might suggest aortic stenosis, where the aortic valve narrows, forcing the heart to work harder to pump blood. Recognizing these sounds is the first step in identifying potentially serious conditions that require medical intervention.
To evaluate murmurs effectively, healthcare providers use a stethoscope to assess their timing, location, intensity, and quality. Systolic murmurs occur during heart contraction, while diastolic murmurs happen when the heart relaxes. The location of the murmur—whether heard best at the apex, base, or mid-chest—can point to specific valve involvement. For example, a murmur heard at the right second intercostal space often indicates aortic valve issues. Grading the intensity of the murmur on a scale of 1 to 6 helps determine its severity, with higher grades suggesting more significant turbulence or obstruction. Understanding these characteristics is essential for distinguishing benign murmurs from those requiring further investigation.
Not all murmurs signify danger; some are innocent or functional, particularly in children and pregnant women. Innocent murmurs are soft, brief, and do not indicate structural abnormalities. However, abnormal murmurs often accompany symptoms like chest pain, shortness of breath, fatigue, or dizziness, which should prompt immediate medical evaluation. Diagnostic tools such as echocardiograms, ECGs, and cardiac MRI can confirm the cause of the murmur and guide treatment. For instance, a patient with a loud, harsh systolic murmur and symptoms of heart failure may require valve repair or replacement to restore normal blood flow.
Preventive measures and early detection play a crucial role in managing conditions associated with abnormal heart sounds. Regular check-ups, especially for individuals with risk factors like hypertension, diabetes, or a family history of heart disease, can identify murmurs before they lead to complications. Lifestyle modifications, such as maintaining a healthy weight, exercising regularly, and avoiding smoking, can reduce the risk of valve disease and blood flow turbulence. For those diagnosed with valve issues, medications like diuretics or beta-blockers may help manage symptoms, but surgical intervention is often necessary for long-term resolution.
In conclusion, murmurs and abnormal heart sounds are not to be ignored. They serve as vital clues to valve dysfunction, blood flow turbulence, or structural abnormalities that require prompt medical attention. By understanding their characteristics, recognizing associated symptoms, and utilizing diagnostic tools, healthcare providers can ensure timely and effective treatment. Patients, too, must remain vigilant and proactive in monitoring their heart health, as early intervention can prevent severe complications and improve quality of life.
Engine Compression and Sound: What's the Link?
You may want to see also
Explore related products






![]()
S3 and S4 Heart Sounds: Indicate ventricular dysfunction, often linked to heart failure or increased filling pressures
Heart sounds, particularly the lesser-known S3 and S4, serve as critical indicators of ventricular dysfunction, often foreshadowing heart failure or increased filling pressures. These extra heart sounds, sometimes referred to as gallops, are not part of the normal lub-dub rhythm (S1 and S2) but rather signal underlying cardiac stress. While S3 is associated with rapid ventricular filling in early diastole, S4 occurs during atrial contraction against a stiff ventricle. Recognizing these sounds is essential for early intervention, as they often precede overt symptoms of heart failure.
To identify S3, listen for a low-pitched "ventricular kick" best heard with the bell of the stethoscope at the apex during early diastole. It is most commonly heard in children and young adults as a benign finding but becomes pathological in older individuals, particularly those with volume overload or reduced ventricular compliance. For instance, patients with dilated cardiomyopathy or severe mitral regurgitation may exhibit an S3 due to increased blood volume returning to the left ventricle. In contrast, S4 is a high-pitched sound occurring just before S1, best detected at the apex with the diaphragm of the stethoscope. It reflects ventricular stiffness, often seen in conditions like hypertension, aortic stenosis, or left ventricular hypertrophy.
Clinicians should approach these sounds with caution, as their presence warrants further investigation. For example, an echocardiogram can assess ventricular function, while BNP or NT-proBNP levels can quantify heart failure risk. Treatment strategies depend on the underlying cause: diuretics for volume overload, ACE inhibitors or beta-blockers for afterload reduction, or lifestyle modifications like sodium restriction and weight management. Early detection of S3 or S4 can significantly alter patient outcomes, delaying progression to advanced heart failure.
Comparatively, while S3 and S4 both indicate diastolic dysfunction, their timing and pathophysiology differ. S3 suggests rapid filling, often due to increased preload, whereas S4 signifies impaired relaxation and compliance. This distinction is crucial for tailored management. For instance, a patient with an S3 might benefit from diuretics to reduce volume, while one with an S4 may require calcium channel blockers to improve ventricular relaxation. Understanding these nuances allows for precise, patient-centered care.
In practice, auscultation remains a cornerstone of cardiac assessment, but it requires skill and experience. For trainees or clinicians less familiar with these sounds, digital stethoscopes or handheld ultrasound devices can aid in detection. Additionally, correlating findings with patient history and risk factors enhances diagnostic accuracy. For example, an elderly patient with hypertension and an S4 is more likely to have left ventricular hypertrophy than a young athlete with an S3, where it might be physiological. By integrating these tools and insights, healthcare providers can effectively identify and manage ventricular dysfunction before it progresses to irreversible heart failure.
Quick Guide: Muting i-Ready Sounds for a Distraction-Free Learning Experience
You may want to see also
Explore related products






![]()
Timing and Pitch Variations: Reflect heart rate, rhythm, and valve competence, aiding in diagnosing arrhythmias or stenosis
The human heart produces a symphony of sounds, each beat a complex interplay of timing and pitch. These variations are not random; they are vital clues to the heart's health. Timing reflects the heart's rhythm, while pitch indicates the competence of its valves. Together, they form a diagnostic duo, revealing conditions like arrhythmias or stenosis with remarkable precision. For instance, a delayed S1 heart sound may suggest mitral valve stenosis, while an irregular rhythm could point to atrial fibrillation. Understanding these nuances is essential for clinicians to differentiate between normal cardiac function and pathological states.
Consider the auscultation process as a detective work. Step 1: Use a stethoscope to listen to the heart sounds at specific locations (aortic, pulmonic, mitral, and tricuspid areas). Step 2: Note the timing of S1 and S2—the first and second heart sounds. A widened split between these sounds may indicate a delay in ventricular contraction, often seen in left bundle branch block. Caution: Environmental noise or patient movement can distort findings, so ensure a quiet setting and proper patient positioning. Step 3: Assess pitch variations. A high-pitched, blowing murmur between S2 and S1 could signify aortic regurgitation, while a low-pitched rumble might indicate mitral stenosis. Practical Tip: Use a sphygmomanometer to correlate murmurs with blood pressure changes for added diagnostic clarity.
From a comparative perspective, timing and pitch variations serve as a cardiac fingerprint, unique to each individual yet consistent within healthy parameters. For example, children and athletes often exhibit faster heart rates with shorter intervals between S1 and S2, reflecting physiological adaptations. In contrast, elderly patients may show prolonged intervals due to age-related stiffening of the heart valves. Takeaway: Context matters. A variation that is normal in one demographic may signal pathology in another. Clinicians must interpret findings within the patient’s age, fitness level, and medical history.
Persuasively, mastering the art of interpreting heart sounds is not just a skill—it’s a necessity. In resource-limited settings, auscultation remains a cost-effective, non-invasive tool for diagnosing cardiac conditions. For instance, detecting a gallop rhythm (S3 or S4) can prompt further investigation into heart failure, even without advanced imaging. Instruction: Practice regularly, using recordings or simulators, to refine your ability to discern subtle changes. Specifics: Aim for at least 10 auscultation sessions weekly to build proficiency. Remember, the heart’s sounds are its language, and fluency in this language can save lives.
Descriptively, imagine the heart as a well-choreographed dance, where timing and pitch are the rhythm and melody. S1, the “lub,” marks the closure of the atrioventricular valves, while S2, the “dub,” signifies the closure of the semilunar valves. When this harmony is disrupted—say, by a harsh, crescendo-decrescendo murmur in systole—it signals aortic stenosis. Analysis: Such murmurs occur due to turbulent blood flow through a narrowed valve, increasing pitch as pressure builds. Conclusion: By translating these auditory cues into clinical insights, healthcare providers can tailor interventions, from medication adjustments to surgical referrals, ensuring optimal patient outcomes.
Unveiling the Science Behind Creating High-Pitched Sounds in Music and Nature
You may want to see also
Explore related products






![]()
Extra Heart Sounds: Clicks, snaps, or rubs may represent valve abnormalities, pericardial issues, or prosthetic valve function
Heart sounds beyond the familiar lub-dub can reveal critical insights into cardiovascular health. Extra sounds like clicks, snaps, or rubs often signal underlying issues, particularly with valves, the pericardium, or prosthetic devices. These sounds are not mere anomalies; they are auditory clues that demand attention and interpretation. Understanding their origins and implications can guide timely interventions and improve patient outcomes.
Consider the mitral valve click, a high-pitched sound often heard in systole. It typically indicates mitral valve prolapse, where the valve leaflets bulge backward into the left atrium. This click is best auscultated at the apex of the heart with the patient in the left lateral decubitus position. While often benign, it warrants monitoring, especially if accompanied by a murmur, as it may suggest significant regurgitation. For instance, in adolescents and young adults, a click without a murmur is usually harmless, but in older adults, it could indicate degenerative valve disease requiring echocardiographic evaluation.
Snaps, on the other hand, are less common but equally significant. A pericardial snap, heard in early diastole, suggests adhesions or inflammation within the pericardium, often due to conditions like pericarditis or prior cardiac surgery. This sound is best detected with the patient leaning forward and exhaling, as it reduces chest wall interference. If a snap is identified, further investigation with imaging, such as a chest X-ray or CT scan, is essential to assess pericardial thickness and potential calcification. Early detection can prevent complications like constrictive pericarditis, which may require pericardiectomy in severe cases.
Rubs are perhaps the most urgent of these extra sounds. A pericardial rub, described as a grating or scratching noise, occurs due to inflamed pericardial layers rubbing against each other. It is typically heard in systole and diastole and is loudest at the lower left sternal border. Patients with a rub often present with chest pain exacerbated by inspiration, fever, and elevated inflammatory markers. Immediate treatment, such as NSAIDs or colchicine, is crucial to reduce inflammation and prevent cardiac tamponade, a life-threatening condition requiring emergency drainage.
Prosthetic valves introduce their own unique sounds. A mechanical valve click, for example, is normal and indicates proper leaflet function. However, changes in click intensity or the emergence of new sounds may suggest valve dysfunction, thrombosis, or paravalvular leak. Patients with mechanical valves require lifelong anticoagulation with warfarin, targeting an INR of 2.0–3.0, to prevent thromboembolic events. Regular auscultation and imaging are vital to ensure optimal function and address complications promptly.
In summary, extra heart sounds are not to be dismissed. Clicks, snaps, and rubs serve as auditory markers of valve abnormalities, pericardial issues, or prosthetic valve function. Recognizing these sounds and their clinical contexts enables healthcare providers to diagnose and manage cardiovascular conditions effectively. Mastery of auscultation techniques, coupled with a systematic approach to patient evaluation, transforms these sounds from mere noises into powerful diagnostic tools.
Mastering Clean Sound Production: Essential Tips for Crisp Audio Quality
You may want to see also
Frequently asked questions
Heart sounds represent the noises produced by the closing of the heart valves and the movement of blood through the heart chambers. They are typically heard as "lub-dub" sounds, with the first sound (S1) representing the closure of the mitral and tricuspid valves, and the second sound (S2) representing the closure of the aortic and pulmonary valves.
Abnormal heart sounds, such as murmurs, clicks, or extra sounds, can indicate underlying heart conditions like valve disorders (e.g., stenosis or regurgitation), congenital heart defects, or issues with blood flow. These sounds are often detected during a physical examination and may require further diagnostic tests.
Heart sounds provide valuable clues about the heart's function and structure. For example, a murmur may suggest valve leakage or narrowing, while a gallop rhythm (extra heart sounds) can indicate heart failure. By analyzing the timing, pitch, and quality of these sounds, healthcare providers can identify potential cardiovascular problems and determine the need for additional testing or treatment.




















