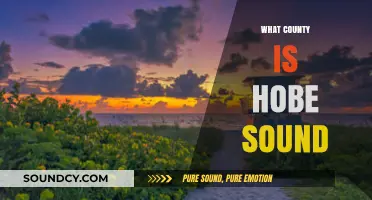
The association between sound and cranial nerves is primarily mediated by the vestibulocochlear nerve, also known as the eighth cranial nerve (CN VIII). This nerve plays a crucial role in both hearing and balance, as it transmits auditory information from the inner ear to the brain. The cochlear branch of CN VIII is responsible for carrying signals related to sound, while the vestibular branch deals with equilibrium. When sound waves reach the inner ear, they stimulate hair cells within the cochlea, which in turn generate electrical signals that travel along the cochlear nerve to the brainstem and ultimately to the auditory cortex, enabling us to perceive sound. Understanding the function of the vestibulocochlear nerve is essential for diagnosing and treating hearing disorders and related conditions.
Explore related products






What You'll Learn
- Vestibulocochlear Nerve (CN VIII): Transmits sound and balance information from the inner ear to the brain
- Cochlear Branch Function: Specifically carries auditory signals from the cochlea to the brainstem
- Auditory Pathway: Sound signals travel from CN VIII to the auditory cortex for processing
- Hearing Loss Causes: Damage to CN VIII can result in sensorineural hearing impairment
- Testing CN VIII: Audiometry and electronystagmography assess the function of this cranial nerve
![]()
Vestibulocochlear Nerve (CN VIII): Transmits sound and balance information from the inner ear to the brain
The Vestibulocochlear Nerve, or CN VIII, is a critical component of our sensory system, serving as the direct link between the inner ear and the brain for both auditory and vestibular functions. This nerve is unique in its dual role: it not only transmits sound information, allowing us to perceive the world around us, but also plays a vital part in maintaining our sense of balance and spatial orientation. Understanding its function is essential for anyone interested in the intricacies of human hearing and equilibrium.
The Journey of Sound: From Ear to Brain
When sound waves enter the ear, they travel through the outer and middle ear, eventually reaching the cochlea in the inner ear. Here, hair cells within the cochlea convert these vibrations into electrical signals. These signals are then relayed to the brain via the cochlear branch of CN VIII. This process is remarkably efficient, enabling us to detect a wide range of frequencies and volumes. For instance, the human ear can perceive sounds as low as 20 Hz and as high as 20,000 Hz, though this range diminishes with age. Practical tip: Regular hearing check-ups, especially after age 50, can help monitor this decline and address issues early.
Balance and Beyond: The Vestibular Connection
While the cochlear branch handles sound, the vestibular branch of CN VIII is responsible for balance. This branch communicates with the semicircular canals and otolith organs in the inner ear, which detect head movements and gravitational forces. This information is crucial for maintaining posture, coordinating movements, and preventing dizziness. For example, conditions like vestibular neuritis, which inflame CN VIII, can cause severe vertigo and imbalance. Caution: If you experience sudden dizziness or hearing loss, seek medical attention promptly, as these could indicate a CN VIII disorder.
Clinical Insights and Practical Applications
Diagnosing issues with CN VIII often involves specialized tests such as audiometry for hearing and electronystagmography (ENG) for balance. Treatments vary depending on the condition; for hearing loss, hearing aids or cochlear implants may be recommended, while vestibular rehabilitation therapy can help manage balance disorders. Interestingly, research shows that certain exercises, like gaze stabilization and balance training, can improve symptoms in patients with vestibular dysfunction. Takeaway: Early intervention and targeted therapy can significantly enhance quality of life for those affected by CN VIII impairments.
Comparative Perspective: CN VIII vs. Other Cranial Nerves
Unlike other cranial nerves that serve specific functions (e.g., CN VII for facial expressions), CN VIII stands out for its dual sensory role. Its complexity underscores the sophistication of the human sensory system. While CN VII and CN IX also have sensory functions, CN VIII’s unique responsibility for both sound and balance highlights its irreplaceable role in our daily lives. This distinction makes it a fascinating subject for both medical professionals and curious minds alike.
In summary, the Vestibulocochlear Nerve is a marvel of human anatomy, bridging the gap between sound perception and spatial awareness. By understanding its function and the conditions that affect it, we can better appreciate the delicate interplay of our senses and take proactive steps to preserve them.
How Fast Does Sound Travel in Knots? Unveiling the Speed
You may want to see also
Explore related products





![]()
Cochlear Branch Function: Specifically carries auditory signals from the cochlea to the brainstem
The cochlear branch of the vestibulocochlear nerve (cranial nerve VIII) is a critical conduit for auditory information, serving as the direct link between the cochlea and the brainstem. This specialized nerve fiber is responsible for transmitting electrical signals generated by the hair cells within the cochlea, which are stimulated by sound waves. Without the cochlear branch, the intricate process of hearing would be severed at its earliest stage, leaving the brain devoid of auditory input. This function underscores its indispensable role in the sensory pathway, making it a focal point in understanding how sound is perceived.
To appreciate the cochlear branch’s function, consider the journey of a sound wave from its entry into the ear to its interpretation by the brain. Once sound reaches the cochlea, it causes the basilar membrane to vibrate, which in turn bends the stereocilia of the hair cells. This mechanical motion is transduced into electrical signals, which are then relayed through the cochlear branch to the cochlear nucleus in the brainstem. This process is remarkably precise, allowing for the discrimination of pitch, volume, and timbre. For instance, high-frequency sounds activate hair cells near the base of the cochlea, while low-frequency sounds stimulate those near the apex, a principle known as tonotopy.
Clinically, damage to the cochlear branch can result in sensorineural hearing loss, a condition where sound reaches the inner ear but is not effectively transmitted to the brain. This can occur due to aging, noise exposure, ototoxic medications, or genetic factors. Diagnostic tools such as audiometry and auditory brainstem response (ABR) testing are used to assess the integrity of the cochlear branch and its pathway. Treatment options vary, ranging from hearing aids and cochlear implants to pharmacological interventions, depending on the underlying cause. Early detection and intervention are crucial, as prolonged deprivation of auditory input can lead to irreversible changes in the auditory cortex.
From a comparative perspective, the cochlear branch’s function highlights the evolutionary sophistication of the auditory system. Unlike simpler sensory systems, such as those for touch or temperature, the auditory pathway requires a high degree of specialization to process the complex, time-sensitive information contained in sound waves. This specialization is evident in the tonotopic organization of the cochlea and the precise synaptic connections within the cochlear nucleus. By contrast, systems like the olfactory nerve rely on a more diffuse coding mechanism, reflecting the different demands of smell versus hearing.
In practical terms, understanding the cochlear branch’s role can inform strategies for hearing conservation and enhancement. For individuals exposed to high noise levels, such as musicians or construction workers, wearing ear protection is essential to prevent mechanical damage to the hair cells and subsequent impairment of the cochlear branch. Additionally, advancements in cochlear implant technology have enabled individuals with severe hearing loss to regain functional hearing by directly stimulating the auditory nerve. These examples illustrate the tangible impact of the cochlear branch’s function on both prevention and rehabilitation in audiology.
Unlocking Optimal Rest: The Ideal Sound Sleep Duration Explained
You may want to see also
Explore related products






![]()
Auditory Pathway: Sound signals travel from CN VIII to the auditory cortex for processing
The auditory system's journey begins with Cranial Nerve VIII, also known as the vestibulocochlear nerve, which plays a pivotal role in our sense of hearing. This nerve is the gateway for sound signals to enter the complex network of the human brain. When sound waves reach the inner ear, they stimulate the hair cells within the cochlea, triggering a cascade of neural events. These hair cells, remarkably sensitive to different frequencies, convert sound vibrations into electrical signals, which are then transmitted via the auditory branch of CN VIII.
The Path Unveiled: Imagine a relay race where the baton is passed from one runner to the next with precision and speed. Similarly, the auditory pathway ensures sound information is swiftly relayed from the ear to the brain. After CN VIII, the signals travel along the cochlear nerve fibers to the cochlear nucleus in the brainstem. Here, the information is processed and relayed to the superior olivary nucleus, which plays a crucial role in localizing sound sources. This processed data then ascends through the lateral lemniscus, a pathway that acts as a highway for auditory signals, leading to the inferior colliculus and, ultimately, the medial geniculate nucleus (MGN) of the thalamus.
In the MGN, the sound signals undergo further refinement and are prepared for the final leg of the journey. From here, the auditory information is projected to the primary auditory cortex, located in the temporal lobe. This cortex is the destination where the magic happens—where sound is perceived, interpreted, and given meaning. The process is remarkably efficient, allowing us to identify and react to sounds in our environment almost instantaneously.
Clinical Insights: Understanding this pathway is not just an academic exercise; it has practical implications in clinical settings. For instance, in cases of hearing impairment, damage to CN VIII or any subsequent structure in the pathway can lead to hearing loss. Audiologists and neurologists often trace the auditory pathway to identify the site of lesions or abnormalities, guiding diagnosis and treatment. Moreover, this knowledge is pivotal in developing hearing aids and cochlear implants, which aim to stimulate the auditory nerve directly or enhance its function.
A Symphony of Sounds: The auditory pathway's elegance lies in its ability to transform mechanical sound waves into a rich auditory experience. From the moment sound enters the ear to its interpretation in the cortex, this journey is a testament to the brain's remarkable capacity for sensory processing. Each step in the pathway contributes to our ability to discern speech, appreciate music, and navigate our environment through sound. Thus, the story of sound's travel from CN VIII to the auditory cortex is not just a biological process but a fundamental aspect of our interaction with the world.
Exploring the Count of Initial Sounds in the English Language
You may want to see also
Explore related products






![]()
Hearing Loss Causes: Damage to CN VIII can result in sensorineural hearing impairment
The vestibulocochlear nerve, or Cranial Nerve VIII (CN VIII), is the unsung hero of our auditory system. It transmits sound and balance information from the inner ear to the brain, enabling us to perceive the world around us. However, when CN VIII is damaged, it can lead to sensorineural hearing loss, a condition that affects millions worldwide. This type of hearing impairment occurs when there is damage to the hair cells in the cochlea or the auditory nerve fibers, disrupting the transmission of sound signals to the brain.
Understanding the Impact of CN VIII Damage
Damage to CN VIII can result from various factors, including aging, exposure to loud noises, ototoxic medications, and head trauma. For instance, prolonged exposure to noise levels above 85 decibels (e.g., concerts, power tools, or heavy traffic) can cause permanent damage to the hair cells in the cochlea. Similarly, certain medications like aminoglycoside antibiotics (e.g., gentamicin) or chemotherapy drugs (e.g., cisplatin) can be toxic to the auditory system, leading to hearing loss. In some cases, CN VIII damage may also be associated with genetic disorders, such as Waardenburg syndrome or Usher syndrome, which affect the development and function of the inner ear.
Diagnosis and Assessment
If you suspect hearing loss due to CN VIII damage, it's essential to consult an audiologist or otolaryngologist for a comprehensive evaluation. This typically involves a series of tests, including pure-tone audiometry, speech discrimination testing, and otoacoustic emissions (OAE) testing. In some cases, imaging studies like MRI or CT scans may be necessary to identify structural abnormalities or damage to the auditory nerve. Early diagnosis is crucial, as it can help prevent further deterioration and guide appropriate management strategies.
Management and Treatment Options
While there is currently no cure for sensorineural hearing loss due to CN VIII damage, several management options can help improve hearing and communication. Hearing aids, for example, can amplify sounds and enhance speech understanding in quiet environments. For more severe cases, cochlear implants may be recommended, which bypass the damaged hair cells and directly stimulate the auditory nerve. Additionally, assistive listening devices (ALDs), such as FM systems or Bluetooth streamers, can help individuals with hearing loss better understand speech in noisy environments. It's worth noting that the effectiveness of these interventions depends on the extent and location of the damage, as well as the individual's age and overall health.
Prevention and Practical Tips
Preventing CN VIII damage is key to maintaining good hearing health. Here are some practical tips to reduce the risk of hearing loss:
- Limit exposure to loud noises, and use earplugs or noise-cancelling headphones when necessary.
- Avoid ototoxic medications or monitor their use under medical supervision.
- Maintain a healthy lifestyle, including regular exercise, a balanced diet, and adequate sleep, to support overall ear health.
- Schedule regular hearing check-ups, especially if you're over 50 or have a family history of hearing loss.
For individuals aged 65 and older, it's recommended to have hearing tests every 1-2 years, as age-related hearing loss (presbycusis) becomes more prevalent. By taking proactive steps to protect your hearing and seeking timely intervention when needed, you can help preserve your auditory function and maintain a high quality of life.
Does SMBus Control Sound? Exploring the Role of SMBus in Audio Systems
You may want to see also
Explore related products






![]()
Testing CN VIII: Audiometry and electronystagmography assess the function of this cranial nerve
Cranial Nerve VIII, also known as the vestibulocochlear nerve, is the primary conduit for auditory and balance information from the inner ear to the brain. Its dual function makes it a critical component in our ability to perceive sound and maintain equilibrium. When assessing the integrity of this nerve, two primary tests stand out: audiometry and electronystagmography (ENG). These methods provide distinct but complementary insights into the nerve’s function, ensuring a comprehensive evaluation of both auditory and vestibular pathways.
Audiometry is the gold standard for testing the auditory component of CN VIII. This non-invasive procedure measures hearing sensitivity across different frequencies, typically ranging from 250 Hz to 8000 Hz. During the test, patients wear headphones and respond to pure tones presented at varying volumes. The results are plotted on an audiogram, which reveals hearing thresholds and identifies potential hearing loss. For example, a patient with sensorineural hearing loss may show elevated thresholds in the high-frequency range, indicating damage to the cochlea or the auditory nerve fibers. Practical tips for accurate testing include ensuring a quiet environment, calibrating equipment regularly, and instructing patients to respond consistently to tones. Audiometry is particularly useful for detecting age-related hearing loss, noise-induced damage, or congenital abnormalities, making it an essential tool for all age groups, from infants to the elderly.
In contrast, electronystagmography (ENG) focuses on the vestibular branch of CN VIII, which is responsible for balance and spatial orientation. This test records involuntary eye movements (nystagmus) in response to stimuli that challenge the vestibular system. The procedure involves placing electrodes around the eyes to measure their movement while the patient undergoes tasks such as tracking a visual target, sitting in darkness, or being irrigated with warm or cold water in the ear canal. For instance, caloric stimulation with water at 30°C and 44°C can elicit nystagmus, which is absent or reduced in patients with vestibular dysfunction. ENG is particularly valuable in diagnosing conditions like Meniere’s disease, labyrinthitis, or vestibular neuritis. However, it requires patient cooperation and can be uncomfortable, especially during caloric testing. Cautions include avoiding testing in patients with severe vertigo or those who cannot remain still for extended periods.
While audiometry and ENG assess different aspects of CN VIII, their combined use offers a holistic evaluation of the nerve’s function. Audiometry provides quantitative data on hearing thresholds, whereas ENG offers qualitative insights into vestibular responses. For example, a patient with normal hearing but abnormal ENG results may have isolated vestibular dysfunction, whereas a patient with hearing loss and normal ENG findings could have cochlear damage without vestibular involvement. This comparative approach allows clinicians to tailor treatment plans, such as recommending hearing aids for auditory deficits or vestibular rehabilitation for balance disorders.
In conclusion, testing CN VIII through audiometry and electronystagmography is a multifaceted process that requires careful consideration of the patient’s symptoms and medical history. Audiometry’s precision in measuring hearing thresholds complements ENG’s ability to assess vestibular function, making them indispensable tools in otolaryngology and neurology. By understanding the strengths and limitations of each test, healthcare providers can accurately diagnose and manage disorders of the vestibulocochlear nerve, ultimately improving patient outcomes. Practical tips, such as ensuring patient comfort during testing and interpreting results in the context of clinical findings, enhance the effectiveness of these assessments. Together, these tests embody the intersection of technology and clinical expertise in evaluating one of the body’s most intricate sensory systems.
Chilling Sounds: The Ultimate Fear Factor
You may want to see also
Frequently asked questions
The vestibulocochlear nerve (cranial nerve VIII) is responsible for transmitting sound information from the inner ear to the brain.
The vestibulocochlear nerve connects to the cochlea in the inner ear, where hair cells convert sound vibrations into electrical signals that are then transmitted to the brain.
Yes, disorders such as auditory neuropathy, Meniere’s disease, and vestibulocochlear nerve damage can affect sound processing and hearing due to issues with cranial nerve VIII.