Sounds from the lungs, such as wheezing, crackling, or stridor, are typically caused by abnormalities in the airways or lung tissue. These sounds occur due to the movement of air through narrowed or obstructed passages, the presence of fluid or mucus in the airways, or inflammation and swelling of lung structures. Conditions like asthma, chronic obstructive pulmonary disease (COPD), pneumonia, bronchitis, or pulmonary edema can lead to these distinctive sounds. Wheezing, for example, often results from constricted airways, while crackling sounds may indicate fluid or mucus accumulation. Understanding the underlying cause of these lung sounds is crucial for accurate diagnosis and effective treatment of respiratory disorders.
| Characteristics | Values |
|---|---|
| Normal Breathing Sounds | Air moving through the tracheobronchial tree (vesicular breathing). |
| Abnormal Sounds | Wheezing, rhonchi, stridor, crackles, pleural friction rub. |
| Wheezing | High-pitched whistling sound due to narrowed airways (e.g., asthma, COPD). |
| Rhonchi | Low-pitched rattling sound from mucus in large airways (e.g., bronchitis). |
| Stridor | High-pitched, inspiratory sound due to upper airway obstruction (e.g., tumor, foreign body). |
| Crackles (Rales) | Discontinuous, bubbling sounds from fluid or mucus in small airways (e.g., pneumonia, heart failure). |
| Pleural Friction Rub | Creaking or grating sound from inflamed pleural surfaces (e.g., pleurisy). |
| Causes of Abnormal Sounds | Infections, inflammation, fluid accumulation, airway obstruction, tumors. |
| Diagnostic Tools | Auscultation with stethoscope, chest X-ray, CT scan, pulmonary function tests. |
| Treatment | Address underlying cause (e.g., bronchodilators for asthma, antibiotics for infections). |
Explore related products






What You'll Learn
![]()
Airflow through narrowed airways (e.g., asthma, COPD)
Narrowed airways, as seen in conditions like asthma and chronic obstructive pulmonary disease (COPD), create a turbulent airflow that generates distinctive lung sounds. This turbulence occurs because the air is forced through a smaller space, increasing its velocity and causing vibrations in the surrounding tissues. These vibrations manifest as wheezing, a high-pitched whistling sound typically heard during exhalation. Wheezing is a hallmark of both asthma and COPD, though its intensity and timing can vary depending on the severity of airway obstruction and the underlying condition.
To understand why narrowed airways produce these sounds, consider the physics of airflow. In healthy lungs, air moves smoothly through open airways, creating minimal noise. However, in asthma, inflammation and bronchoconstriction (tightening of the airway muscles) reduce the airway diameter. In COPD, chronic inflammation and mucus buildup narrow the airways, often irreversibly. As air rushes through these constricted passages, it creates eddies and vortices, similar to the noise produced by wind whistling through a narrow opening. This phenomenon is more pronounced during exhalation because the airways are further compressed by the force of breathing out.
Clinicians often use these sounds as diagnostic clues. For instance, wheezing in asthma is typically responsive to bronchodilators, which relax the airway muscles and widen the passages. In COPD, wheezing may be less responsive to these medications due to the structural changes in the airways. Additionally, the presence of other sounds, such as rhonchi (low-pitched rattling noises caused by mucus in larger airways), can help differentiate between conditions. Patients with asthma may also experience stridor, a high-pitched inspiratory sound, if the upper airways are involved, though this is less common.
Managing airflow through narrowed airways requires a tailored approach. For asthma, short-acting beta-agonists like albuterol (2 puffs every 4–6 hours as needed) provide quick relief by relaxing the airway muscles. Long-term control often involves inhaled corticosteroids (e.g., fluticasone 100–250 mcg twice daily) to reduce inflammation. In COPD, bronchodilators such as tiotropium (18 mcg daily) or combination therapies (e.g., fluticasone/salmeterol) are used to improve airflow. Pulmonary rehabilitation programs, including breathing exercises and physical activity, can also enhance lung function in both conditions.
Practical tips for patients include monitoring peak flow readings to track airway obstruction, avoiding triggers like smoke or allergens, and using spacer devices with inhalers to ensure proper medication delivery. Early recognition of worsening symptoms, such as increased wheezing or shortness of breath, is crucial for preventing exacerbations. By addressing the underlying causes of narrowed airways and optimizing airflow, patients can minimize lung sounds and improve their respiratory health.
Understanding Factors Influencing Sound Frequency: Key Elements Explained
You may want to see also
Explore related products






![]()
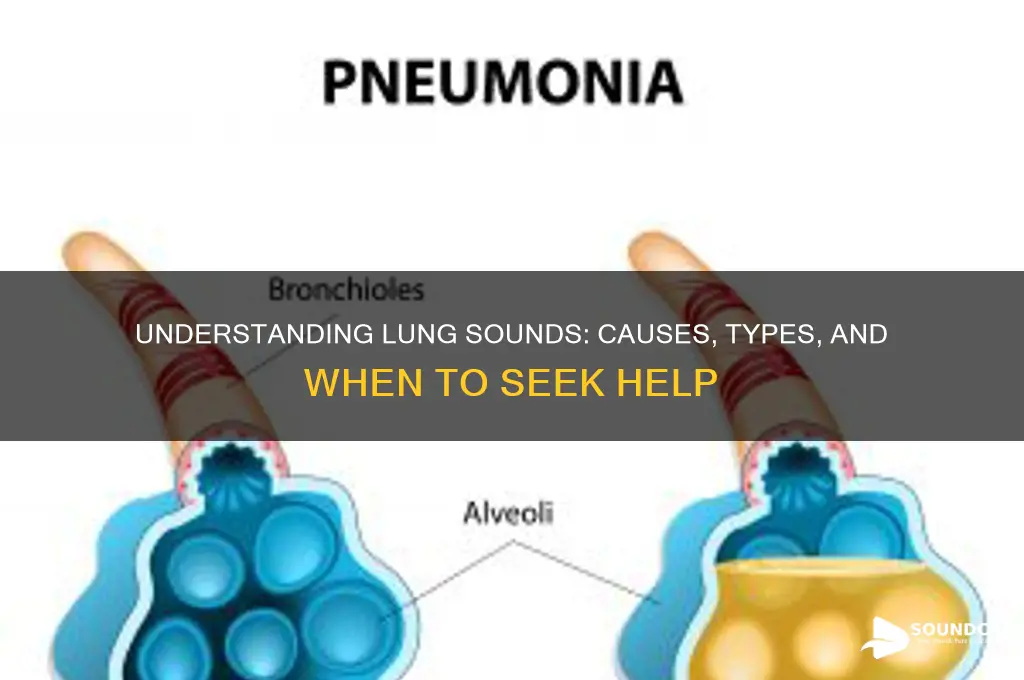
Fluid in alveoli (e.g., pneumonia, pulmonary edema)
Fluid accumulation in the alveoli, the tiny air sacs responsible for gas exchange, disrupts the lungs' normal function and produces distinctive sounds. This condition, often associated with pneumonia or pulmonary edema, fills the airspaces with fluid instead of air, hindering oxygenation. As a result, the lungs emit abnormal sounds during breathing, serving as crucial diagnostic clues for healthcare providers.
Understanding the Mechanism:
Imagine the alveoli as tiny balloons. In a healthy lung, these balloons are inflated with air, allowing for efficient oxygen and carbon dioxide exchange. When fluid fills the alveoli, it's akin to partially filling the balloons with water. This fluid creates a barrier, preventing the alveoli from fully expanding and collapsing normally during breathing. The movement of air through these fluid-filled spaces generates unique sounds, audible through a stethoscope.
In pneumonia, infection causes inflammation and fluid buildup within the alveoli. Pulmonary edema, on the other hand, results from fluid leakage from the blood vessels into the alveoli, often due to heart failure or other conditions. Both scenarios lead to similar auditory manifestations.
Identifying the Sounds:
The characteristic sound associated with fluid in the alveoli is crackles (also known as rales). These are brief, discontinuous sounds that resemble the crackling of velcro or the rustling of leaves. Crackles occur during inspiration (inhaling) as air moves through the fluid-filled alveoli. The intensity and frequency of crackles can vary depending on the severity of the condition. Fine crackles are soft and high-pitched, while coarse crackles are louder and lower-pitched.
Auscultation, the act of listening to the lungs with a stethoscope, is a vital tool for detecting these sounds. Healthcare professionals carefully listen to different lung fields to identify the presence, location, and characteristics of crackles, aiding in diagnosis and monitoring the progression of the underlying condition.
Clinical Significance and Management:
The presence of crackles is a red flag, prompting further investigation into the underlying cause. In pneumonia, treatment typically involves antibiotics to combat the infection, along with supportive care to manage symptoms and ensure adequate oxygenation. For pulmonary edema, addressing the root cause, such as optimizing heart function in heart failure, is crucial. Diuretics may be prescribed to reduce fluid buildup, and oxygen therapy can be administered to support breathing.
Early detection of fluid in the alveoli through auscultation is essential for timely intervention. Recognizing these lung sounds enables healthcare providers to initiate appropriate treatment, preventing complications and promoting recovery. Understanding the link between fluid accumulation and lung sounds empowers both medical professionals and individuals to take proactive steps in managing respiratory health.
Discover the Ultimate Audio File Format for Superior Sound Quality
You may want to see also
Explore related products






![]()
Inflammation of lung tissue (e.g., bronchitis, infections)
Inflammation of the lung tissue, whether from bronchitis, pneumonia, or other infections, often manifests as abnormal lung sounds. These sounds, detected through a stethoscope, include wheezing, crackles, and rhonchi, each signaling distinct airway and tissue involvement. Wheezing, a high-pitched whistling sound, typically indicates narrowed or inflamed airways, common in acute bronchitis. Crackles, resembling the rustling of velcro, suggest fluid or mucus accumulation in the alveoli, often seen in pneumonia. Rhonchi, low-pitched rattling sounds, point to mucus or secretions in larger airways, as in chronic bronchitis. Recognizing these sounds is crucial for diagnosing the underlying cause and guiding treatment.
Consider a patient with acute bronchitis, a viral infection causing inflammation of the bronchial tubes. The inflammation leads to excessive mucus production, which narrows the airways and obstructs airflow. During auscultation, a healthcare provider will hear wheezing, especially during expiration, as air struggles to pass through the constricted passages. Treatment focuses on symptom relief, including bronchodilators to open airways and expectorants to loosen mucus. For adults, a common dosage of guaifenesin (an expectorant) is 200–400 mg every 4 hours, while children’s doses are weight-based, typically 50–100 mg/kg/day. Hydration and rest are equally vital to aid recovery.
In contrast, pneumonia, often bacterial or viral, causes inflammation in the lung’s air sacs, filling them with fluid and pus. This results in crackles, heard during inhalation, as air moves past the fluid-filled alveoli. For bacterial pneumonia, antibiotics are essential; amoxicillin (500 mg every 8 hours for adults) or azithromycin (500 mg on day 1, followed by 250 mg daily for 4 days) are commonly prescribed. Viral cases may require antiviral medications, such as oseltamivir for influenza. Patients should monitor for worsening symptoms, like shortness of breath or high fever, which may indicate complications like sepsis or lung abscess.
Prevention plays a key role in reducing lung inflammation. Annual flu vaccines and pneumococcal vaccines (e.g., PCV13 and PPSV23 for adults over 65) lower infection risks. Avoiding smoking and minimizing exposure to pollutants reduce chronic inflammation, a precursor to conditions like chronic bronchitis. For those with recurrent infections, prophylactic antibiotics or inhaled corticosteroids may be recommended. Practical tips include using a humidifier to ease breathing, practicing deep breathing exercises to clear mucus, and staying updated on vaccinations. Early detection and management of inflammation not only alleviate symptoms but also prevent long-term lung damage.
Comparing acute bronchitis and pneumonia highlights the importance of accurate diagnosis. While both cause inflammation, their treatments differ significantly. Misdiagnosis can lead to unnecessary antibiotic use in viral bronchitis or delayed treatment in pneumonia. Healthcare providers rely on lung sounds, imaging (e.g., chest X-rays), and sometimes sputum cultures to differentiate the conditions. Patients should communicate symptoms clearly, such as the duration of cough, presence of fever, and color of sputum, to aid diagnosis. Understanding these distinctions empowers individuals to seek timely care and follow appropriate treatment plans, ensuring better outcomes and faster recovery.
Capturing Survivor's Audio: Techniques for Authentic and Immersive Sound Design
You may want to see also
Explore related products






![]()
Obstruction in airways (e.g., mucus, foreign bodies, tumors)
Airway obstructions, whether from mucus, foreign bodies, or tumors, can transform the lungs into a cacophony of abnormal sounds. These sounds, audible through a stethoscope, serve as critical clues for healthcare providers diagnosing respiratory issues. Mucus, a common culprit, accumulates in conditions like chronic bronchitis or cystic fibrosis, creating a gurgling or rattling sound known as *rhonchi*. This occurs as air attempts to pass through the narrowed, mucus-filled passages. Foreign bodies, often inhaled accidentally, particularly in children, can cause localized wheezing or stridor, a high-pitched noise resulting from turbulent airflow around the obstruction. Tumors, whether benign or malignant, narrow the airway lumen, producing similar wheezing sounds, though often more persistent and unilateral.
Consider the scenario of a child who inhales a small toy part. The immediate symptom might be sudden coughing or choking, followed by persistent wheezing on one side of the chest. This asymmetry is a red flag, as healthy lungs typically produce symmetrical sounds. In adults, chronic mucus buildup from smoking or COPD can lead to recurrent *rhonchi*, especially during expiration. Tumors, on the other hand, may present with gradual onset of symptoms, including persistent cough, hemoptysis, and unilateral wheezing. Recognizing these patterns is crucial for timely intervention, as untreated obstructions can lead to respiratory distress or failure.
To address airway obstructions effectively, a systematic approach is essential. For mucus-related issues, techniques like chest physiotherapy, postural drainage, and inhaled mucolytics (e.g., hypertonic saline or dornase alfa) can help mobilize secretions. In children with foreign bodies, immediate action is critical; the Heimlich maneuver or, in severe cases, bronchoscopy may be necessary. Tumors require a multidisciplinary approach, often involving surgical resection, chemotherapy, or radiation therapy, depending on the stage and type. For instance, a small, benign tumor might be removed via bronchoscopy, while advanced malignancies may necessitate lobectomy or pneumonectomy.
Prevention plays a key role in minimizing airway obstructions. For mucus-related conditions, quitting smoking, avoiding environmental irritants, and staying hydrated can reduce secretion buildup. Parents should ensure small objects are kept out of reach of young children, who are at highest risk for foreign body aspiration (ages 6 months to 3 years). Regular lung cancer screenings, such as low-dose CT scans for high-risk individuals (e.g., smokers over 50), can detect tumors early, improving treatment outcomes. By understanding the causes and consequences of airway obstructions, individuals and healthcare providers can take proactive steps to maintain lung health and prevent complications.
In summary, airway obstructions from mucus, foreign bodies, or tumors manifest as distinct lung sounds, each requiring tailored management. Early recognition of these sounds, coupled with appropriate interventions, can prevent severe respiratory complications. Whether through lifestyle modifications, emergency procedures, or advanced medical treatments, addressing these obstructions is vital for preserving lung function and overall well-being.
Mastering Sound Previews: A Step-by-Step Guide to Crafting Perfect Clips
You may want to see also
Explore related products






![]()
Abnormal lung tissue movement (e.g., pleural effusion, pneumothorax)
Abnormal lung tissue movement can produce distinctive sounds that signal underlying conditions, often requiring immediate medical attention. Two common culprits are pleural effusion and pneumothorax, both of which disrupt the normal mechanics of breathing. Pleural effusion occurs when excess fluid accumulates in the pleural space, the thin cavity between the lung and chest wall. This fluid acts as a barrier, restricting lung expansion and causing a dampened or absent breath sound on the affected side. Pneumothorax, on the other hand, involves air entering the pleural space, collapsing the lung partially or fully. This results in a hyper-resonant sound upon percussion and diminished breath sounds due to the lung’s inability to expand properly.
To diagnose these conditions, healthcare providers rely on auscultation, percussion, and imaging. During auscultation, a stethoscope reveals decreased or absent breath sounds in pleural effusion, while pneumothorax may present with a complete absence of sounds over the collapsed area. Percussion of the chest wall in pneumothorax produces a hyper-resonant note, akin to tapping an empty container, whereas pleural effusion yields a dull sound, similar to tapping a full water bottle. Imaging, such as chest X-rays or ultrasounds, confirms the diagnosis by visualizing fluid or air in the pleural space. For instance, a chest X-ray in pneumothorax shows a sharp white line (the collapsed lung edge) alongside a dark area (air-filled pleural space), while pleural effusion appears as a hazy opacity obscuring lung tissue.
Treatment for these conditions varies based on severity and underlying cause. Pleural effusion often requires drainage via thoracentesis, a procedure where a needle is inserted into the pleural space to remove fluid. Patients typically receive local anesthesia, and up to 1.5 liters of fluid can be safely removed in a single session, depending on stability. Pneumothorax treatment ranges from observation for small, stable cases to needle decompression or chest tube insertion for larger, symptomatic collapses. In tension pneumothorax, a life-threatening condition where air accumulates under pressure, immediate needle decompression is critical, using a 14-gauge cannula inserted into the second intercostal space at the mid-clavicular line.
Prevention and monitoring are key for individuals at risk. Patients with conditions like COPD, cancer, or trauma history should undergo regular pulmonary assessments. For pneumothorax, avoiding activities that increase intrathoracic pressure, such as heavy lifting or scuba diving, reduces recurrence risk. Pleural effusion prevention focuses on managing underlying diseases, such as heart failure or infections, through medications like diuretics or antibiotics. Early recognition of symptoms—shortness of breath, chest pain, or cough—can lead to timely intervention, minimizing complications like respiratory distress or infection.
In summary, abnormal lung tissue movement due to pleural effusion or pneumothorax manifests as distinct clinical and auditory findings. Prompt diagnosis through physical examination and imaging, coupled with targeted interventions like drainage or decompression, is essential for effective management. Awareness of risk factors and symptoms empowers patients and providers to act swiftly, ensuring better outcomes and reducing the burden of these potentially serious conditions.
Helium's Unique Impact on Sound Production: Exploring the Science Behind It
You may want to see also
Frequently asked questions
Sounds from the lungs, such as wheezing, crackles, or stridor, are often caused by conditions like asthma, bronchitis, pneumonia, or chronic obstructive pulmonary disease (COPD). These sounds occur due to narrowed airways, fluid or mucus buildup, or inflammation in the lungs.
Yes, allergies can trigger asthma-like symptoms, leading to wheezing, while respiratory infections like pneumonia or bronchitis can cause crackles or rattling sounds due to mucus or fluid in the airways.
Mild breathing sounds during intense exercise can be normal, but persistent or unusual sounds, such as wheezing or crackles, may indicate an underlying respiratory issue and should be evaluated by a healthcare professional.