Normal heart sounds are primarily caused by the rhythmic closing and opening of the heart valves as blood flows through the heart chambers. The first heart sound, often described as lub, occurs when the mitral and tricuspid valves close at the beginning of systole, marking the start of ventricular contraction. The second heart sound, or dub, is produced when the aortic and pulmonary valves close at the end of systole, signaling the end of ventricular ejection. These sounds are a result of the pressure changes and vibrations within the blood and surrounding tissues as the valves snap shut. Additionally, the smooth flow of blood and the absence of abnormalities in valve structure or function contribute to the characteristic, healthy heart sounds heard during auscultation.
| Characteristics | Values |
|---|---|
| Source of Sounds | Vibrations caused by the closing of heart valves and blood flow turbulence |
| Heart Valves Involved | Tricuspid, Pulmonic, Mitral, Aortic |
| Normal Heart Sounds | S1 (first heart sound), S2 (second heart sound) |
| S1 (Lub) | Caused by closure of mitral and tricuspid valves; marks beginning of systole |
| S2 (Dub) | Caused by closure of aortic and pulmonic valves; marks beginning of diastole |
| Timing | S1 occurs at the start of systole; S2 occurs at the start of diastole |
| Frequency | S1: Lower-pitched (40-60 Hz); S2: Higher-pitched (60-100 Hz) |
| Duration | S1: Longer (0.10-0.14 seconds); S2: Shorter (0.08-0.12 seconds) |
| Physiological Basis | Valve closure creates vibrations transmitted through blood and tissues |
| Normal Split | Physiological splitting of S2 may occur during inspiration |
| Associated Factors | Heart rate, age, exercise, and respiratory phase influence sound quality |
| Absence of Murmurs | No abnormal sounds or turbulence detected during auscultation |
| Clinical Significance | Normal heart sounds indicate proper valve function and blood flow |
Explore related products






What You'll Learn
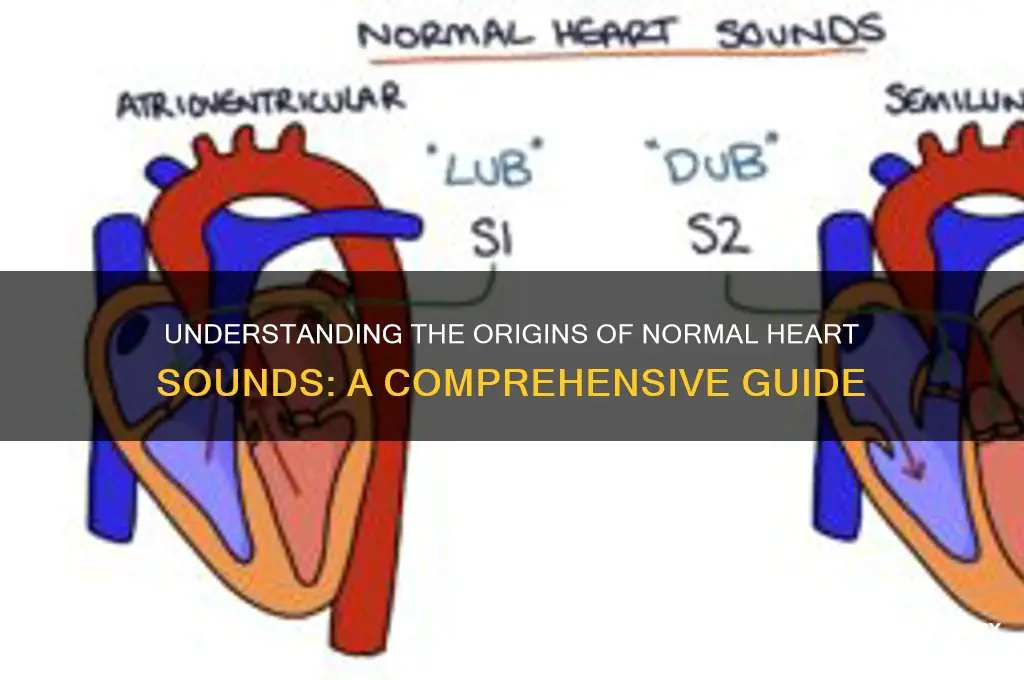
- Ventricular Contraction: Blood ejection creates S1 and S2 heart sounds during systole and diastole
- Valve Closure: Mitral and tricuspid valves close (S1); aortic/pulmonic valves close (S2)
- Blood Flow Velocity: Faster flow increases sound intensity; slower flow reduces it
- Chest Wall Thickness: Thin walls amplify sounds; thick walls muffle them
- Heart Position: Normal cardiac alignment ensures clear, consistent sound transmission
![]()
Ventricular Contraction: Blood ejection creates S1 and S2 heart sounds during systole and diastole
The normal heart sounds, often referred to as the "lub-dub" sounds, are primarily generated by the mechanical events of the cardiac cycle, specifically during ventricular contraction and relaxation. These sounds, known as S1 and S2, are crucial for assessing cardiac function and are directly linked to the ejection of blood from the ventricles. S1, the first heart sound, occurs at the beginning of systole when the ventricles contract. As the ventricles forcefully eject blood into the aorta and pulmonary artery, the atrioventricular (AV) valves (tricuspid and mitral) close abruptly to prevent backflow into the atria. This sudden closure creates a low-pitched sound, often described as the "lub" sound, marking the start of ventricular systole.
The closure of the AV valves is a direct result of the pressure in the ventricles exceeding the pressure in the atria, causing the leaflets of the valves to coapt and shut tightly. This event is essential for ensuring unidirectional blood flow and is the primary mechanism behind the S1 sound. The intensity and quality of S1 can provide valuable clinical information, such as the presence of valve abnormalities or changes in ventricular contractility. For instance, a split S1 may indicate a delay in the closure of one of the AV valves, often seen in conditions like right bundle branch block.
Following systole, the heart transitions into diastole, where the ventricles relax and fill with blood. S2, the second heart sound, occurs at the end of ventricular systole and the beginning of diastole. This sound is produced by the closure of the semilunar valves (aortic and pulmonary) as the pressure in the aorta and pulmonary artery exceeds the pressure in the ventricles. The abrupt closure of these valves prevents backflow into the ventricles and generates a higher-pitched "dub" sound. The timing and characteristics of S2 are influenced by factors such as blood pressure, heart rate, and the compliance of the arterial system.
The ejection of blood during ventricular contraction is the driving force behind both S1 and S2. During systole, the forceful ejection increases ventricular pressure, leading to AV valve closure and the S1 sound. As systole ends, the cessation of ejection causes a drop in ventricular pressure, allowing the semilunar valves to close and produce the S2 sound. This sequence highlights the critical role of blood ejection in creating the normal heart sounds and underscores the importance of ventricular function in the cardiac cycle.
Understanding the relationship between ventricular contraction, blood ejection, and heart sounds is essential for clinical practice. Auscultation of these sounds provides a non-invasive method to evaluate cardiac health and detect abnormalities. For example, changes in the intensity, pitch, or splitting of S1 and S2 can indicate valve disorders, hypertension, or other cardiovascular conditions. By focusing on the mechanics of ventricular contraction and blood ejection, healthcare professionals can better interpret heart sounds and make informed diagnostic decisions. In summary, the normal heart sounds S1 and S2 are directly caused by the ejection of blood during ventricular contraction, with S1 marking the onset of systole and S2 signaling the transition to diastole.
Broadway Theatres: Renting Sound Equipment?
You may want to see also
Explore related products






![]()
Valve Closure: Mitral and tricuspid valves close (S1); aortic/pulmonic valves close (S2)
The first heart sound, denoted as S1, is primarily produced by the closure of the mitral and tricuspid valves. This occurs at the beginning of systole, when the ventricles start to contract. As the ventricular pressure exceeds the atrial pressure, these atrioventricular (AV) valves snap shut to prevent backflow of blood into the atria. The mitral valve, located between the left atrium and left ventricle, and the tricuspid valve, between the right atrium and right ventricle, are composed of leaflets that coapt tightly when closed. This rapid closure creates a vibration in the surrounding structures, including the blood, heart walls, and nearby tissues, which is transmitted as the S1 sound. The S1 sound is typically low-pitched and longer in duration compared to S2, reflecting the forceful closure of these larger valves.
The intensity and quality of S1 are influenced by several factors, including the speed of valve closure, the pressure difference across the valves, and the compliance of the leaflets. During normal cardiac function, the mitral component of S1 is slightly louder than the tricuspid component due to the higher pressure in the left ventricle. Conditions such as mitral stenosis or regurgitation can alter the characteristics of S1, making it softer, louder, or split (heard at different times in the cardiac cycle). Understanding the mechanics of S1 is crucial for diagnosing valvular abnormalities and assessing overall heart function.
The second heart sound, S2, is generated by the closure of the aortic and pulmonic valves at the end of ventricular systole and the beginning of diastole. As the ventricles finish contracting and the pressure in the aorta and pulmonary artery exceeds ventricular pressure, these semilunar valves close to prevent blood from flowing back into the ventricles. The aortic valve, situated between the left ventricle and aorta, and the pulmonic valve, between the right ventricle and pulmonary artery, are designed to close rapidly and efficiently. This closure produces a higher-pitched and shorter sound compared to S1, as the semilunar valves are smaller and close with less force.
The splitting of S2 into two distinct components—aortic (A2) and pulmonic (P2)—is a normal phenomenon that can be heard in many individuals. During inspiration, the decreased intrathoracic pressure causes the pulmonic valve to close slightly later than the aortic valve, resulting in a physiological split. This split becomes more pronounced during deep inspiration and is a useful clinical sign for assessing cardiac timing and pulmonary pressures. Abnormalities in S2, such as a widened or paradoxically split second sound, can indicate conditions like pulmonary hypertension or congenital heart defects.
The coordination between S1 and S2 is essential for maintaining efficient cardiac function. The interval between these sounds corresponds to systole (S1 to S2) and diastole (S2 to the next S1), providing valuable information about heart rate and rhythm. For example, a shortened S1-S2 interval suggests tachycardia or increased ventricular preload, while a prolonged interval may indicate bradycardia or decreased preload. Clinicians often use the timing and characteristics of these valve closure sounds to evaluate cardiac performance and identify potential pathologies.
In summary, the normal heart sounds S1 and S2 are directly caused by the closure of the mitral and tricuspid valves (S1) and the aortic and pulmonic valves (S2), respectively. These sounds are the result of vibrations produced when the valves coapt under pressure, preventing backflow of blood. The distinct qualities of S1 and S2—pitch, duration, and timing—provide critical insights into the mechanical function of the heart and its valves. Understanding the physiology of valve closure is fundamental for interpreting heart sounds and diagnosing cardiovascular conditions.
How to Watch 'Do I Sound Gay' for Free?
You may want to see also
Explore related products

$19.99





![]()
Blood Flow Velocity: Faster flow increases sound intensity; slower flow reduces it
The intensity of heart sounds is closely tied to the velocity of blood flow through the heart and its associated vessels. When blood flows at a higher velocity, it creates more turbulence and kinetic energy, which in turn increases the sound intensity of the heart sounds. This phenomenon is particularly noticeable during systole, when the heart contracts and ejects blood into the aorta and pulmonary artery. As the velocity of blood flow increases, the resulting heart sounds become louder and more distinct, allowing healthcare professionals to assess cardiac function more accurately. For instance, a fast-moving blood stream during ventricular ejection generates the characteristic "lub" sound, known as S1, which is primarily caused by the closure of the atrioventricular (AV) valves.
The relationship between blood flow velocity and sound intensity is governed by the principles of fluid dynamics. As blood accelerates through a narrowing orifice, such as the aortic or pulmonic valves, its velocity increases, leading to a rise in sound intensity. This is because faster-moving blood particles collide more frequently and with greater force, generating acoustic energy that propagates through the chest wall and becomes audible as heart sounds. Conversely, when blood flow velocity decreases, as seen during diastole or in cases of reduced cardiac output, the sound intensity diminishes, resulting in softer or less distinct heart sounds. Understanding this relationship is crucial for interpreting auscultatory findings and identifying potential cardiac abnormalities.
In clinical practice, assessing blood flow velocity indirectly through heart sound intensity helps in evaluating cardiac performance. For example, conditions like aortic stenosis or hypertrophic cardiomyopathy can cause increased blood flow velocity across the aortic valve, leading to louder and more intense ejection sounds. On the other hand, diseases that impair cardiac contractility, such as heart failure, often result in slower blood flow velocities and consequently softer heart sounds. By correlating the intensity of heart sounds with blood flow velocity, clinicians can gain valuable insights into the underlying hemodynamics and structural integrity of the heart.
It is also important to note that blood flow velocity is influenced by factors like stroke volume, vascular resistance, and heart rate. An increase in stroke volume or a decrease in vascular resistance typically elevates blood flow velocity, thereby amplifying heart sound intensity. Conversely, conditions that reduce stroke volume or increase vascular resistance tend to lower blood flow velocity and diminish sound intensity. This interplay between hemodynamic factors and heart sound characteristics underscores the importance of considering blood flow velocity when interpreting auscultatory findings.
In summary, the principle that faster blood flow increases sound intensity while slower flow reduces it is fundamental to understanding normal heart sounds. This relationship is rooted in fluid dynamics and has significant clinical implications for assessing cardiac function. By recognizing how blood flow velocity influences heart sound intensity, healthcare professionals can more accurately diagnose and manage cardiovascular conditions, ensuring optimal patient care.
Understanding Ohm Impedance and Audio Quality
You may want to see also
Explore related products






![]()
Chest Wall Thickness: Thin walls amplify sounds; thick walls muffle them
The thickness of the chest wall plays a significant role in the transmission and perception of heart sounds. Chest wall thickness directly influences how cardiac sounds are amplified or muffled, impacting the auscultation process. Thin chest walls allow for better conduction of sound waves from the heart to the stethoscope, as there is less tissue to attenuate the vibrations. This results in clearer, more distinct heart sounds that are easier for clinicians to interpret. In contrast, thick chest walls act as a barrier, absorbing and dampening the sound waves before they reach the listener’s ear. This muffling effect can make it more challenging to discern the nuances of normal heart sounds, such as the S1 and S2 heart murmurs.
Individuals with naturally thin chest walls, often seen in lean or underweight patients, tend to exhibit amplified heart sounds during auscultation. This amplification occurs because the minimal adipose and muscular tissue between the heart and the stethoscope allows sound waves to travel with minimal interference. Clinicians often find it easier to detect subtle abnormalities or appreciate the quality of heart sounds in such cases. Conversely, patients with thicker chest walls, typically due to increased adipose tissue or muscular build, experience muffled heart sounds. The additional layers of tissue act as a natural sound insulator, reducing the intensity and clarity of the sounds transmitted to the stethoscope.
Understanding the impact of chest wall thickness is crucial for accurate auscultation and diagnosis. Clinicians must adjust their technique when examining patients with thick chest walls, such as applying firmer pressure with the stethoscope or using a bell chest piece to capture lower-frequency sounds. In cases of extreme thickness, additional diagnostic tools like echocardiography may be necessary to overcome the limitations imposed by muffled sounds. Conversely, when assessing patients with thin chest walls, clinicians should be mindful of the amplified sounds and avoid misinterpreting normal variations as pathological murmurs.
The relationship between chest wall thickness and sound transmission highlights the importance of patient-specific auscultation techniques. Thin chest walls enhance sound conduction, making heart sounds more pronounced, while thick chest walls dampen these sounds, requiring careful adjustment of the auscultation approach. This principle underscores why normal heart sounds can vary significantly between individuals based on their anatomical characteristics. By considering chest wall thickness, healthcare providers can improve the accuracy of their cardiac assessments and ensure appropriate patient care.
In summary, chest wall thickness is a critical determinant of how heart sounds are perceived during auscultation. Thin walls amplify sounds, providing clearer auditory cues, whereas thick walls muffle them, necessitating adjustments in technique. Recognizing this relationship enables clinicians to optimize their diagnostic approach, ensuring that normal heart sounds are accurately interpreted across diverse patient populations. This knowledge is essential for anyone involved in cardiac auscultation, from medical students to experienced practitioners.
Highly Sensitive People: Alert to More Than Just Sounds
You may want to see also
Explore related products






![]()
Heart Position: Normal cardiac alignment ensures clear, consistent sound transmission
The position of the heart within the thoracic cavity plays a crucial role in the transmission of normal heart sounds. Normal cardiac alignment refers to the heart’s anatomical position, slightly tilted to the left side of the chest, with its apex resting in the fifth intercostal space. This alignment is essential because it ensures that the heart’s structures—the valves, chambers, and walls—are optimally positioned relative to the chest wall. When the heart is in its normal position, the vibrations generated by the closing of the heart valves (specifically the mitral and tricuspid valves in diastole and the aortic and pulmonary valves in systole) travel efficiently through the chest wall. This alignment minimizes interference from surrounding tissues, such as the lungs or bony structures, allowing for clear and consistent sound transmission to the stethoscope.
The importance of normal cardiac alignment becomes evident when auscultating heart sounds. For instance, the first heart sound (S1), produced by the closure of the mitral and tricuspid valves, is best heard at the apex of the heart. If the heart is not in its normal position, the apex may shift, making S1 more difficult to detect or causing it to sound muffled. Similarly, the second heart sound (S2), resulting from the closure of the aortic and pulmonary valves, is typically heard along the sternum. Misalignment of the heart can alter the pathway of these vibrations, leading to diminished or distorted sounds. Thus, proper cardiac positioning ensures that these sounds are transmitted directly to the appropriate auscultation points, facilitating accurate diagnosis.
Another critical aspect of normal cardiac alignment is its role in maintaining the integrity of the cardiopulmonary relationship. The heart and lungs are closely positioned, and their normal alignment ensures that lung tissue does not excessively dampen heart sounds. In a healthy individual, the lungs act as a medium for sound transmission rather than an obstacle. However, if the heart is displaced—for example, due to conditions like dextrocardia (heart positioned on the right side) or cardiomegaly (enlarged heart)—the additional lung tissue or other structures may interfere with sound transmission. This interference can result in softer or less distinct heart sounds, making it challenging to differentiate between normal and abnormal auscultatory findings.
Furthermore, normal cardiac alignment supports the mechanical efficiency of the heart, which indirectly contributes to clear heart sounds. When the heart is properly positioned, its chambers and valves function optimally, producing consistent and predictable vibrations. For example, the left ventricle, responsible for generating the loudest component of S1, is positioned closest to the chest wall in normal alignment. This proximity ensures that the sound of the mitral valve closing is transmitted clearly. Any deviation from normal alignment can alter the force or direction of these vibrations, affecting the quality of the sounds heard during auscultation.
In clinical practice, understanding the significance of heart position is vital for healthcare providers. During physical examinations, auscultation is performed at specific anatomical landmarks based on the assumption of normal cardiac alignment. If a patient’s heart is not in its typical position, the examiner must adjust their technique to account for the altered anatomy. For example, in patients with right ventricular hypertrophy or lung disease, the heart may shift, requiring auscultation in different intercostal spaces. By recognizing the relationship between heart position and sound transmission, clinicians can ensure accurate interpretation of heart sounds and identify potential underlying cardiac conditions.
In summary, normal cardiac alignment is fundamental to the clear and consistent transmission of heart sounds. It ensures that the heart’s structures are optimally positioned for efficient vibration transmission, minimizes interference from surrounding tissues, and supports the mechanical efficiency of the heart. Clinicians must appreciate this relationship to perform effective auscultation and diagnose cardiac abnormalities accurately. Thus, heart position is not merely an anatomical detail but a critical factor in understanding and assessing normal heart sounds.
How Distance Impacts Sound Level: Understanding the Inverse Square Law
You may want to see also
Frequently asked questions
Normal heart sounds are the noises produced by the closing of the heart valves as blood flows through the heart. They are typically described as "lub-dub" sounds, with the first sound (S1) representing the closure of the mitral and tricuspid valves, and the second sound (S2) representing the closure of the aortic and pulmonary valves.
The first heart sound (S1) is caused by the closure of the mitral and tricuspid valves at the beginning of systole, when the ventricles contract and pump blood out of the heart. This creates a vibration that is heard as the "lub" sound.
The second heart sound (S2) is caused by the closure of the aortic and pulmonary valves at the end of systole, when the ventricles finish contracting and the valves close to prevent backflow of blood. This creates a vibration that is heard as the "dub" sound.
Heart valves produce sounds when they close rapidly, creating a pressure wave that travels through the blood and vibrates the surrounding tissues. These vibrations are transmitted to the chest wall and can be heard using a stethoscope.
Yes, factors like heart rate, blood pressure, and the volume of blood pumped by the heart can affect the intensity and timing of normal heart sounds. For example, a faster heart rate may cause the sounds to be closer together, while high blood pressure can increase the force of the sounds. However, these changes are typically within a normal range and do not indicate a problem unless accompanied by other symptoms or abnormalities.