Heart lub sounds, commonly referred to as heart murmurs, are abnormal whooshing or swishing noises detected during a heartbeat, often caused by turbulent blood flow through the heart valves. These sounds can arise from various factors, including valve abnormalities such as stenosis (narrowing) or regurgitation (leakage), congenital heart defects, or conditions like high blood pressure or anemia that alter blood flow dynamics. Additionally, factors like rapid heart rate, pregnancy, or aging can contribute to the occurrence of these sounds. While some murmurs are harmless, others may indicate underlying heart problems, necessitating further evaluation by a healthcare professional to determine the cause and appropriate management.
| Characteristics | Values |
|---|---|
| Cause | Closure of the atrioventricular (AV) valves (mitral and tricuspid valves) |
| Timing | Beginning of systole (ventricular contraction) |
| Sound Quality | Duller, longer, and lower-pitched compared to the "dub" sound |
| Mechanism | Blood rushes back toward the atria, causing the AV valves to snap shut |
| Associated Conditions | Normal in healthy individuals; abnormalities may indicate valve disorders (e.g., mitral stenosis, tricuspid regurgitation) |
| Diagnostic Relevance | Evaluated during auscultation to assess valve function and cardiac health |
| Frequency | Typically heard as the first heart sound (S1) |
| Duration | Approximately 0.1-0.15 seconds |
| Intensity | Generally louder than the "dub" sound due to higher blood flow velocity |
Explore related products






What You'll Learn
- Ventricular contraction: Blood forcefully ejected from ventricles, creating first heart sound (S1)
- AV valve closure: Tricuspid/mitral valves shut, producing S1's distinctive lub noise
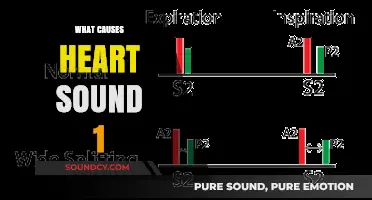
- Semilunar valve closure: Aortic/pulmonic valves close, generating second heart sound (S2)
- Blood turbulence: Flow disruption near valves contributes to audible heart sounds
- Vibrations in tissues: Sound transmission through chest wall amplifies lub-dub sounds
![]()
Ventricular contraction: Blood forcefully ejected from ventricles, creating first heart sound (S1)
The first heart sound, often described as the "lub" in the familiar "lub-dub" rhythm, is a direct consequence of ventricular contraction. This phase, known as systole, begins when the ventricles receive the electrical signal to contract. As the ventricular muscles tighten, they generate immense pressure, forcing blood out of the heart. This forceful ejection is not silent; it creates a distinct sound that resonates through the chest and can be heard with a stethoscope. Understanding this process is crucial for healthcare professionals, as abnormalities in S1 can indicate underlying cardiac issues.
To visualize this, imagine squeezing a water balloon with significant force. The sudden pressure causes the balloon to expel its contents rapidly, creating a sharp, audible release. Similarly, ventricular contraction propels blood into the aorta and pulmonary artery with such force that the atrioventricular (AV) valves—the mitral and tricuspid valves—snap shut. This closure is the primary source of the first heart sound. The timing and quality of S1 provide valuable insights into ventricular function and valve integrity. For instance, a delayed or muffled S1 might suggest impaired contraction or valve dysfunction.
Clinicians often assess S1 during auscultation, paying attention to its intensity, duration, and pitch. A normal S1 is typically low-pitched and lasts about 0.1 seconds. Factors such as heart rate, blood pressure, and age can influence the characteristics of this sound. For example, in children and young adults, S1 is often softer and less pronounced compared to older individuals, where it may become more distinct due to age-related changes in the heart’s structure. Practicing auscultation on diverse patient populations helps refine the ability to differentiate between normal and abnormal S1 sounds.
For those learning to identify S1, a systematic approach is beneficial. Start by locating the mitral area (fifth intercostal space, mid-clavicular line) and the tricuspid area (left sternal border, third intercostal space) using a stethoscope. Listen carefully during systole, focusing on the abrupt, dull sound that marks the beginning of ventricular ejection. Compare findings across patients to build familiarity with variations. Additionally, correlating auscultation with other diagnostic tools, such as echocardiography, can enhance understanding of the relationship between ventricular contraction and S1 production.
In summary, the first heart sound is a direct auditory manifestation of ventricular contraction and AV valve closure. Its characteristics offer a window into cardiac health, making it an essential component of physical examination. By mastering the art of auscultation and understanding the mechanics behind S1, healthcare providers can better diagnose and manage cardiovascular conditions. This knowledge not only improves patient care but also underscores the elegance of the heart’s physiological processes.
Splice Samples: Are They Royalty-Free?
You may want to see also
Explore related products






![]()
AV valve closure: Tricuspid/mitral valves shut, producing S1's distinctive lub noise
The heart's rhythmic "lub-dub" sounds are a symphony of valve closures, each with its own distinct role. The first sound, often described as the "lub," is primarily attributed to the closure of the atrioventricular (AV) valves—the tricuspid and mitral valves. This event marks the beginning of systole, the phase when the ventricles contract to pump blood out of the heart. Understanding this mechanism is crucial for anyone interested in cardiology or simply curious about how the heart functions.
Consider the anatomy: the tricuspid valve separates the right atrium from the right ventricle, while the mitral valve divides the left atrium from the left ventricle. As the atria contract, blood flows into the ventricles, and these valves remain open. However, when the ventricles begin to contract, the pressure in the ventricles exceeds that in the atria, causing the tricuspid and mitral valves to slam shut. This sudden closure prevents backflow of blood into the atria and creates the audible "lub" sound, technically known as the S1 heart sound. The force and timing of this closure are influenced by factors like blood volume, heart rate, and valve integrity.
From a diagnostic perspective, the quality of the S1 sound can reveal much about heart health. A soft or muffled "lub" might indicate mitral stenosis or tricuspid regurgitation, conditions where the valves fail to close properly. Conversely, a loud S1 could suggest volume overload or hypertension, where the heart works harder to maintain circulation. Clinicians often use stethoscopes to assess these sounds, but advanced tools like echocardiograms provide a more detailed view of valve function. For instance, a Doppler echocardiogram can measure blood flow velocity across the valves, helping to quantify any abnormalities.
Practical tips for listening to S1 include placing the stethoscope at the mitral area (fifth intercostal space, midclavicular line) or the tricuspid area (left sternal border, third intercostal space). Patients should be in a supine or left lateral decubitus position to optimize sound detection. For those learning auscultation, recording heart sounds and comparing them to standard examples can be immensely helpful. Apps and online resources often provide audio clips of normal and abnormal S1 sounds, aiding in skill development.
In summary, the "lub" sound of the heart is a direct result of the tricuspid and mitral valves closing at the onset of ventricular contraction. This event is not just a mechanical process but a vital indicator of cardiac health. By understanding its causes and implications, both medical professionals and enthusiasts can better appreciate the intricacies of the cardiovascular system. Whether through auscultation or advanced imaging, listening to the S1 sound offers a window into the heart's dynamic function.
How Sound Travels Over Water: Unraveling the Aquatic Acoustic Mystery
You may want to see also
Explore related products






![]()
Semilunar valve closure: Aortic/pulmonic valves close, generating second heart sound (S2)
The second heart sound, often described as the "dub" in the iconic "lub-dub" rhythm, is a critical marker of cardiac health. This sound is primarily generated by the closure of the semilunar valves—specifically, the aortic and pulmonic valves. Understanding this mechanism is essential for both medical professionals and anyone interested in how the heart functions. When blood is ejected from the ventricles into the aorta and pulmonary artery, these valves snap shut to prevent backflow, creating the audible S2 sound. This process is a testament to the heart’s precision and the importance of valve integrity in maintaining circulatory efficiency.
To visualize this, imagine a high-pressure system where blood is forcefully expelled from the left and right ventricles during systole. Once the ventricles finish contracting, the pressure in the aorta and pulmonary artery exceeds that in the ventricles, causing the aortic and pulmonic valves to slam shut. This closure is abrupt and generates vibrations in the surrounding tissues, which are amplified by the heart’s structure and transmitted to the chest wall. Clinicians use a stethoscope to detect these vibrations, noting the timing and quality of S2 to assess valve function and overall cardiac performance. For instance, a widened splitting of S2 can indicate delayed closure of the pulmonic valve, often seen in conditions like right bundle branch block.
From a practical standpoint, auscultating S2 is a routine part of physical examinations, particularly in pediatric and adult cardiology. In children, a normal S2 is typically single, as the aortic and pulmonic components are closely aligned. However, in adults, respiratory variations can cause S2 to split into two distinct components during inspiration, a phenomenon known as physiological splitting. Pathological conditions, such as pulmonary hypertension or aortic stenosis, can alter S2’s characteristics, making it a valuable diagnostic tool. For example, a loud, palpable S2 may suggest hypertension, while a muffled sound could indicate valve dysfunction.
For those learning auscultation, focusing on the timing and intensity of S2 relative to the heart cycle is crucial. Place the stethoscope over the second intercostal space (aortic area) and third left sternal border (pulmonic area) to isolate the components of S2. Practice on diverse patients to recognize normal variations and abnormalities. Remember, S2 occurs at the end of systole, marking the transition to diastole, so correlate it with the pulse to refine your timing. This skill is not just academic—it’s a lifeline in emergencies, where rapid assessment of valve function can guide critical interventions.
In summary, semilunar valve closure is the unsung hero of the cardiac cycle, producing the second heart sound that clinicians rely on for diagnosis. By understanding the mechanics of S2, from its physiological basis to its clinical implications, one gains deeper insight into cardiovascular health. Whether you’re a medical student, practitioner, or curious learner, mastering this concept enhances your ability to interpret the heart’s language, ensuring better patient care and outcomes.
Mastering the British Accent: Tips to Sound Authentically English
You may want to see also
Explore related products






![]()
Blood turbulence: Flow disruption near valves contributes to audible heart sounds
The rhythmic 'lub-dub' of the heart is a symphony of fluid dynamics, where blood turbulence plays a pivotal role in creating these audible cues. As the heart contracts and relaxes, blood flow accelerates and decelerates, particularly near the valves. This rapid change in velocity causes disruptions, leading to turbulent flow—a key contributor to the heart sounds we hear. Understanding this phenomenon not only sheds light on cardiac physiology but also highlights the importance of turbulence in diagnosing heart conditions.
Consider the mitral valve during ventricular contraction. As blood rushes from the left atrium to the left ventricle, it encounters a narrowing at the valve opening. This constriction accelerates flow, creating a pressure gradient that can lead to turbulence. The resulting vibrations, amplified by the surrounding tissues, manifest as the first heart sound (S1), or the 'lub.' Similarly, during ventricular relaxation, the aortic valve closes to prevent backflow, causing turbulence as blood momentarily reverses direction. This disruption generates the second heart sound (S2), or the 'dub.' These sounds are not mere byproducts of circulation but critical indicators of valve function and blood flow efficiency.
To visualize this, imagine water flowing through a hose with a partially closed nozzle. The restriction increases velocity, creating turbulence that produces a distinct noise. In the heart, this turbulence is more complex due to the non-linear geometry of valves and the pulsatile nature of blood flow. Advanced imaging techniques, such as echocardiography with Doppler flow studies, can quantify turbulence by measuring flow velocities and pressure gradients across valves. For instance, a peak velocity of >2 m/s across the aortic valve suggests significant turbulence and potential stenosis, warranting further evaluation.
Clinicians leverage this understanding to diagnose valvular disorders. For example, a harsh, crescendo-decrescendo murmur heard between S1 and S2 may indicate aortic stenosis, where turbulence is heightened due to a narrowed valve. Conversely, a softer, blowing murmur in the same window could point to aortic regurgitation, where turbulence arises from blood flowing backward. Practical tips for auscultation include using the diaphragm of the stethoscope for low-pitched sounds (like S1) and the bell for higher-pitched murmurs, ensuring accurate detection of turbulence-related abnormalities.
In summary, blood turbulence near heart valves is not a flaw but a feature—one that translates flow disruptions into audible signals. By studying these sounds, healthcare providers can non-invasively assess cardiac health, emphasizing the interplay between fluid dynamics and clinical diagnosis. Whether in a routine checkup or a specialized cardiac evaluation, the 'lub-dub' remains a testament to the heart’s intricate design and the turbulence that gives it voice.
Top Soundproofing Materials: Discover What Blocks Sound Best for Quiet Spaces
You may want to see also
Explore related products





![]()
Vibrations in tissues: Sound transmission through chest wall amplifies lub-dub sounds
The heart's iconic lub-dub sounds originate from the closing of valves during the cardiac cycle, but these subtle vibrations require amplification to become audible. This is where the chest wall steps in, acting as a natural resonator. As the heart contracts and relaxes, it generates low-frequency vibrations that travel through surrounding tissues. The chest wall, composed of skin, fat, muscle, and bone, effectively transmits and amplifies these vibrations, making them detectable by the human ear or a stethoscope. This process highlights the interplay between the heart's mechanical activity and the body's anatomical structures in producing the familiar heartbeat sounds.
To understand this phenomenon, consider the physics of sound transmission. Vibrations from the heart's valves are initially low in amplitude and frequency, typically ranging between 20 to 100 Hz. When these vibrations reach the chest wall, the denser tissues, particularly the ribs and sternum, act as a soundboard, enhancing the energy of the waves. This amplification is crucial because the human ear is less sensitive to low frequencies, and without this natural boost, the lub-dub sounds would be imperceptible. Stethoscopes further capitalize on this principle by funneling and amplifying these vibrations, allowing healthcare providers to assess cardiac function.
Practical implications of this sound transmission are evident in clinical settings. For instance, the clarity of heart sounds can vary depending on the patient's body habitus. Individuals with a thinner chest wall or less adipose tissue may exhibit louder and more distinct lub-dub sounds, while those with obesity might have muffled or softer sounds due to increased tissue damping. Clinicians must account for these variations when auscultating, adjusting their technique by applying varying pressure with the stethoscope to optimize sound transmission. This underscores the importance of understanding the role of tissue vibrations in cardiac auscultation.
A comparative analysis reveals that other body sounds, such as lung crackles or bowel movements, also rely on tissue transmission but differ in frequency and source. Heart sounds, however, are unique in their reliance on the chest wall for amplification due to their low frequency. This distinction is why stethoscopes are designed with specific materials and shapes to enhance low-frequency sound transmission. For example, electronic stethoscopes often include filters to amplify these frequencies, making them particularly useful in noisy environments or for patients with challenging acoustics.
In conclusion, the lub-dub sounds of the heart are not merely a product of valve closure but a result of intricate sound transmission through the chest wall. This process transforms faint vibrations into audible signals, enabling diagnosis and monitoring of cardiac health. By appreciating the role of tissue vibrations and the chest wall's amplifying properties, healthcare providers can refine their auscultation skills and better interpret heart sounds. This knowledge also highlights the elegance of the human body's design, where even the simplest sounds carry profound diagnostic value.
Does Tesla Sentry Mode Include Sound Alerts? Exploring Features and Functionality
You may want to see also
Frequently asked questions
The first heart sound (S1) is caused by the closure of the atrioventricular (AV) valves—the mitral valve on the left side and the tricuspid valve on the right side. This occurs when the ventricles contract (systole), creating a "lub" sound as the valves snap shut to prevent blood from flowing back into the atria.
The second heart sound (S2) is caused by the closure of the semilunar valves—the aortic valve on the left side and the pulmonary valve on the right side. This occurs when the ventricles finish contracting and begin to relax (diastole), creating a "dub" sound as these valves close to prevent blood from flowing back into the ventricles.
Heart lub sounds (S1 and S2) are typically normal and indicate the proper functioning of the heart valves. However, changes in the intensity, timing, or splitting of these sounds can indicate underlying issues, such as valve disorders (e.g., stenosis or regurgitation), heart murmurs, or other cardiovascular conditions. A healthcare professional should evaluate any abnormal sounds.