An S4 heart sound, often described as a late diastolic gallop, is caused by the forceful contraction of a stiff or hypertrophied left ventricle against a higher than normal volume of blood. This occurs when the left atrium contracts to push blood into the left ventricle, but the ventricle is already filled to a greater extent due to conditions such as hypertension, aortic stenosis, or left ventricular hypertrophy. The increased pressure and stiffness of the ventricular wall result in the characteristic low-pitched, rumbling sound, which is best heard at the cardiac apex with the patient in the left lateral decubitus position. Identifying an S4 sound is clinically significant as it often indicates underlying cardiac pathology and may prompt further evaluation for heart failure, valvular disease, or systemic hypertension.
| Characteristics | Values |
|---|---|
| Definition | S4 heart sound is a low-pitched sound occurring in late diastole, often described as a "presystolic gallop." |
| Timing | Heard just before the first heart sound (S1), during the atrial contraction phase. |
| Causes | - Reduced ventricular compliance (e.g., due to hypertension, left ventricular hypertrophy). - Increased blood volume in the ventricles (e.g., due to anemia, hyperthyroidism). - Ventricular stiffness (e.g., from ischemia, cardiomyopathy). - Conditions causing increased filling pressures (e.g., heart failure, mitral or aortic regurgitation). |
| Associated Conditions | Hypertension, left ventricular hypertrophy, ischemic heart disease, cardiomyopathy, anemia, hyperthyroidism, heart failure. |
| Clinical Significance | Often indicates decreased ventricular compliance or increased filling pressures, suggesting underlying cardiac dysfunction. |
| Diagnostic Tools | Auscultation with a stethoscope, echocardiography, ECG, and other imaging studies. |
| Treatment | Address underlying cause (e.g., managing hypertension, treating anemia, optimizing heart failure therapy). |
| Prognosis | Depends on the underlying condition; may indicate advanced cardiac disease if untreated. |
Explore related products






What You'll Learn
- Left ventricular hypertrophy: Thickened heart muscle increases stiffness, delaying filling and causing S4 sound
- Hypertension effects: Chronic high blood pressure leads to ventricular stiffness, producing an S4 sound
- Ischemic heart disease: Reduced blood flow to the heart causes stiffening, resulting in an S4 sound
- Aortic stenosis: Obstructed aortic valve increases ventricular pressure, leading to S4 sound development
- Infiltrative cardiomyopathy: Conditions like amyloidosis cause ventricular stiffness, generating an S4 sound
![]()
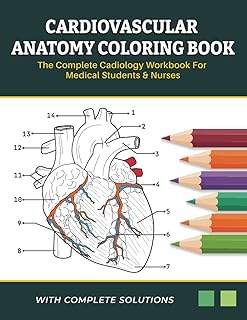
Left ventricular hypertrophy: Thickened heart muscle increases stiffness, delaying filling and causing S4 sound
The S4 heart sound, often described as a late diastolic "atrial kick," is a subtle yet significant marker of cardiac dysfunction. Among its causes, left ventricular hypertrophy (LVH) stands out as a critical contributor. LVH occurs when the muscle wall of the heart’s main pumping chamber thickens, typically in response to prolonged pressure overload, such as hypertension. This thickening increases the stiffness of the left ventricle, impairing its ability to relax and fill with blood during diastole. As a result, the atria must contract more forcefully to push blood into the ventricle, producing the audible S4 sound.
To understand the mechanism, consider the normal cardiac cycle. During diastole, the left ventricle should passively fill with blood, aided by atrial contraction. In LVH, the thickened muscle resists this filling, delaying the process. The atria compensate by contracting harder, creating a vibration that manifests as the S4 sound, typically heard best at the cardiac apex with the patient in the left lateral decubitus position. This sound is often described as low-pitched and brief, following the third heart sound (S3) if present.
Clinically, identifying an S4 sound in a patient with LVH is a red flag, signaling advanced cardiac remodeling. It suggests that the heart is struggling to maintain adequate filling pressures, often due to long-standing hypertension or aortic stenosis. For example, a 55-year-old patient with untreated hypertension may present with LVH and an S4 sound, indicating a need for aggressive blood pressure management. Medications like ACE inhibitors or beta-blockers can reduce afterload, slowing the progression of LVH and potentially reversing the S4 sound over time.
Practical tips for healthcare providers include using a diaphragm stethoscope to detect the S4 sound, as it is more sensitive to low-frequency sounds. Patients should be instructed to avoid excessive salt intake and adhere to antihypertensive therapy to prevent further LVH. Regular echocardiograms can monitor wall thickness and diastolic function, providing objective data to guide treatment. Early intervention is key, as prolonged LVH with an S4 sound increases the risk of heart failure, arrhythmias, and sudden cardiac death.
In summary, LVH-induced S4 is a mechanical consequence of a stiff, thickened left ventricle. It serves as both a diagnostic clue and a call to action, urging clinicians to address the underlying cause and prevent further cardiac deterioration. By recognizing this sound and its implications, healthcare providers can implement targeted therapies to improve patient outcomes and reduce cardiovascular risk.
Cork's Acoustic Magic: Unveiling Its Sound-Absorbing Properties and Benefits
You may want to see also
Explore related products





![]()
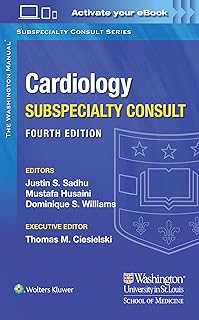
Hypertension effects: Chronic high blood pressure leads to ventricular stiffness, producing an S4 sound
Chronic hypertension silently remodels the heart, turning its once-pliable ventricles into rigid chambers. This stiffness impairs the heart’s ability to fill with blood during the atrial contraction phase, a process critical for maintaining cardiac output. As the left ventricle struggles to accommodate incoming blood, it generates an abnormal, low-pitched sound known as S4. This gallop rhythm, often described as a “Tennessee” gallop, signals advanced cardiac strain and is a late-stage marker of untreated high blood pressure.
To understand the mechanism, consider the heart’s diastolic phase. Normally, the ventricle relaxes and expands effortlessly, but chronic hypertension thickens the ventricular walls (left ventricular hypertrophy). This hypertrophy reduces compliance, forcing the atria to work harder to push blood into the ventricle. The resulting S4 sound occurs just before the first heart sound (S1), creating an audible “a-t” rhythm. Clinicians detect this using a stethoscope over the mitral area, often in patients with long-standing hypertension aged 50 and older.
Preventing S4 begins with blood pressure management. Guidelines recommend maintaining systolic/diastolic pressure below 130/80 mmHg for most adults, particularly those with cardiovascular risk factors. Lifestyle modifications—reducing sodium intake to <2,300 mg/day, engaging in 150 minutes of moderate exercise weekly, and limiting alcohol—are foundational. For pharmacological intervention, ACE inhibitors, beta-blockers, or calcium channel blockers may be prescribed, tailored to patient comorbidities and tolerance. Regular monitoring, including echocardiograms to assess ventricular function, is essential for early detection of hypertrophy.
The presence of S4 is a red flag, indicating not just hypertension but potential progression to heart failure. Patients with this finding often require aggressive management, including diuretics to reduce preload and afterload-reducing agents. A multidisciplinary approach, involving cardiologists, dietitians, and physical therapists, optimizes outcomes. For example, a 60-year-old with a 10-year history of uncontrolled hypertension (160/95 mmHg) and new-onset S4 might benefit from a regimen of lisinopril 20 mg daily, spironolactone 25 mg, and a low-sodium DASH diet, alongside biweekly cardiac rehab sessions.
In summary, S4 is not merely a sound but a symptom of systemic cardiac deterioration driven by hypertension. Its emergence demands immediate intervention, combining medical therapy, lifestyle adjustments, and vigilant monitoring. By addressing the root cause—chronic high blood pressure—clinicians can halt ventricular stiffening, preserve cardiac function, and avert the cascade to heart failure. Early recognition and action are paramount; S4 is a warning, not a verdict.
Mastering the Art of the 'T' Sound: Tips and Techniques for Clear Pronunciation
You may want to see also
Explore related products




![]()
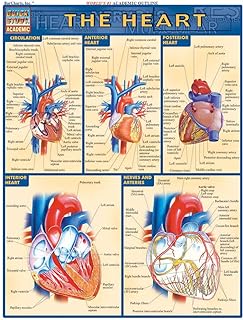
Ischemic heart disease: Reduced blood flow to the heart causes stiffening, resulting in an S4 sound
The S4 heart sound, often described as a late diastolic "atrial gallop," is a subtle yet significant marker of cardiac dysfunction. Among its various causes, ischemic heart disease stands out as a critical contributor. This condition, characterized by reduced blood flow to the heart muscle, triggers a cascade of events that ultimately lead to the stiffening of the ventricles. As the heart struggles to compensate for inadequate oxygen supply, the left ventricle thickens, a process known as hypertrophy. This stiffening impairs the heart’s ability to relax and fill properly during diastole, generating the audible S4 sound as blood forcefully enters the less compliant ventricle.
To understand the mechanism, consider the heart’s normal diastolic phase: blood flows passively from the atria to the ventricles. In ischemic heart disease, however, the ventricle’s reduced elasticity causes resistance, forcing the atria to contract with greater pressure. This additional effort produces the low-pitched S4 sound, typically heard just before the first heart sound (S1). Clinicians often detect this using a stethoscope, placing it over the mitral area with the patient in the left lateral decubitus position. The presence of an S4 is a red flag, warranting further investigation into underlying coronary artery disease or other ischemic conditions.
From a diagnostic perspective, identifying an S4 sound in a patient with suspected ischemic heart disease is a critical step. It often prompts additional tests such as an electrocardiogram (ECG), echocardiogram, or stress test to assess myocardial perfusion. For instance, an echocardiogram can reveal ventricular hypertrophy and reduced diastolic function, corroborating the auscultatory findings. Early detection is key, as untreated ischemia can progress to heart failure or myocardial infarction. Lifestyle modifications, such as a heart-healthy diet, regular exercise, and smoking cessation, are foundational. Pharmacological interventions, including antiplatelet agents (e.g., aspirin 81 mg daily), statins, and beta-blockers, may also be prescribed to manage risk factors and improve outcomes.
Comparatively, while other conditions like hypertension or aortic stenosis can also cause an S4 sound, ischemic heart disease is unique in its direct link to coronary artery pathology. Hypertension, for example, primarily induces left ventricular hypertrophy through chronic pressure overload, whereas ischemia results from episodic or chronic oxygen deprivation. This distinction highlights the importance of targeted treatment strategies. In ischemic cases, revascularization procedures like angioplasty or coronary artery bypass grafting (CABG) may be necessary to restore blood flow and alleviate ventricular stiffness.
In practical terms, patients with ischemic heart disease should monitor symptoms such as chest pain, shortness of breath, or fatigue, which may accompany the S4 sound. Regular follow-ups with a cardiologist are essential to track disease progression and adjust treatment plans. For healthcare providers, educating patients about the significance of an S4 sound can foster early intervention and better adherence to therapy. By addressing the root cause—reduced blood flow—clinicians can mitigate ventricular stiffening and improve long-term cardiac function, ultimately reducing the morbidity associated with this condition.
Sound Speed Unveiled: How Fast Does Sound Travel in FPS?
You may want to see also
Explore related products



![]()
Aortic stenosis: Obstructed aortic valve increases ventricular pressure, leading to S4 sound development
The S4 heart sound, often described as a late diastolic "atrial gallop," is a clinical marker of ventricular dysfunction. Among its causes, aortic stenosis stands out as a primary culprit. This condition occurs when the aortic valve narrows, obstructing blood flow from the left ventricle to the aorta. As a result, the left ventricle must generate higher pressures to eject blood, leading to hypertrophy and stiffening of the ventricular wall. This increased stiffness impairs the ventricle’s ability to relax during diastole, causing elevated atrial pressures as the left atrium works harder to fill the ventricle. The forceful contraction of the atrium against this resistance produces the audible S4 sound, typically heard just before the first heart sound (S1).
To diagnose aortic stenosis-induced S4, clinicians rely on a combination of auscultation and imaging. During auscultation, the S4 sound is best heard at the cardiac apex with the patient in the left lateral decubitus position. It is often described as a low-pitched, dull thud, distinct from the sharper S1. Echocardiography is essential for confirming the diagnosis, as it visualizes the obstructed aortic valve, measures valve gradients, and assesses left ventricular hypertrophy. In severe cases, the mean transvalvular pressure gradient exceeds 40 mmHg, and the aortic valve area falls below 1 cm². Early detection is critical, as untreated aortic stenosis can progress to heart failure, arrhythmias, or sudden cardiac death.
From a pathophysiological perspective, the development of an S4 sound in aortic stenosis reflects a compensatory mechanism gone awry. Initially, left ventricular hypertrophy helps maintain stroke volume despite the obstructed valve. However, as the ventricle becomes increasingly stiff, diastolic filling is compromised, leading to elevated left atrial pressures and the S4 sound. This progression underscores the importance of monitoring patients with aortic stenosis, even in asymptomatic stages. For instance, adults over 65 with a history of hypertension or bicuspid aortic valve should undergo regular echocardiographic screening, as these factors predispose to stenosis.
Management of aortic stenosis-related S4 focuses on addressing the underlying valve obstruction. In symptomatic patients or those with severe stenosis, aortic valve replacement (AVR) is the definitive treatment. Surgical AVR remains the gold standard, but transcatheter aortic valve replacement (TAVR) offers a less invasive option for high-risk patients. Post-procedure, patients often experience resolution of the S4 sound as ventricular pressures normalize. However, lifelong monitoring is necessary to assess for complications such as valve degeneration or paravalvular leaks. For asymptomatic patients with moderate stenosis, guidelines recommend serial echocardiograms every 6–12 months to track disease progression and guide timely intervention.
In summary, the S4 sound in aortic stenosis is a direct consequence of ventricular stiffening and impaired diastolic filling caused by an obstructed aortic valve. Recognizing this auscultatory finding prompts critical diagnostic and therapeutic actions, from echocardiographic evaluation to timely valve replacement. By understanding the mechanistic link between aortic stenosis and S4, clinicians can improve patient outcomes and prevent the progression to advanced heart failure. This underscores the importance of integrating clinical auscultation with advanced imaging to manage this prevalent valvular disorder effectively.
How Thick Foam Rubber Dampens Sound
You may want to see also
Explore related products





![]()
Infiltrative cardiomyopathy: Conditions like amyloidosis cause ventricular stiffness, generating an S4 sound
An S4 heart sound, often described as a late diastolic "atrial gallop," is a clinical sign that can point to significant underlying cardiac issues. Among the various causes, infiltrative cardiomyopathies, particularly amyloidosis, stand out due to their unique mechanism of ventricular stiffening. Unlike conditions such as hypertension or aortic stenosis, where the S4 results from increased left ventricular pressure, amyloidosis causes the heart muscle to become rigid due to the deposition of abnormal proteins. This stiffness impairs ventricular relaxation, forcing the atria to contract with greater force against the resistant ventricle, producing the audible S4 sound.
Amyloidosis, a disorder characterized by the extracellular deposition of amyloid fibrils, infiltrates the myocardium, leading to diastolic dysfunction. The accumulation of these fibrils disrupts the normal architecture of the heart muscle, rendering it less compliant. As a result, the ventricle struggles to fill adequately during diastole, a process that is further exacerbated by the increased atrial effort required to overcome the stiffness. Clinicians often detect this as an S4 sound, which is best heard at the cardiac apex with the patient in the left lateral decubitus position. Recognizing this sound in the context of amyloidosis is crucial, as it may prompt further diagnostic evaluation, such as echocardiography or cardiac MRI, to confirm the infiltrative process.
Diagnosing amyloidosis-related S4 requires a systematic approach. Patients may present with nonspecific symptoms like fatigue, shortness of breath, or peripheral edema, making the S4 sound a valuable clue. Laboratory tests, including serum and urine protein electrophoresis, can identify abnormal protein deposits, while tissue biopsy remains the gold standard for confirmation. Treatment focuses on managing the underlying condition, with options ranging from chemotherapy for light-chain amyloidosis to supportive care for transthyretin-related amyloidosis. Emerging therapies, such as tafamidis, have shown promise in slowing disease progression, particularly in hereditary forms.
For healthcare providers, the presence of an S4 sound in a patient with suspected infiltrative cardiomyopathy should trigger a high index of suspicion for amyloidosis. Early detection and intervention are critical, as untreated ventricular stiffness can progress to heart failure. Patients should be monitored for signs of worsening cardiac function, such as weight gain, worsening edema, or new-onset arrhythmias. Education about the condition and its implications is equally important, empowering patients to recognize symptoms and seek timely medical attention. By understanding the link between amyloidosis, ventricular stiffness, and the S4 sound, clinicians can improve diagnostic accuracy and patient outcomes in this complex disease.
How Sound Waves Travel Through Different Mediums Explained
You may want to see also
Frequently asked questions
An S4 heart sound, also known as a fourth heart sound or atrial gallop, is an extra heart sound that occurs immediately before the first heart sound (S1). It is often described as a low-pitched "thud" and is typically heard in individuals with certain cardiac conditions.
An S4 heart sound is usually caused by a stiff or non-compliant left ventricle, which impairs its ability to fill properly during diastole. This can be due to conditions such as hypertension, left ventricular hypertrophy, ischemic heart disease, or aortic stenosis.
An S4 heart sound is typically diagnosed through a physical examination using a stethoscope. It is best heard at the cardiac apex, with the patient in the left lateral decubitus position and during expiration. Additional diagnostic tests, such as echocardiography or electrocardiography, may be performed to identify the underlying cause.
The presence of an S4 heart sound often indicates diastolic dysfunction or elevated left ventricular filling pressures. It may be a sign of underlying cardiac conditions, such as heart failure, ischemic heart disease, or valvular heart disease. Further evaluation and management are necessary to address the underlying cause and prevent complications.