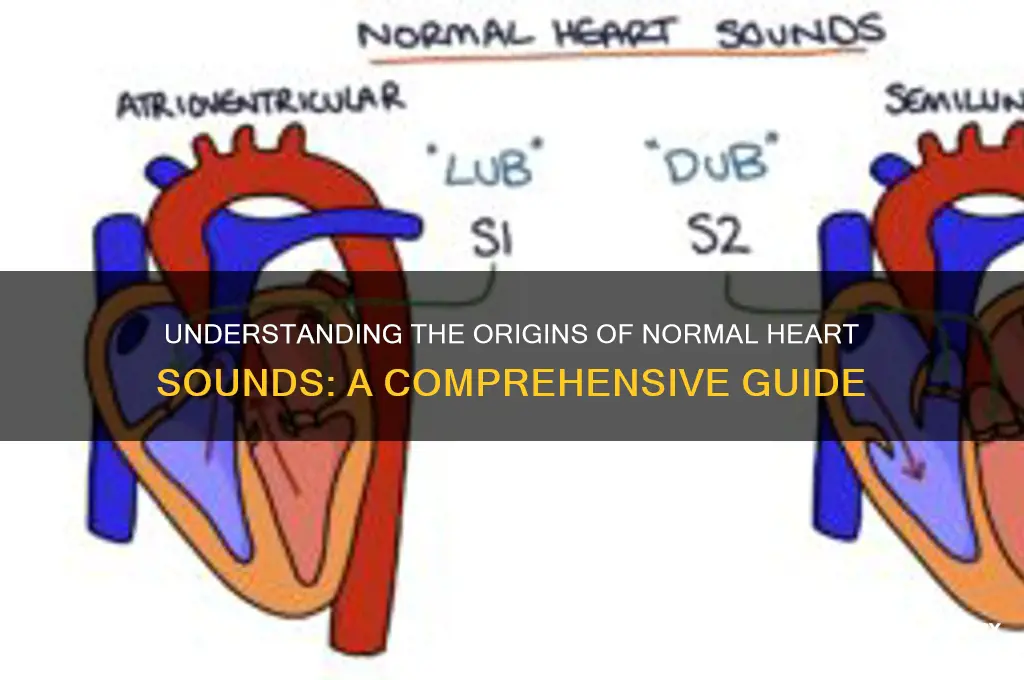
Normal heart sounds are primarily caused by the rhythmic contraction and relaxation of the heart's valves as blood flows through its chambers. The two distinct sounds, often described as lub-dub, correspond to the closing of the atrioventricular valves (mitral and tricuspid) during systole, producing the first heart sound (S1), and the closing of the semilunar valves (aortic and pulmonary) during diastole, creating the second heart sound (S2). These sounds are a result of the turbulent blood flow and the sudden cessation of backflow when the valves close, amplified by the heart's structures and transmitted through the chest wall. Understanding these mechanisms is essential for diagnosing cardiovascular health, as abnormalities in heart sounds can indicate underlying cardiac conditions.
| Characteristics | Values |
|---|---|
| Cause of Sounds | Vibrations produced by the closing and opening of heart valves. |
| First Heart Sound (S1) | Caused by closure of the mitral and tricuspid valves (AV valves). |
| Second Heart Sound (S2) | Caused by closure of the aortic and pulmonary valves (semilunar valves). |
| Timing | S1 occurs at the beginning of systole; S2 occurs at the start of diastole. |
| Pitch | S1 is lower pitched (duller); S2 is higher pitched (sharper). |
| Duration | S1 is longer in duration; S2 is shorter. |
| Physiological Basis | Sounds result from turbulent blood flow and valve leaflet movement. |
| Normal Rhythm | Lub-dub pattern (S1-S2) repeated with each heartbeat. |
| Frequency Range | S1: 20–60 Hz; S2: 60–100 Hz. |
| Associated Factors | Heart rate, blood pressure, and valve integrity influence sound quality. |
| Clinical Significance | Normal sounds indicate healthy valve function and cardiac physiology. |
Explore related products






What You'll Learn
- Ventricular Contraction: Blood ejection creates S1 and S2 heart sounds during systole
- Valve Closure: Mitral and tricuspid valves close, producing the S1 sound
- Semilunar Valves: Aortic and pulmonary valves close, generating the S2 sound
- Blood Flow Turbulence: Laminar flow through valves and vessels contributes to normal sounds
- Chest Wall Transmission: Heart sounds travel through tissues to auscultation sites
![]()
Ventricular Contraction: Blood ejection creates S1 and S2 heart sounds during systole
The rhythmic lub-dub of a healthy heart is a symphony of precision, orchestrated by the contraction and relaxation of cardiac muscles. At the core of this auditory performance is ventricular contraction, a powerful event that propels blood into circulation and generates the iconic S1 and S2 heart sounds. These sounds, often likened to the closing of mitral and tricuspid valves (S1) and the aortic and pulmonary valves (S2), are not mere byproducts but essential markers of cardiac efficiency. Understanding their origin during systole—the heart’s ejection phase—offers a window into the mechanics of life itself.
Consider the sequence: as the ventricles contract, blood is forcefully ejected into the aorta and pulmonary artery. This ejection slams shut the atrioventricular valves (mitral and tricuspid), producing the S1 sound, often described as a deep "lub." The intensity of S1 is influenced by factors like blood volume, valve integrity, and contraction force. For instance, a hyperdynamic state, such as in athletes or during pregnancy, amplifies S1 due to increased stroke volume. Conversely, conditions like mitral stenosis may mute or split the sound. Clinicians often use the quality of S1 to assess ventricular function, making it a critical diagnostic tool.
Following S1, the semilunar valves (aortic and pulmonary) close as ventricular pressure drops below arterial pressure, creating the S2 sound, or the crisp "dub." The timing and pitch of S2 are particularly revealing. A widened splitting of S2, for example, can indicate delayed closure of the pulmonary valve, seen in conditions like right bundle branch block. Age also plays a role: in children, S2 is typically single due to simultaneous closure of both valves, while in adults, respiratory variations cause splitting. Auscultating S2 with precision requires attention to these nuances, ensuring accurate interpretation of cardiac health.
To effectively evaluate these sounds, follow a structured approach: position the patient in a supine or left lateral decubitus position, use a diaphragm for S1 and a bell for S2, and listen at the appropriate valve areas. Note the duration, intensity, and quality of each sound. For instance, a harsh, loud S1 may suggest mitral valve prolapse, while a soft, high-pitched S2 could indicate aortic stenosis. Pairing auscultation with echocardiography or ECG enhances diagnostic accuracy, especially in complex cases.
In practice, recognizing the interplay between ventricular contraction and heart sounds is indispensable. For medical professionals, it’s a skill honed through repetition and vigilance. For patients, understanding these sounds demystifies the heartbeat, fostering a deeper appreciation for cardiac health. Whether in a bustling ER or a quiet clinic, the S1 and S2 sounds remain steadfast indicators of the heart’s tireless work, a testament to the elegance of human physiology.
The Fading Sound of Running Feet
You may want to see also
Explore related products





![Normal Heart [Blu-ray]](https://m.media-amazon.com/images/I/919FZ1uGbdL._AC_UY218_.jpg)
![]()
Valve Closure: Mitral and tricuspid valves close, producing the S1 sound
The first heart sound, S1, is a critical marker of cardiac health, produced by the closure of the mitral and tricuspid valves. This event occurs at the beginning of systole, when the ventricles contract and force blood into the aorta and pulmonary artery. The abrupt halt of blood flow causes these valves to snap shut, generating a distinctive low-pitched "lub" sound. Clinicians rely on this sound to assess the timing and integrity of valve function, as deviations can indicate conditions like mitral stenosis or tricuspid regurgitation.
To understand S1, consider the mechanics of valve closure. The mitral valve, situated between the left atrium and ventricle, and the tricuspid valve, between the right atrium and ventricle, are designed to prevent backflow during systole. When ventricular pressure exceeds atrial pressure, these valves close simultaneously, creating a pressure wave that propagates through the heart and chest wall. This wave is what auscultation captures as S1. For healthcare providers, the quality and intensity of this sound offer insights into valve leaflet mobility, chordal integrity, and overall cardiac performance.
Auscultation techniques play a pivotal role in evaluating S1. Positioning the diaphragm of a stethoscope at the apex of the heart (fifth intercostal space, midclavicular line) optimizes detection of the mitral component, while placement at the left sternal border (third intercostal space) highlights the tricuspid component. Patients should be in a supine or left lateral decubitus position to enhance sound transmission. Abnormalities, such as a split S1 (common in right bundle branch block) or a muffled sound (suggestive of fluid accumulation), warrant further investigation via echocardiography or electrocardiography.
For individuals monitoring their heart health, recognizing the significance of S1 is essential. While self-auscultation is impractical, understanding that this sound reflects valve function can motivate proactive care. Regular check-ups, especially for those with risk factors like hypertension or diabetes, ensure early detection of valve-related issues. Lifestyle modifications, such as maintaining a healthy weight and avoiding smoking, can reduce the strain on these valves, preserving their function and the clarity of S1.
In summary, the closure of the mitral and tricuspid valves, producing S1, is a fundamental aspect of cardiac physiology. Its assessment through auscultation provides a non-invasive window into heart function, guiding both diagnosis and preventive care. By appreciating the mechanics and clinical implications of this sound, healthcare providers and patients alike can better navigate the complexities of cardiovascular health.
Do Blackout Curtains Block Sound? Exploring Their Acoustic Benefits
You may want to see also
Explore related products


![The Normal Heart [DVD] (English audio. English subtitles)](https://m.media-amazon.com/images/I/81LB4hsk75L._AC_UY218_.jpg)
![Normal Heart [DVD] [2014] [Region 1] [US Import] [NTSC]](https://m.media-amazon.com/images/I/81ADi9uZBzL._AC_UY218_.jpg)

![The Normal Heart [DVD] [2014]](https://m.media-amazon.com/images/I/51oOEU9MbrL._AC_UY218_.jpg)
![]()
Semilunar Valves: Aortic and pulmonary valves close, generating the S2 sound
The second heart sound, S2, is a critical marker of cardiac function, produced by the closure of the semilunar valves—specifically, the aortic and pulmonary valves. This sound occurs at the end of ventricular systole, marking the transition to diastole. Understanding the mechanics behind S2 is essential for clinicians and medical students alike, as it provides insights into the timing and efficiency of blood flow through the heart. For instance, a normally split S2 is heard in healthy individuals, with the aortic component (A2) following the pulmonary component (P2) due to the higher pressure in the aorta. This split becomes more pronounced during inspiration, a physiological phenomenon that aids in differentiating it from pathological murmurs.
To appreciate the significance of S2, consider the anatomical and physiological interplay of the semilunar valves. The aortic valve closes when the pressure in the left ventricle falls below that in the aorta, while the pulmonary valve closes when right ventricular pressure drops below pulmonary artery pressure. This closure is abrupt, creating vibrations in the valve leaflets and surrounding structures, which are audible as S2. Auscultation techniques, such as using the diaphragm of the stethoscope over the second intercostal space (for A2) and the third left sternal border (for P2), can help isolate these components. Practicing on patients with varying heart rates or during maneuvers like deep breathing enhances the ability to discern normal from abnormal S2 sounds.
From a comparative perspective, S2 contrasts with S1, which is generated by the closure of the atrioventricular valves (mitral and tricuspid). While S1 signifies the start of systole, S2 marks its end, creating a distinct "lub-dub" rhythm. Pathological variations of S2, such as a wide or paradoxically split S2, can indicate conditions like left bundle branch block or pulmonary hypertension, respectively. For example, in pulmonary hypertension, the P2 component becomes louder and may even overshadow A2, a finding that warrants further investigation. Recognizing these nuances is crucial for early diagnosis and intervention.
Instructively, teaching auscultation of S2 should emphasize both technique and interpretation. Begin by ensuring the patient is in a quiet environment, preferably in the supine position. Use a systematic approach, starting with the aortic area and moving to the pulmonary area, noting the intensity, timing, and splitting of S2. For learners, recording heart sounds or using simulation tools can reinforce understanding. Additionally, correlating auscultation findings with other diagnostic modalities, such as echocardiography, provides a comprehensive view of valve function. This multimodal approach ensures accuracy in assessing the health of the semilunar valves.
Finally, the practical takeaway is that S2 is more than just a sound—it is a window into the dynamic function of the semilunar valves. By mastering its auscultation, healthcare providers can detect early signs of valve dysfunction or systemic issues. For instance, a delayed or absent A2 may suggest aortic valve insufficiency, while a prominent P2 could indicate right-sided heart strain. Regular practice and familiarity with normal variations across age groups (e.g., children may have a more pronounced split S2) enhance diagnostic confidence. In essence, S2 is a vital tool in the clinician’s arsenal, bridging the gap between physiology and patient care.
Nashville Sounds: Uncovering Tennessee's Beloved Minor League Baseball Team
You may want to see also
Explore related products


![The Normal Heart [DVD] (English audio. English subtitles)](https://m.media-amazon.com/images/I/91e--qvJnjL._AC_UY218_.jpg)



![]()
Blood Flow Turbulence: Laminar flow through valves and vessels contributes to normal sounds
The heart's rhythmic symphony, often described as the iconic 'lub-dub' sound, is a result of the intricate dance of blood flow through its chambers and valves. This harmonious melody is not merely a sign of life but a testament to the precision of cardiovascular physics. At the core of this phenomenon lies the concept of blood flow turbulence, a critical factor in understanding normal heart sounds.
The Role of Laminar Flow: Imagine blood as a river flowing through the heart's vessels and valves. In an ideal scenario, this flow is laminar, meaning it moves in parallel layers, smooth and efficient. This type of flow is characterized by its predictability and minimal resistance, allowing blood to travel effortlessly through the cardiovascular system. When blood flows laminarly, it creates a gentle, consistent sound, contributing to the softer components of the heart's auditory signature.
Turbulence and Valve Function: As blood encounters the heart's valves, a fascinating transformation occurs. These valves, acting as gatekeepers, ensure unidirectional flow. During valve closure, the sudden change in flow direction and velocity introduces turbulence. This turbulence is not a sign of disorder but a necessary consequence of the heart's efficient design. The turbulent flow creates distinct sounds, particularly the sharper 'dub' sound, which is crucial for medical professionals to assess heart health. For instance, a heart murmur, often detected during auscultation, can indicate turbulent flow due to valve abnormalities, providing valuable diagnostic insights.
Vessel Geometry and Flow Dynamics: The architecture of blood vessels also plays a pivotal role in flow turbulence. As blood navigates through the aorta and other major vessels, the shape and diameter of these conduits influence flow patterns. In certain areas, such as vessel bifurcations or regions with atherosclerotic plaques, turbulence may increase. This localized turbulence contributes to the overall acoustic profile of the heart, adding subtle nuances to the soundscape. Understanding these flow dynamics is essential for differentiating between normal and pathological heart sounds.
Practical Implications: Recognizing the significance of blood flow turbulence has practical applications in healthcare. For instance, during a physical examination, a trained healthcare provider can use a stethoscope to listen for these sounds, assessing the heart's performance. The quality and intensity of turbulence-induced sounds can provide clues about valve competence, blood pressure, and even the presence of structural abnormalities. Moreover, advanced imaging techniques, such as Doppler ultrasound, can visually represent blood flow patterns, aiding in the diagnosis of cardiovascular conditions related to turbulent flow.
In essence, the normal sounds of the heart are a symphony orchestrated by the precise interplay of laminar and turbulent blood flow. This understanding not only deepens our appreciation for the heart's complexity but also equips medical professionals with valuable tools for diagnosis and patient care. By deciphering the language of blood flow turbulence, we unlock a critical aspect of cardiovascular health assessment.
Does Maxxaudio Enhance Stereo Sound Quality? A Comprehensive Analysis
You may want to see also
Explore related products






![]()
Chest Wall Transmission: Heart sounds travel through tissues to auscultation sites
Heart sounds, those rhythmic lub-dubs, originate from the mechanical movements of cardiac valves and blood flow. However, their transmission to auscultation sites like the chest wall is a complex journey through multiple tissue layers. Understanding this process is crucial for accurate interpretation during physical examination.
Chest wall transmission involves the propagation of sound waves generated by the heart through various tissues, including skin, subcutaneous fat, muscle, and bone. These tissues act as both conductors and filters, influencing the frequency and intensity of the sounds that reach the stethoscope. For instance, higher-frequency sounds, which are crucial for detecting murmurs, are more readily absorbed by tissues, making them harder to detect without proper technique.
To optimize auscultation, clinicians must consider the patient’s body habitus. Thicker layers of subcutaneous fat or muscle can dampen sound transmission, necessitating firmer stethoscope pressure or repositioning. Conversely, in lean individuals, sounds may transmit more clearly but with less attenuation, potentially amplifying both normal and abnormal sounds. Pediatric patients, with their thinner chest walls, often require lighter pressure to avoid distorting the sounds.
Practical tips for enhancing chest wall transmission include ensuring the patient is in a relaxed position, as tension in chest wall muscles can impede sound conduction. Warming the stethoscope diaphragm can also improve patient comfort and reduce the dampening effect of cold materials on sound transmission. Additionally, using a stethoscope with a bell for low-frequency sounds (S1, S2) and a diaphragm for high-frequency sounds (murmurs) maximizes the clarity of auscultated sounds.
In summary, chest wall transmission is a critical yet often overlooked aspect of heart sound auscultation. By understanding how tissues influence sound propagation and adapting techniques accordingly, clinicians can improve diagnostic accuracy and patient care. This knowledge bridges the gap between the heart’s mechanical activity and the sounds heard at the chest wall, making it an essential skill in cardiovascular assessment.
Unveiling the Unique and Playful Sound of a Laughing Fox
You may want to see also
Frequently asked questions
Normal heart sounds are primarily caused by the closing of the heart valves during the cardiac cycle. The first heart sound (S1) is produced by the closure of the mitral and tricuspid valves, while the second heart sound (S2) is caused by the closure of the aortic and pulmonary valves.
Blood flow through the heart creates pressure changes that force the valves to close, producing the characteristic "lub-dub" sounds. The "lub" (S1) occurs when the atrioventricular valves close, and the "dub" (S2) occurs when the semilunar valves close, ensuring one-way blood flow.
Yes, external factors can influence heart sounds. Physical activity or exercise can increase heart rate, making the sounds more rapid but still normal. Age can also affect heart sounds, as valve flexibility may decrease over time, altering the quality of the sounds slightly, though they remain within normal ranges.