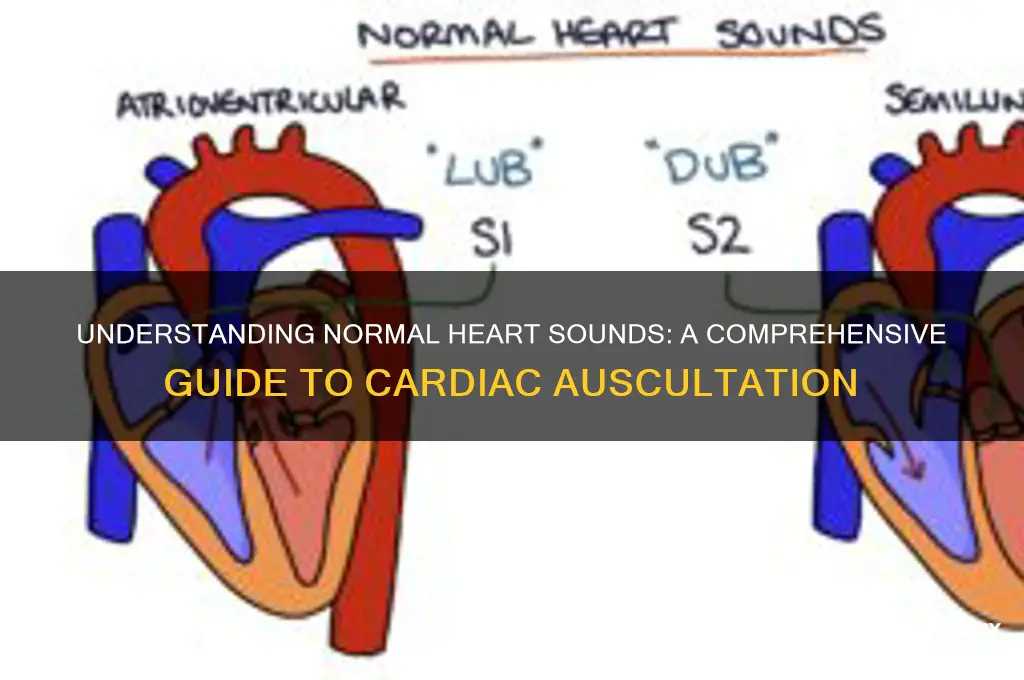
Normal heart sounds are the rhythmic noises produced by the closing of the heart valves as blood flows through the heart's chambers. Typically, two distinct sounds, often described as lub-dub, are heard through a stethoscope. The first sound (S1), or lub, occurs when the mitral and tricuspid valves close, marking the beginning of systole, when the heart contracts to pump blood. The second sound (S2), or dub, is produced by the closure of the aortic and pulmonary valves, signaling the end of systole and the start of diastole, when the heart relaxes and fills with blood. These sounds are crucial for assessing cardiac function, as any deviations in their timing, quality, or intensity can indicate underlying heart conditions. Understanding normal heart sounds is essential for healthcare professionals to diagnose and monitor cardiovascular health effectively.
Explore related products






What You'll Learn
- First and Second Heart Sounds: Understanding S1 (lub) and S2 (dub) as primary heart sounds
- Innocent Heart Murmurs: Benign extra sounds often heard in children and healthy adults
- Abnormal Heart Sounds: Identifying third or fourth heart sounds (S3, S4) and murmurs
- Heart Sound Timing: Analyzing when sounds occur during the cardiac cycle
- Heart Sound Intensity: Assessing loudness and quality of normal versus abnormal sounds
![]()
First and Second Heart Sounds: Understanding S1 (lub) and S2 (dub) as primary heart sounds
The human heart produces a symphony of sounds, but two stand out as the primary conductors of this cardiac orchestra: the first heart sound (S1) and the second heart sound (S2). These sounds, often described as "lub" (S1) and "dub" (S2), are the most prominent and clinically significant auscultatory findings in a normal heart. Understanding their origins and characteristics is essential for healthcare professionals and anyone interested in cardiac physiology.
The "Lub" (S1) Sound: A Closer Look
S1 occurs at the beginning of systole, the phase when the heart contracts to pump blood. It is primarily caused by the closure of the mitral and tricuspid valves, which prevent blood from flowing back into the atria as the ventricles contract. This sound is low-pitched and lasts approximately 0.1 to 0.14 seconds. Clinically, S1 is best heard at the apex of the heart, typically located in the fifth intercostal space at the midclavicular line. Its intensity and quality can provide insights into valve function and ventricular contraction strength. For example, a widened or split S1 may suggest issues with valve closure or electrical conduction abnormalities.
The "Dub" (S2) Sound: Decoding Its Significance
S2 marks the beginning of diastole, the relaxation phase of the heart. It results from the closure of the aortic and pulmonary valves, which prevent backflow into the ventricles as they fill with blood. Unlike S1, S2 is higher-pitched and slightly shorter, lasting around 0.08 to 0.1 seconds. It is best auscultated at the base of the heart, particularly the second right intercostal space for the aortic component and the third left intercostal space for the pulmonary component. A normally split S2 is physiological, but a widened or paradoxically split S2 can indicate conditions like left bundle branch block or pulmonary hypertension.
Comparing S1 and S2: Key Differences and Clinical Implications
While both sounds are critical, their timing, pitch, and location differ significantly. S1 is associated with systole and valve closure between atria and ventricles, while S2 is linked to diastole and valve closure between ventricles and arteries. Practically, auscultating these sounds requires a systematic approach: listen first at the apex for S1, then move to the base for S2. For children and young adults, S2 may be single due to simultaneous valve closure, but with age, it often splits physiologically. Recognizing these nuances is vital for distinguishing normal variants from pathological murmurs.
Practical Tips for Auscultation
To effectively hear S1 and S2, use the bell of the stethoscope for low-pitched S1 and the diaphragm for high-pitched S2. Ensure the patient is in a relaxed position, as anxiety can alter heart sounds. For pediatric patients, use a smaller stethoscope head and be mindful of faster heart rates, which may make S1 and S2 less distinct. Document the intensity, duration, and quality of each sound, as these details can guide further diagnostic steps. For instance, a soft S1 may warrant an echocardiogram to assess valve function.
Takeaway: The Foundation of Cardiac Auscultation
Mastering the identification of S1 and S2 is the cornerstone of cardiac auscultation. These sounds provide a window into the heart’s mechanical function, allowing early detection of abnormalities. By understanding their origins, characteristics, and clinical implications, healthcare providers can differentiate normal heart sounds from pathological ones, ensuring timely and accurate patient care. Whether in a routine checkup or a critical care setting, S1 and S2 remain indispensable tools in the medical toolkit.
Do Skunks Meow? Unraveling the Surprising Sounds of Skunks vs. Cats
You may want to see also
Explore related products


$12.99




![]()
Innocent Heart Murmurs: Benign extra sounds often heard in children and healthy adults
Heart sounds, typically described as the rhythmic "lub-dub," are the result of blood flowing through the heart's chambers and valves. However, not all heart sounds are cause for alarm. Innocent heart murmurs, often detected during routine check-ups, are benign extra sounds that can be heard in children and healthy adults. These murmurs are distinct from pathological murmurs, which may indicate underlying heart conditions. Understanding innocent murmurs is crucial for distinguishing them from more serious issues, ensuring appropriate care and reducing unnecessary anxiety.
Innocent murmurs are most commonly heard in children, particularly between the ages of 3 and 7, due to the rapid growth and increased blood flow demands of their developing bodies. These murmurs are often described as soft, high-pitched, and brief, typically occurring during specific phases of the cardiac cycle. For instance, a still murmur, a type of innocent murmur, is frequently heard in children and is characterized by its benign nature and lack of associated symptoms. In adults, innocent murmurs may arise from conditions like pregnancy, anemia, or hyperthyroidism, where the heart works harder to meet increased metabolic demands.
Diagnosing innocent murmurs involves a thorough physical examination, including auscultation with a stethoscope, and sometimes additional tests like electrocardiograms (ECGs) or echocardiograms to rule out structural abnormalities. Healthcare providers assess the murmur’s timing, intensity, and location to differentiate it from pathological murmurs. For example, innocent murmurs are often grade I or II on a six-point scale, whereas pathological murmurs may be louder and accompanied by symptoms like chest pain or shortness of breath. Parents and individuals should remain calm if a murmur is detected, as most innocent murmurs resolve on their own without intervention.
Practical tips for managing innocent murmurs include regular follow-ups with a healthcare provider to monitor any changes. Parents should avoid restricting their child’s physical activities unless advised otherwise, as innocent murmurs do not typically impair heart function. Adults with innocent murmurs should focus on addressing underlying conditions, such as treating anemia or managing thyroid disorders, to alleviate the extra strain on the heart. Education and awareness are key to reducing fear and ensuring that benign murmurs are not mistaken for more serious cardiac issues.
In conclusion, innocent heart murmurs are common, harmless extra sounds that require no treatment but warrant understanding and monitoring. By recognizing their characteristics and contexts, individuals and healthcare providers can differentiate them from pathological murmurs, promoting peace of mind and appropriate care. Whether in a growing child or a healthy adult, these murmurs are a reminder of the heart’s adaptability and resilience in meeting the body’s demands.
How a Tweeter's Position Affects Audio Quality
You may want to see also
Explore related products






![]()
Abnormal Heart Sounds: Identifying third or fourth heart sounds (S3, S4) and murmurs
Normal heart sounds, typically described as the familiar "lub-dub" (S1 and S2), are produced by the closing of heart valves and mark the beginning and end of systole and diastole. However, the presence of additional sounds, such as S3 or S4, or abnormal murmurs, can signal underlying cardiac issues. These sounds are not part of the standard cardiac cycle and often require careful auscultation to detect. For instance, a third heart sound (S3), also known as a "ventricular gallop," is a low-pitched sound occurring in early diastole, while a fourth heart sound (S4), or "atrial gallop," is heard in late diastole. Both are associated with increased ventricular filling pressures and can indicate conditions like heart failure or hypertensive heart disease.
Identifying S3 and S4 requires a systematic approach. Begin by using the bell of the stethoscope for low-pitched sounds and listen at the apex of the heart, with the patient in the left lateral decubitus position. S3 is best heard in children, pregnant individuals, or athletes as a benign finding, but in adults, it often signifies volume overload or reduced compliance. S4, on the other hand, is rarely normal and typically indicates stiffened ventricles, commonly seen in hypertension or aortic stenosis. A useful mnemonic is "S3 follows S2, S4 precedes S1," helping clinicians differentiate between the two.
Murmurs, another form of abnormal heart sound, are whooshing noises caused by turbulent blood flow. They are categorized by timing (systolic or diastolic), intensity (graded 1 to 6), and location. For example, a systolic ejection murmur in a child could indicate an innocent heart murmur, while the same in an adult might suggest aortic stenosis. Diastolic murmurs, such as those heard in mitral stenosis, are often lower-pitched and require careful differentiation from S3 or S4. Auscultation should be paired with patient history and risk factors to determine the murmur’s significance.
Practical tips for clinicians include using a quiet room, ensuring proper patient positioning, and comparing sounds across multiple heart areas. For S3 and S4, ask the patient to exhale while listening, as this can enhance detection. Murmurs may require additional maneuvers, such as handgrip or squatting, to provoke changes in intensity. Referral for echocardiography is often necessary to confirm the cause of abnormal sounds, especially in ambiguous cases. Early recognition of these sounds can lead to timely intervention, preventing progression to more severe cardiac conditions.
In summary, while normal heart sounds are straightforward, abnormal sounds like S3, S4, and murmurs demand attention to detail. Understanding their characteristics, associated conditions, and auscultation techniques empowers clinicians to diagnose and manage cardiac issues effectively. Mastery of these skills is essential for anyone evaluating cardiovascular health, ensuring that deviations from the norm are neither missed nor misinterpreted.
Understanding Sound Level Measurement: Techniques, Tools, and Decibel Scales
You may want to see also
Explore related products






![]()
Heart Sound Timing: Analyzing when sounds occur during the cardiac cycle
The cardiac cycle, a symphony of contractions and relaxations, produces a distinct rhythm of heart sounds. These sounds, often described as "lub-dub," are not random but occur at precise moments, each tied to specific events in the heart's workflow. Understanding this timing is crucial for healthcare professionals to diagnose cardiac abnormalities and ensure the heart functions optimally.
Let's dissect the timing of these sounds, exploring their significance and how they reflect the heart's intricate dance.
First, the "lub" sound, medically termed S1, marks the beginning of systole, the phase when the ventricles contract. This sound coincides with the closure of the atrioventalricular (AV) valves—the mitral and tricuspid valves—as blood is forcefully ejected into the aorta and pulmonary artery. S1 typically occurs around 0.12 to 0.16 seconds after the onset of the ECG R wave, a key reference point in cardiac timing. For clinicians, an abnormally split or delayed S1 can indicate issues like bundle branch block or valve dysfunction.
Next, the "dub" sound, or S2, signals the end of systole and the start of diastole, when the ventricles relax. This sound corresponds to the closure of the semilunar valves—the aortic and pulmonary valves—preventing backflow of blood into the ventricles. S2 usually occurs 0.28 to 0.32 seconds after the R wave. In children and young adults, S2 is often single, but in older adults, it may physiologically split due to differences in pressure between the aorta and pulmonary artery. An unusually wide or paradoxically split S2 can hint at conditions like pulmonary hypertension or left bundle branch block.
Beyond S1 and S2, additional heart sounds like S3 and S4 may occur in certain conditions. S3, a soft "ta" sound, is heard in early diastole and is normal in children and some athletes but pathological in adults, often indicating heart failure. S4, another soft sound, occurs in late diastole and is associated with a stiffened ventricle, commonly seen in hypertension or left ventricular hypertrophy. Both S3 and S4 are best heard with the patient in the left lateral position and during expiration.
Analyzing heart sound timing requires a systematic approach. Start by identifying the ECG R wave as the temporal anchor. Use a stethoscope with the bell for low-pitched sounds (S3, S4) and the diaphragm for high-pitched sounds (S1, S2). Note the duration and quality of each sound, comparing them to established norms. For instance, S1 is typically longer and lower in pitch than S2. In pediatrics, heart rates are faster (100–160 bpm in infants), so sounds are closer together, requiring quicker auscultation.
In conclusion, heart sound timing is a window into the cardiac cycle's efficiency. By mastering this timing, healthcare providers can detect subtle abnormalities early, guiding timely interventions. Whether in a routine checkup or a critical care setting, precise auscultation remains an indispensable tool in cardiovascular assessment.
Rock-Solid Sounds: B&W's Audio Revolution
You may want to see also
Explore related products






![]()
Heart Sound Intensity: Assessing loudness and quality of normal versus abnormal sounds
The intensity of heart sounds, measured by their loudness and quality, serves as a critical diagnostic tool in cardiology. Normal heart sounds, specifically S1 and S2, are typically soft yet distinct, with S1 slightly louder than S2 in most individuals. These sounds correspond to the closure of the atrioventricular (AV) valves (S1) and the semilunar valves (S2), respectively. Assessing their intensity requires a stethoscope and a trained ear, as subtle changes can indicate underlying conditions. For instance, a wide pulse pressure or fever may physiologically increase sound intensity, while pathological conditions like mitral stenosis can cause abnormally loud S1.
To evaluate heart sound intensity effectively, follow these steps: position the patient in a supine or left lateral decubitus position, use a high-quality stethoscope, and listen systematically at the aortic, pulmonic, tricuspid, and mitral areas. Normal S1 is best heard at the tricuspid and mitral areas, while S2 is clearest at the aortic and pulmonic regions. Note the relative loudness and any changes in quality, such as snapping or dullness. For children, adjust the stethoscope pressure gently, as their chest walls are more compliant. Adults over 50 may exhibit softer heart sounds due to age-related valve thickening, so baseline comparisons are essential.
Abnormal heart sound intensity often signals valve dysfunction or structural abnormalities. For example, a pansystolic murmur with a loud, high-pitched quality suggests mitral regurgitation, while a loud, palpable S2 (known as a "wide-fixed split") can indicate pulmonary hypertension. In contrast, diminished heart sounds may arise from conditions like pericardial effusion or obesity, where adipose tissue muffles transmission. Always correlate intensity findings with other clinical data, such as echocardiography, to avoid misdiagnosis.
Practical tips for accurate assessment include minimizing ambient noise, ensuring proper stethoscope placement, and using the diaphragm for low-pitched sounds (S3, S4) and the bell for high-pitched sounds (S1, S2). For pediatric patients, use age-appropriate stethoscope heads and explain the procedure to reduce anxiety. In adults, ask about symptoms like chest pain or shortness of breath, as these may guide your focus during auscultation. Remember, intensity is just one aspect of heart sound analysis; timing, pitch, and duration are equally important for a comprehensive evaluation.
In conclusion, mastering heart sound intensity assessment bridges the gap between normal and abnormal cardiac function. By understanding the nuances of loudness and quality, clinicians can detect early signs of pathology and tailor interventions accordingly. Regular practice, coupled with a systematic approach, ensures accuracy and confidence in this fundamental skill. Whether in a bustling ER or a quiet clinic, the ability to discern normal from abnormal heart sounds remains a cornerstone of cardiovascular care.
Exploring the Unique Sounds and Voices of Modern Robots
You may want to see also
Frequently asked questions
Normal heart sounds consist of two primary sounds, often described as "lub-dub." The first sound (S1) is caused by the closing of the mitral and tricuspid valves, while the second sound (S2) is caused by the closing of the aortic and pulmonary valves.
In a normal heart, there are two distinct sounds, referred to as S1 and S2. Additional sounds, such as S3 or S4, may be present in certain conditions but are not typically heard in a healthy heart.
The "lub" sound (S1) is produced by the closing of the atrioventricular valves (mitral and tricuspid), while the "dub" sound (S2) is produced by the closing of the semilunar valves (aortic and pulmonary).
Yes, normal heart sounds can vary slightly between individuals due to factors such as age, heart size, and body habitus. However, the basic "lub-dub" pattern remains consistent in a healthy heart.
Normal heart sounds serve as a baseline for comparison when diagnosing heart conditions. Abnormalities in heart sounds, such as murmurs, extra sounds, or changes in timing, can indicate underlying cardiac issues and prompt further evaluation.