Documenting lung sounds is a critical skill in clinical practice, as it provides valuable insights into a patient’s respiratory health. Proper documentation involves systematically auscultating specific lung regions, noting the characteristics of breath sounds, and identifying any abnormalities such as wheezes, crackles, or diminished airflow. Accurate recording of these findings in the patient’s medical chart ensures continuity of care, aids in diagnosing conditions like pneumonia, asthma, or COPD, and supports evidence-based decision-making. Effective documentation also includes noting the patient’s position, breathing pattern, and any factors that may influence the auscultation results, ensuring a comprehensive and reliable assessment.
| Characteristics | Values |
|---|---|
| Patient Position | Sitting upright or semi-recumbent; ensure comfort for optimal auscultation. |
| Equipment | Stethoscope (preferably dual-head with bell and diaphragm). |
| Anatomical Landmarks | Identify lung fields: anterior, posterior, lateral, and axillary regions. |
| Technique | Use both bell (low-pitched sounds) and diaphragm (high-pitched sounds) of the stethoscope. |
| Breathing Instructions | Ask patient to breathe normally, then take deep breaths for better assessment. |
| Sound Characteristics | Document pitch (high/low), intensity (loud/soft), quality (e.g., wheezes, crackles, rhonchi), and duration. |
| Normal Lung Sounds | Vesicular breathing (soft during inspiration, quieter during expiration). |
| Abnormal Sounds | Wheezes (high-pitched, whistling), crackles (popping or bubbling), rhonchi (low-pitched, rattling), stridor (harsh, high-pitched). |
| Location | Note the specific lung field(s) where abnormal sounds are heard (e.g., right lower lobe). |
| Symmetry | Compare sounds between left and right lungs for asymmetry. |
| Documentation Format | Use clear, concise descriptions (e.g., "Bilateral wheezes in upper lobes, crackles in left lower lobe"). |
| Additional Notes | Include patient’s position, breathing effort, and any observed distress during auscultation. |
| Frequency | Document lung sounds at initial assessment and with any changes in respiratory status. |
| Comparative Analysis | Compare current findings with previous assessments for trends or improvements. |
| Special Considerations | Note factors like obesity, chest wall thickness, or recent surgery that may affect sound transmission. |
Explore related products






What You'll Learn
- Equipment Preparation: Stethoscope positioning, patient placement, and environment setup for clear lung sound auscultation
- Anatomical Landmarks: Identifying key chest areas (e.g., lobes, segments) for accurate sound localization
- Normal vs. Abnormal Sounds: Differentiating between crackles, wheezes, stridor, and normal breath sounds
- Documentation Techniques: Recording findings using standardized terminology and structured formats for clarity
- Patient Positioning: Supine, sitting, or lateral positions to assess lung sounds effectively
![]()
Equipment Preparation: Stethoscope positioning, patient placement, and environment setup for clear lung sound auscultation
To ensure accurate documentation of lung sounds, proper equipment preparation is essential. Begin by inspecting the stethoscope for any damage or debris, ensuring the earpieces, tubing, and diaphragm are clean and functional. Position the stethoscope correctly by angling the earpieces to face forward in your ears, creating a tight seal to minimize external noise. Hold the stethoscope diaphragm gently but firmly against the patient’s skin, avoiding clothing or loose fabric that could muffle sounds. For low-pitched sounds, use the bell by lightly pressing it against the chest wall; for high-pitched sounds, use the diaphragm with firmer pressure. Ensure the tubing is not twisted or kinked, as this can interfere with sound transmission.
Patient placement is critical for optimal auscultation. Position the patient in a comfortable, upright sitting position, as this allows for maximum lung expansion and clear sound detection. If the patient is unable to sit, a semi-recumbent position (45-degree angle) is acceptable. Instruct the patient to relax and breathe normally through their mouth, as this reduces upper airway noise. For posterior lung fields, have the patient lean slightly forward or turn their head to the side to expose the back fully. Ensure the patient’s clothing is loosened or removed around the chest area to allow direct skin contact with the stethoscope.
The environment setup plays a significant role in obtaining clear lung sounds. Choose a quiet room with minimal background noise, such as the hum of machinery or conversations, which can obscure subtle lung sounds. Close windows to reduce external noise and maintain a comfortable room temperature to prevent patient discomfort. Ensure adequate lighting to clearly see anatomical landmarks for proper stethoscope placement. If using a digital stethoscope or recording device, test the equipment beforehand to ensure it is functioning correctly and positioned to capture sounds accurately.
Proper stethoscope positioning involves systematic auscultation of lung fields. Begin at the apex (upper part of the lung) and move downward in a logical pattern, covering all areas: anterior, posterior, and lateral chest walls. Place the stethoscope over each lung field for at least 5-10 seconds to listen for normal breath sounds, adventitious sounds, or abnormalities. Avoid rushing, as this can lead to missed findings. Use anatomical landmarks, such as the clavicle, scapula, and spine, to guide placement and ensure comprehensive coverage.
Finally, prepare any additional tools needed for documentation, such as a notepad, digital device, or auscultation map. Note the patient’s position, stethoscope placement, and the specific lung fields being assessed. Record the quality, intensity, and timing of breath sounds (e.g., vesicular, wheezes, crackles) in a clear, concise manner. If using a recording device, label the audio file with the patient’s details and the corresponding lung field for future reference. Consistent and organized preparation ensures accurate and reliable documentation of lung sounds.
Subwoofer Ports: Sound Emittance Explained
You may want to see also
Explore related products






![]()
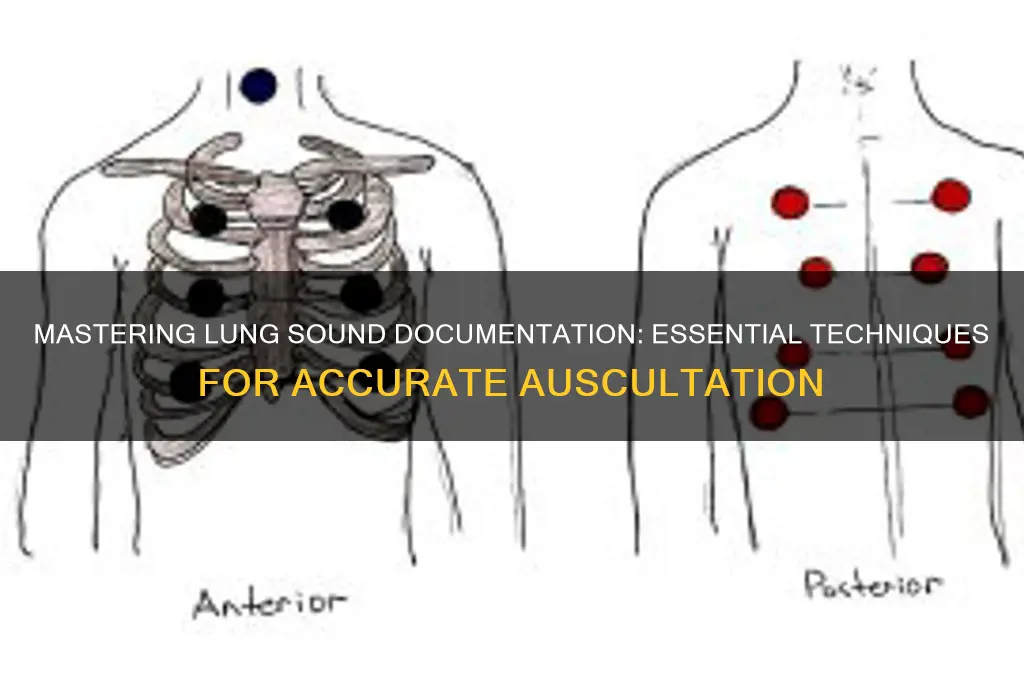
Anatomical Landmarks: Identifying key chest areas (e.g., lobes, segments) for accurate sound localization
Accurate localization of lung sounds is crucial for effective auscultation and documentation. To achieve this, understanding the anatomical landmarks of the chest is essential. The human lungs are divided into lobes—three in the right lung (upper, middle, and lower) and two in the left lung (upper and lower). Each lobe is further divided into segments, which are smaller, distinct areas. Identifying these areas allows healthcare providers to pinpoint the origin of abnormal sounds, such as crackles, wheezes, or diminished breath sounds. The first key landmark is the sternal border, which runs vertically along the sternum. This helps in distinguishing between the right and left lung fields. The clavicles and scapulae also serve as important reference points, as they mark the upper limits of the lung fields and help avoid confusion with other anatomical structures.
The inter-scapular region is another critical area, as it overlies the posterior segments of the lower lobes. Sounds heard here often indicate issues in the basal segments of the lungs. The axillary regions are also significant, as they correspond to the lateral segments of the upper and lower lobes. Palpating the spine and vertebral columns aids in identifying the posterior lung fields, which are divided into the upper, middle, and lower zones. The nipple line (fifth intercostal space) and the mid-clavicular line are commonly used to divide the chest into specific quadrants, facilitating precise localization of sounds.
The anterior chest wall is divided into the upper, middle, and lower zones, each corresponding to specific lung segments. For instance, the upper zone corresponds to the apices of the lungs, where abnormalities like apical wheezing may be detected. The posterior chest wall is similarly divided, with the upper zone corresponding to the superior segments of the lower lobes. The lateral chest wall is particularly useful for assessing the lateral segments of the lungs, where conditions like pleural effusions may manifest as diminished sounds.
To accurately localize sounds, it is important to correlate anatomical landmarks with lung segments. For example, the second intercostal space at the mid-clavicular line corresponds to the apex of the lung, while the sixth intercostal space at the mid-clavicular line overlies the upper lobe. The eighth intercostal space at the scapular line corresponds to the inferior segment of the lower lobe. By systematically auscultating these areas and noting the quality and intensity of sounds, healthcare providers can create a detailed map of lung function.
Finally, understanding the relationship between anatomical landmarks and lung segments ensures consistency in documentation. For instance, crackles heard in the fifth intercostal space at the mid-axillary line likely originate from the anterior segment of the upper lobe or the superior segment of the lower lobe. Wheezes heard in the second intercostal space at the sternum may indicate issues in the trachea or main bronchi. By integrating this knowledge into auscultation practice, healthcare providers can enhance diagnostic accuracy and provide targeted interventions for respiratory conditions.
Exploring the Bakersfield Sound: Roots, Artists, and Legacy
You may want to see also
Explore related products






![]()
Normal vs. Abnormal Sounds: Differentiating between crackles, wheezes, stridor, and normal breath sounds
When documenting lung sounds, it is crucial to differentiate between normal and abnormal sounds to accurately assess a patient’s respiratory status. Normal breath sounds are typically soft, smooth, and continuous, heard consistently throughout the respiratory cycle. They are categorized into vesicular (soft during inspiration, quieter during expiration) and tracheal (louder, higher-pitched sounds over the trachea). Normal breath sounds indicate clear airways and healthy lung tissue. In contrast, abnormal sounds such as crackles, wheezes, and stridor signal underlying respiratory issues and require careful documentation.
Crackles are abnormal lung sounds characterized by brief, popping noises that occur during inspiration. They are often described as crackling, bubbling, or rattling and are typically heard in patients with fluid accumulation in the alveoli or small airways, such as in pneumonia, heart failure, or pulmonary fibrosis. Crackles can be fine or coarse, with fine crackles being softer and higher-pitched, while coarse crackles are louder and lower-pitched. Documenting the location, intensity, and timing of crackles (e.g., "fine crackles heard bilaterally in lower lung fields during late inspiration") is essential for clinical evaluation.
Wheezes are high-pitched, whistling sounds produced by narrowed or obstructed airways, typically during expiration but can also occur during inspiration. They are commonly associated with asthma, chronic obstructive pulmonary disease (COPD), or bronchitis. Wheezes can be localized or diffuse and may vary in pitch and intensity. When documenting wheezes, note their presence, location, and phase of respiration (e.g., "expiratory wheezes heard diffusely throughout both lung fields"). Persistent or widespread wheezing may indicate severe airway obstruction requiring immediate intervention.
Stridor is a harsh, high-pitched, musical sound that occurs during inspiration and is caused by turbulent airflow through a narrowed upper airway. It is often a sign of acute obstruction, such as croup, epiglottitis, or a foreign body. Stridor is a medical emergency and requires urgent documentation and intervention. When noting stridor, specify its presence, intensity, and any associated symptoms (e.g., "inspiratory stridor heard in a child with acute respiratory distress").
In summary, differentiating between normal breath sounds and abnormal sounds like crackles, wheezes, and stridor is vital for accurate lung sound documentation. Normal sounds are soft, continuous, and consistent, while abnormal sounds indicate specific pathologies. Crackles suggest fluid or inflammation, wheezes indicate airway obstruction, and stridor signals upper airway narrowing. Detailed documentation, including the type, location, intensity, and timing of these sounds, provides critical information for diagnosis and treatment planning. Always use precise language and follow standardized terminology to ensure clarity and consistency in medical records.
Mastering Laptop Audio: Simple Steps to Adjust Sound Settings
You may want to see also
Explore related products






![]()
Documentation Techniques: Recording findings using standardized terminology and structured formats for clarity
When documenting lung sounds, it is essential to use standardized terminology and structured formats to ensure clarity, consistency, and accuracy in your findings. This approach facilitates effective communication among healthcare professionals and supports accurate diagnosis and treatment planning. Begin by familiarizing yourself with widely accepted terminology, such as the International Classification of Diseases (ICD) or the American Thoracic Society (ATS) guidelines, which provide a common language for describing lung sounds. Terms like "vesicular," "bronchial," "crackles," "wheezes," "stridor," and "rhonchi" should be used precisely to describe the characteristics of the sounds auscultated. Avoid vague or subjective descriptions that may lead to misinterpretation.
A structured format is crucial for organizing your documentation in a logical and easy-to-follow manner. Start by recording the patient’s demographic information, such as name, age, and medical record number, followed by the date and time of the assessment. Next, document the purpose of the auscultation, whether it is a routine check, follow-up, or in response to specific symptoms like cough or shortness of breath. Use a systematic approach to describe lung sounds, typically examining the lungs in a specific order (e.g., anterior to posterior, or by lung fields: right upper, right middle, right lower, left upper, and left lower). For each area, note the presence or absence of normal and abnormal sounds, their intensity (soft, moderate, loud), pitch (high, low), and any changes with respiration (inspiration, expiration, or both).
Incorporate a standardized template or checklist to ensure all relevant information is captured. For example, use a table or bullet points to list each lung field and the corresponding findings. Include additional observations such as symmetry between lung fields, the effect of positioning (e.g., sitting vs. lying down), and any patient responses during auscultation (e.g., discomfort or coughing). If using a stethoscope with recording capabilities, note the availability of audio or visual recordings for future reference or consultation with colleagues. Ensure your documentation is concise yet comprehensive, avoiding unnecessary details that do not contribute to the clinical picture.
Clarity in documentation also involves distinguishing between subjective and objective findings. Subjective data, such as the patient’s description of their symptoms (e.g., "I feel like there’s a tightness in my chest"), should be recorded verbatim in quotation marks. Objective findings, such as the auscultated lung sounds, must be described using precise, observable terms. For instance, instead of writing "lungs sound bad," document "bilateral fine crackles heard in the lower lung fields, more prominent on inspiration." This distinction ensures that your documentation is evidence-based and clinically useful.
Finally, conclude your documentation with a summary of key findings and any immediate actions taken or recommended. For example, note if the findings are consistent with a specific condition (e.g., pneumonia, asthma) or if further diagnostic tests (e.g., chest X-ray, spirometry) are warranted. Sign and timestamp your documentation to confirm its authenticity and completeness. Regularly review and update your documentation practices to align with current standards and guidelines, ensuring that your records remain a reliable tool for patient care and communication. By adhering to these techniques, you enhance the quality and utility of your lung sound documentation, ultimately contributing to better patient outcomes.
Mastering iMac Audio: Simple Steps to Adjust Sound Settings
You may want to see also
Explore related products






![]()
Patient Positioning: Supine, sitting, or lateral positions to assess lung sounds effectively
Proper patient positioning is crucial for effectively assessing and documenting lung sounds. The choice of position—supine, sitting, or lateral—can significantly influence the clarity and accuracy of auscultation. Each position allows access to different lung regions, ensuring a comprehensive evaluation. Here’s how to position the patient for optimal lung sound assessment:
Supine Position: In the supine position, the patient lies flat on their back with their head, neck, and spine in a neutral alignment. This position is ideal for assessing the posterior lung fields, particularly the lower lobes. To enhance sound transmission, place a small pillow under the patient’s knees to slightly elevate the chest. Instruct the patient to breathe normally through their mouth, as this reduces upper airway noise. Begin auscultation at the apex (upper region) of the lungs and move systematically downward, ensuring coverage of all lung segments. Document any abnormalities, such as crackles, wheezes, or diminished breath sounds, noting their location and intensity.
Sitting Position: The sitting position is advantageous for patients with respiratory distress or those who cannot lie flat. Have the patient sit upright with their feet flat on the floor and their hands resting on their lap or thighs. This position promotes maximal chest expansion and is particularly useful for assessing the anterior and lateral lung fields. Encourage the patient to take slow, deep breaths to facilitate better auscultation. Start at the apex and move downward, paying attention to symmetry between the left and right lungs. Note any asymmetry or abnormal sounds, as these may indicate localized pathology.
Lateral Positions (Left and Right): Lateral positioning is essential for assessing the lateral and posterior lung fields, which may not be fully accessible in supine or sitting positions. To position the patient laterally, have them lie on their side with their arms comfortably placed in front of them or resting on the opposite side. For the right lateral position, the patient lies on their right side, allowing access to the left posterior lung field. Conversely, the left lateral position provides access to the right posterior lung field. Ensure the patient’s back is straight and their chest is unobstructed. Instruct them to breathe normally while you auscultate systematically from the apex to the base. Document any findings, such as rales, rhonchi, or decreased breath sounds, specifying the position and lung region.
In all positions, maintain consistent technique and pressure while using the stethoscope to avoid artifactual sounds. Combine findings from each position to create a comprehensive assessment of lung sounds. Clear and detailed documentation of the patient’s position during auscultation is essential, as it provides context for the findings and aids in monitoring changes over time. By mastering these positioning techniques, healthcare providers can ensure accurate and thorough lung sound assessments.
Mastering CS:GO Sound Binding: A Step-by-Step Guide for Gamers
You may want to see also
Frequently asked questions
To document lung sounds, you will need a stethoscope, a recording device (such as a smartphone or digital recorder), and, optionally, auscultation software or apps for enhanced analysis.
The patient should be seated or in a semi-upright position, relaxed, and breathing normally. Ensure they are properly exposed for access to the chest and back areas.
Auscultate all lung fields, including the anterior, posterior, and lateral chest walls, focusing on key areas like the trachea, lung bases, and axillae.
Place the stethoscope firmly on the chest, minimize ambient noise, and record for at least 10–15 seconds per area. Label recordings with the location and patient details for clarity.
Document the type of sounds (e.g., normal, crackles, wheezes), their intensity, location, and any abnormalities. Include patient position, breathing pattern, and relevant clinical context.