Performing a carpal tunnel ultrasound exam is a non-invasive diagnostic procedure used to assess the median nerve and surrounding structures within the carpal tunnel. This exam involves using a high-frequency ultrasound probe to visualize the median nerve, flexor tendons, and transverse carpal ligament, allowing for the detection of abnormalities such as nerve swelling, tendon inflammation, or space-occupying lesions. The process begins with proper patient positioning, typically with the hand in a neutral or slightly extended position, followed by the application of ultrasound gel to the palmar aspect of the wrist. The sonographer then systematically scans the area, measuring the cross-sectional area of the median nerve at specific landmarks, such as the proximal and distal carpal tunnel, to identify signs of compression or pathology. This technique is valuable for diagnosing carpal tunnel syndrome and guiding treatment decisions, offering real-time imaging without the need for radiation exposure.
| Characteristics | Values |
|---|---|
| Patient Position | Sitting with forearm in neutral position, wrist slightly extended. |
| Transducer Position | Transverse or longitudinal orientation over the carpal tunnel area. |
| Frequency | 7.5–12 MHz linear array transducer for high-resolution imaging. |
| Anatomical Landmarks | Flexor retinaculum, median nerve, flexor tendons, and surrounding structures. |
| Median Nerve Assessment | Measure cross-sectional area (CSA) at the level of the pisiform bone. |
| Normal CSA Values | <10 mm² (may vary slightly based on reference). |
| Pathological CSA Values | >10 mm² (suggestive of carpal tunnel syndrome). |
| Dynamic Testing | Assess median nerve mobility during finger flexion/extension. |
| Additional Findings | Evaluate for tendonitis, ganglion cysts, or space-occupying lesions. |
| Artifacts to Avoid | Ensure proper coupling, avoid pressure-induced deformation of structures. |
| Reporting | Document CSA, nerve morphology, and any abnormalities in the report. |
| Contraindications | None specific, but avoid excessive pressure on the carpal tunnel area. |
| Advantages | Non-invasive, real-time imaging, no radiation exposure. |
| Limitations | Operator-dependent, may miss early-stage changes. |
Explore related products






What You'll Learn
- Patient Positioning: Supine, arm extended, wrist neutral, hand relaxed, ulnar side accessible for probe
- Probe Selection: Use high-frequency linear array transducer (7-12 MHz) for detailed imaging
- Transducer Placement: Longitudinal and transverse scans over the carpal tunnel area
- Anatomical Landmarks: Identify median nerve, flexor tendons, and surrounding structures
- Pathology Detection: Look for nerve swelling, synovial thickening, or space encroachment
![]()
Patient Positioning: Supine, arm extended, wrist neutral, hand relaxed, ulnar side accessible for probe
Proper patient positioning is the cornerstone of an accurate carpal tunnel ultrasound exam. The supine position, with the arm extended, wrist neutral, hand relaxed, and ulnar side accessible for the probe, creates an optimal acoustic window for visualizing the median nerve and surrounding structures. This positioning minimizes soft tissue interference and allows for consistent, reproducible imaging, which is crucial for both diagnostic accuracy and longitudinal comparisons.
From an anatomical perspective, this positioning aligns the carpal tunnel structures in a way that facilitates clear visualization. The extended arm and neutral wrist reduce flexion or extension artifacts, ensuring the median nerve remains in its natural course. A relaxed hand prevents muscle tension, which could distort the tunnel’s dimensions. Exposing the ulnar side of the wrist provides unobstructed access for the probe, enabling smooth scanning from the proximal to distal tunnel without repositioning.
Instructing the patient to lie supine with the arm extended along the table is straightforward, but attention to detail is key. Ensure the shoulder is not abducted or externally rotated, as this can strain the arm and alter wrist alignment. The wrist should be in a true neutral position—not hyperextended or flexed—which can be verified by aligning the third metacarpal with the forearm. For pediatric patients or those with limited mobility, gentle support with a pillow under the arm may be necessary to maintain comfort without compromising positioning.
A practical tip for sonographers is to use a small towel or gel pad under the patient’s hand to slightly elevate the wrist, enhancing probe contact and reducing pressure on the ulnar side. This simple adjustment can improve image quality, particularly in patients with obesity or edema. Additionally, warming the gel can increase patient comfort, reducing involuntary movements that might degrade the image.
While this positioning is standard, variations may be required for specific clinical scenarios. For instance, in patients with severe pain or limited range of motion, a semi-supine position with the arm slightly abducted may be more tolerable. However, such modifications should be minimal to avoid compromising diagnostic accuracy. Mastery of this positioning technique not only ensures high-quality imaging but also streamlines the exam, enhancing both patient experience and diagnostic confidence.
Effective Techniques to Remove Camera Autofocus Noise from Audio Recordings
You may want to see also
Explore related products






![]()
Probe Selection: Use high-frequency linear array transducer (7-12 MHz) for detailed imaging
Selecting the right probe is the cornerstone of a successful carpal tunnel ultrasound exam. The high-frequency linear array transducer, operating in the 7-12 MHz range, is the tool of choice for this application. Its design and frequency characteristics make it uniquely suited to capture the intricate anatomy of the wrist, where structures like the median nerve, flexor tendons, and surrounding soft tissues are tightly packed. Lower frequency probes, while useful for deeper structures, lack the resolution needed to discern the fine details critical for diagnosing carpal tunnel syndrome.
Consider the anatomy of the carpal tunnel: a narrow passageway approximately 2.5 cm in length, bounded by carpal bones and the flexor retinaculum. Within this confined space, the median nerve and nine flexor tendons must be visualized clearly. A high-frequency linear probe excels here because its small footprint allows for precise placement over the volar aspect of the wrist, and its high resolution enables differentiation between the hyperechoic fibrillary structure of tendons and the more homogeneous appearance of the median nerve. This level of detail is essential for assessing nerve swelling, tendon abnormalities, or synovial thickening—key indicators of carpal tunnel syndrome.
From a practical standpoint, using a 7-12 MHz transducer requires attention to technique. The probe should be oriented longitudinally and transversely to the forearm axis to obtain both axial and cross-sectional views. Applying minimal pressure is crucial to avoid compressing the median nerve, which could artificially alter its appearance. Coupling gel should be used liberally to ensure optimal acoustic transmission, and the wrist should be positioned in a neutral posture to mimic the tunnel’s natural dimensions. For patients with severe symptoms, slight flexion or extension may be necessary to provoke discomfort, aiding in dynamic assessment.
While high-frequency probes are ideal, they are not without limitations. Their shallow penetration depth (typically 3-4 cm) restricts their use to superficial structures, making them unsuitable for deeper examinations. Additionally, their high resolution comes at the cost of reduced tissue penetration, so proper patient positioning and probe angulation are critical. For obese patients or those with significant subcutaneous tissue, a lower frequency probe (e.g., 5-10 MHz) might be considered, though at the expense of some detail. However, for the majority of carpal tunnel exams, the 7-12 MHz linear array remains the gold standard.
In conclusion, the high-frequency linear array transducer is indispensable for carpal tunnel ultrasound due to its ability to provide detailed, high-resolution images of the wrist’s complex anatomy. Its selection is not arbitrary but rooted in the specific demands of the exam, where clarity and precision are paramount. By mastering its use, sonographers can confidently identify pathologies, guide treatments, and improve patient outcomes. This probe is not just a tool—it’s the key to unlocking diagnostic accuracy in carpal tunnel syndrome.
Mastering Auscultation: A Step-by-Step Guide to Identifying Lung Sounds
You may want to see also
Explore related products






![]()
Transducer Placement: Longitudinal and transverse scans over the carpal tunnel area
Proper transducer placement is critical for accurate carpal tunnel ultrasound evaluation, as it directly impacts visualization of key structures and diagnostic confidence. The two primary scanning planes—longitudinal and transverse—offer complementary perspectives of the carpal tunnel’s anatomy. In the longitudinal scan, position the transducer along the axis of the forearm, aligning it with the course of the median nerve. This orientation provides a continuous view of the nerve as it traverses the carpal tunnel, allowing assessment of its echogenicity, caliber, and relationship to surrounding structures like the flexor tendons. A slight medial or lateral tilt may be necessary to optimize visualization, particularly in patients with anatomical variations or prior surgery.
Contrastingly, the transverse scan involves placing the transducer perpendicular to the long axis of the forearm, capturing cross-sectional images of the carpal tunnel at specific levels. This plane is ideal for measuring the median nerve’s cross-sectional area (CSA) at the proximal tunnel inlet (scaphoid-pisiform level), where CSA >10 mm² is a reliable indicator of carpal tunnel syndrome. Ensure the transducer is angled to maintain the hyperechoic "tram track" appearance of the median nerve’s epineurium, which confirms proper alignment. Transverse scans also facilitate dynamic assessment during finger flexion, helping identify nerve mobility restrictions or bowstringing.
A systematic approach to transducer placement enhances diagnostic yield. Begin with a longitudinal scan at the distal forearm, 5–7 cm proximal to the pisiform, to identify the median nerve’s entry into the carpal tunnel. Gradually slide distally, observing for flattening or deformity of the nerve. Transition to transverse scans at the proximal tunnel (scaphoid-pisiform level), mid-tunnel (hook of hamate), and distal tunnel (distal to the transverse carpal ligament) to measure CSA and evaluate surrounding pathology, such as tenosynovitis or ganglia. Maintain gentle pressure to avoid compressing the tunnel artificially, which could mimic pathology.
Practical tips include using a high-frequency linear transducer (12–18 MHz) for optimal resolution and applying copious gel to minimize anisotropy. For obese patients or those with edema, adjust depth and gain settings to penetrate deeper tissues without losing clarity. In cases of nerve hypertrophy, compare CSA measurements bilaterally, as asymmetry >2 mm² is clinically significant. Combining longitudinal and transverse scans ensures comprehensive evaluation, enabling accurate diagnosis and guiding treatment decisions, such as steroid injection or surgical release. Mastery of these techniques transforms ultrasound into a powerful tool for carpal tunnel assessment.
Understanding the Science Behind Bone Cracking Sounds and Joint Health
You may want to see also
Explore related products






![]()
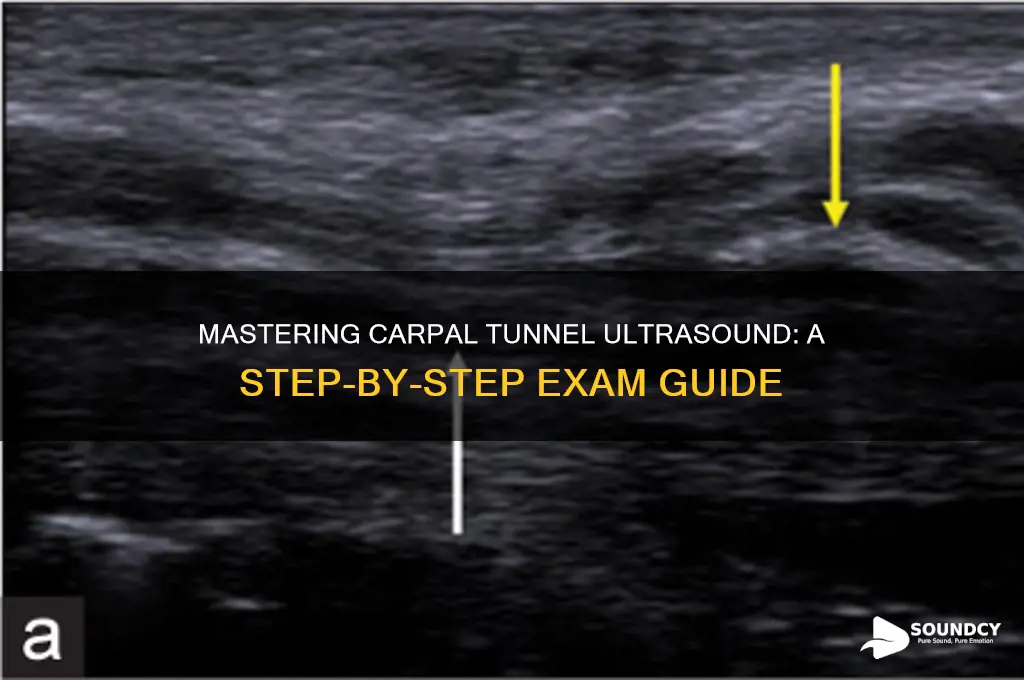
Anatomical Landmarks: Identify median nerve, flexor tendons, and surrounding structures
The median nerve, a critical structure in carpal tunnel ultrasound exams, is best identified by its location between the flexor tendons within the carpal tunnel. This nerve, approximately 2-3 mm in diameter, appears hyperechoic (bright) relative to surrounding tissues due to its epineural fat. Begin by placing the transducer transversely at the distal wrist crease, aligning it with the palmaris longus tendon as a midline reference. The median nerve lies deep to the flexor retinaculum, flanked by the flexor digitorum superficialis and profundus tendons, which appear as hypoechoic (darker) oval structures.
To ensure accurate identification, compare the median nerve’s position across multiple planes. In the longitudinal view, slide the transducer proximally along the course of the nerve, observing its continuity and relationship to the flexor tendons. The nerve should maintain its oval shape and echogenicity, distinguishing it from the more rounded, darker tendons. A helpful tip: apply gentle pressure with the transducer to displace surrounding tissues, enhancing the nerve’s visibility.
Misidentification of the median nerve is a common pitfall, often confused with the nearby flexor tendons or ulnar nerve. To avoid this, focus on the nerve’s characteristic branching pattern distal to the carpal tunnel, where it divides into digital branches. Additionally, the median nerve’s proximity to the palmar artery, visible as a pulsating structure, can serve as a secondary landmark. Always correlate ultrasound findings with clinical symptoms, such as tingling or numbness in the median nerve distribution, to confirm diagnostic accuracy.
Surrounding structures, including the flexor retinaculum and proximal carpal bones, provide essential context for assessing carpal tunnel pathology. The retinaculum appears as a thin, hyperechoic band superficial to the median nerve, while the scaphoid and pisiform bones serve as bony landmarks in deeper scans. When evaluating for compression, measure the cross-sectional area of the median nerve at the level of the distal wrist crease; values exceeding 10 mm² in adults may indicate carpal tunnel syndrome. This systematic approach ensures precise identification of anatomical landmarks, critical for both diagnostic and interventional ultrasound procedures.
Exploring the Ocean's Noisy Neighbors: Which Marine Creatures Make Sounds?
You may want to see also
Explore related products






![]()
Pathology Detection: Look for nerve swelling, synovial thickening, or space encroachment
Nerve swelling, synovial thickening, and space encroachment are hallmark signs of carpal tunnel syndrome (CTS) detectable via ultrasound. The median nerve, normally oval in cross-section, becomes flattened or deformed under pressure. Synovial tissue surrounding flexor tendons may appear hypoechoic and thickened, reducing the available space within the carpal tunnel. These abnormalities correlate with symptom severity and can guide treatment decisions, making ultrasound a valuable diagnostic tool.
To identify these pathologies, begin by locating the median nerve at the distal wrist crease, where the carpal tunnel inlet is narrowest. Use a high-frequency linear probe (12–18 MHz) for optimal resolution. Scan in both longitudinal and transverse planes, comparing the affected side to the contralateral wrist for asymmetry. Measure the cross-sectional area (CSA) of the median nerve at the proximal tunnel inlet; a CSA ≥10 mm² is highly suggestive of CTS in adults. Synovial thickening appears as a hypoechoic rim around flexor tendons, often with increased vascularity on Doppler.
While ultrasound is operator-dependent, its real-time imaging allows dynamic assessment during maneuvers like finger flexion or wrist extension. Encroachment of the carpal tunnel space may be evident when comparing tunnel dimensions to normative values or the unaffected side. For instance, a tunnel outlet-to-inlet ratio <0.6 indicates significant narrowing. However, avoid over-reliance on single measurements; combine findings for a comprehensive diagnosis.
Practical tips include using gel generously to avoid anisotropy artifacts, which can mimic pathology. Ensure patient comfort by maintaining a neutral wrist position during scanning. For pediatric cases, adjust CSA thresholds downward, as normal values vary by age. Document findings with annotated images for clarity in reporting. Ultrasound’s non-invasiveness and cost-effectiveness make it superior to MRI for initial CTS evaluation, though correlation with clinical symptoms remains essential.
Understanding Tinnitus: How Loud Noises Can Worsen Ringing Ears
You may want to see also
Frequently asked questions
The purpose of a carpal tunnel ultrasound exam is to evaluate the median nerve and surrounding structures in the wrist. It helps diagnose carpal tunnel syndrome by assessing nerve swelling, compression, or abnormalities in the carpal tunnel area.
The patient should be seated comfortably with the forearm resting on a table, palm facing upward (supinated position). The wrist should be in a neutral or slightly extended position to optimize visualization of the carpal tunnel and median nerve.
Key landmarks include the flexor retinaculum (transverse carpal ligament), pisiform bone, and hook of the hamate. The median nerve should be visualized as it passes through the carpal tunnel, and its cross-sectional area, echogenicity, and relationship to surrounding structures should be assessed.