Describing breath sounds is a critical skill in medical diagnostics, particularly in pulmonology, as it provides valuable insights into respiratory health. These sounds, produced by the movement of air through the respiratory tract, can be categorized into normal and abnormal types, each with distinct characteristics. Normal breath sounds, such as vesicular and bronchovesicular sounds, are typically soft and consistent, while abnormal sounds like wheezes, rhonchi, and crackles indicate underlying conditions such as asthma, chronic obstructive pulmonary disease (COPD), or pneumonia. Accurate description involves noting the pitch, intensity, timing, and location of the sounds, often aided by auscultation with a stethoscope. Mastering this skill enables healthcare professionals to differentiate between healthy lung function and pathological changes, guiding appropriate treatment and management.
| Characteristics | Values |
|---|---|
| Pitch | High, medium, or low frequency of breath sounds. |
| Intensity | Soft, loud, or whispered breath sounds. |
| Quality | Harsh, smooth, wheezy, gurgling, or stridorous. |
| Rhythm | Regular, irregular, or labored breathing patterns. |
| Duration | Short, prolonged, or intermittent breath phases. |
| Location | Unilateral (one side), bilateral (both sides), or localized to a region. |
| Timing | Inspiratory, expiratory, or biphasic (both phases). |
| Associated Sounds | Crackles, rhonchi, wheezing, stridor, or absence of sounds. |
| Effort | Effortless, labored, or use of accessory muscles. |
| Consistency | Constant, intermittent, or variable throughout respiration. |
| Response to Position | Changes in sound quality or intensity with positional changes. |
| Accompanying Symptoms | Cough, chest pain, fever, or cyanosis (blue discoloration). |
Explore related products

$71.99 $84.99





What You'll Learn
- Normal Breath Sounds: Characteristics of vesicular, bronchial, and broncho-vesicular sounds in healthy individuals
- Adventitious Sounds: Types, causes, and descriptions of wheezes, crackles, rhonchi, and stridor
- Assessment Techniques: Proper use of stethoscope, positioning, and auscultation methods for accurate evaluation
- Abnormal Patterns: Identifying diminished, absent, or asymmetrical breath sounds and their clinical significance
- Documentation Tips: Clear, concise ways to record breath sound findings in medical notes
![]()
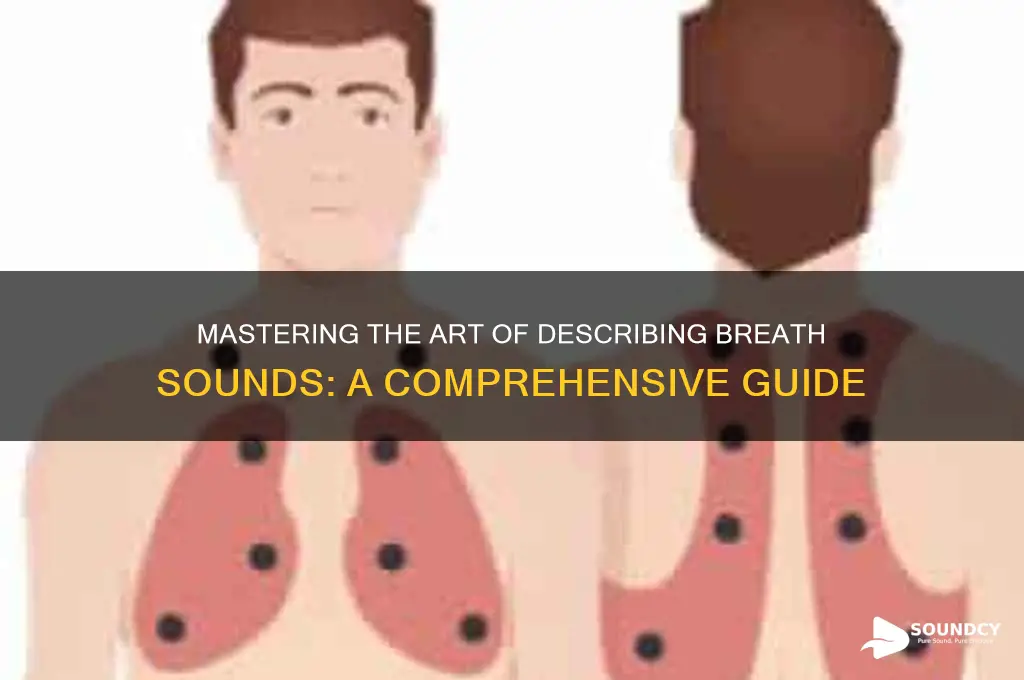
Normal Breath Sounds: Characteristics of vesicular, bronchial, and broncho-vesicular sounds in healthy individuals
Vesicular Breath Sounds are the most common and characteristic of normal breathing in healthy individuals. These sounds are typically heard over the majority of the lung fields, particularly in the peripheral regions. Vesicular breath sounds are soft, low-pitched, and rustling in quality, resembling the sound of air gently moving through a forest of small tubes. They are longer in duration during inspiration, typically lasting 2-3 times longer than expiration. This is because air moves more slowly through the smaller alveoli and distal airways during inhalation. Vesicular sounds are best heard in areas where the lung tissue is rich in alveoli, such as the bases and periphery of the lungs. In healthy individuals, these sounds are clear, without any added noises like wheezes, crackles, or rhonchi, indicating unobstructed airflow and normal gas exchange.
Bronchial Breath Sounds, in contrast, are normally heard only over the trachea and mainstem bronchi, specifically in the suprasternal notch and between the scapulae. These sounds are higher-pitched, louder, and more tubular in quality compared to vesicular sounds. Bronchial breath sounds are nearly equal in duration during inspiration and expiration, reflecting the larger diameter and central location of the airways involved. The inspiratory phase may be slightly higher-pitched due to the turbulence of air entering the trachea. In healthy individuals, bronchial sounds are not heard over peripheral lung fields, as this would indicate abnormal transmission of sound due to conditions like consolidation or increased airway secretions. Their presence in normal locations is a sign of healthy central airway function.
Broncho-vesicular Breath Sounds are intermediate in quality between vesicular and bronchial sounds. They are typically heard over the upper lobe areas of the lungs, such as the second and third intercostal spaces anteriorly. These sounds are medium in pitch and intensity, with a slightly louder and more bronchial quality during inspiration and a softer, more vesicular quality during expiration. The inspiratory phase is slightly longer than the expiratory phase, but not as prolonged as in vesicular sounds. Broncho-vesicular sounds occur in regions where larger bronchioles are closer to the chest wall, allowing for a blend of the two sound types. In healthy individuals, these sounds are clear and indicate normal airflow through the upper airway structures without obstruction or inflammation.
Understanding the characteristics of these normal breath sounds is crucial for distinguishing them from abnormal sounds that may indicate respiratory pathology. Vesicular, bronchial, and broncho-vesicular sounds each have distinct qualities that reflect the anatomy and physiology of the airways and alveoli. In healthy individuals, these sounds are consistent, clear, and free from adventitious noises. Clinicians use auscultation to assess these sounds, ensuring they are heard in the appropriate locations and with the expected qualities. Mastery of these normal breath sound patterns provides a baseline for identifying deviations that may signal underlying respiratory conditions.
In summary, normal breath sounds in healthy individuals are categorized into vesicular, bronchial, and broncho-vesicular types, each with unique characteristics. Vesicular sounds are soft, low-pitched, and predominate in peripheral lung fields. Bronchial sounds are louder, higher-pitched, and confined to central airways. Broncho-vesicular sounds are intermediate, blending features of both and typically heard in upper lobe regions. Recognizing these patterns is essential for clinical assessment, as deviations from normal can indicate airway obstruction, inflammation, or parenchymal disease. Proficiency in auscultation allows healthcare providers to detect early signs of respiratory abnormalities and guide appropriate interventions.
How Much Sound Do Earplugs Block? A Comprehensive Guide
You may want to see also
Explore related products






![]()
Adventitious Sounds: Types, causes, and descriptions of wheezes, crackles, rhonchi, and stridor
Adventitious Sounds: Types, Causes, and Descriptions
Adventitious breath sounds are abnormal lung sounds that indicate underlying respiratory conditions. These sounds are typically heard during inhalation or exhalation and can provide critical clues about the nature and location of the pathology. The most common adventitious sounds include wheezes, crackles (or rales), rhonchi, and stridor. Each has distinct characteristics, causes, and clinical implications.
Wheezes are high-pitched, whistling sounds that occur due to narrowed or obstructed airways. They are typically continuous and can be heard during both inhalation and exhalation, though they are often more prominent during expiration. Wheezes are commonly associated with conditions that cause airway constriction, such as asthma, chronic obstructive pulmonary disease (COPD), or bronchitis. The sound is produced by turbulent airflow through narrowed airways, often due to inflammation, mucus plugging, or bronchospasm. Wheezes can be localized to specific areas of the lung or diffuse, depending on the extent of airway obstruction.
Crackles (Rales) are discontinuous, popping or clicking sounds that resemble the noise of opening a bundle of hairpins. They are typically heard during inspiration and are caused by the sudden opening of small airways or alveoli filled with fluid, mucus, or pus. Crackles are classified as fine or coarse. Fine crackles are soft, brief, and high-pitched, often heard in interstitial lung diseases like pulmonary fibrosis or congestive heart failure. Coarse crackles are louder, lower-pitched, and longer-lasting, commonly associated with conditions like pneumonia or acute bronchitis. The presence of crackles suggests alveolar or small airway disease.
Rhonchi are low-pitched, snoring-like sounds that result from airflow turbulence through airways containing secretions or mucus. Unlike wheezes, rhonchi are usually heard during both phases of respiration and have a more coarse quality. They are often localized to specific areas of the lung and can be cleared by coughing. Rhonchi are commonly associated with chronic bronchitis, cystic fibrosis, or conditions causing excessive mucus production. The sound is produced by the vibration of airway walls as air passes through the narrowed, mucus-filled passages.
Stridor is a high-pitched, musical sound that occurs during inspiration and is indicative of upper airway obstruction. It is often described as a harsh, crowing noise and can be a medical emergency. Stridor is caused by turbulent airflow through a narrowed or partially blocked upper airway, such as the larynx, trachea, or large bronchi. Common causes include croup, epiglottitis, foreign body aspiration, or tumors. The sound is more pronounced during inspiration because the negative intrathoracic pressure exacerbates the narrowing. Immediate evaluation and intervention are necessary when stridor is present, as it can rapidly progress to complete airway obstruction.
Understanding the characteristics and causes of these adventitious sounds is essential for accurate diagnosis and management of respiratory conditions. Each sound provides unique insights into the location and nature of the underlying pathology, guiding clinicians in their assessment and treatment plans. Proper auscultation techniques and familiarity with these sounds are crucial for healthcare providers to effectively evaluate patients with respiratory symptoms.
How Sweet the Sound 2025: A Musical Journey to Remember
You may want to see also
Explore related products






![]()
Assessment Techniques: Proper use of stethoscope, positioning, and auscultation methods for accurate evaluation
Proper Use of Stethoscope for Accurate Breath Sound Assessment
The stethoscope is an essential tool for evaluating breath sounds, and its proper use is critical for accuracy. Begin by ensuring the stethoscope is in good condition—check for cracks in the tubing, proper diaphragm and bell function, and secure earpiece placement. Place the earpieces with the flat surface facing forward to create a tight seal, minimizing external noise interference. Adjust the headset tension for comfort and optimal sound transmission. When using the stethoscope, apply light pressure with the diaphragm for high-pitched sounds (e.g., normal breath sounds) and firmer pressure with the bell for low-pitched sounds (e.g., wheezes or rales). Avoid touching the patient’s clothing, as this can create artifactual noises that distort the assessment.
Patient Positioning for Optimal Auscultation
Proper patient positioning is key to accurately assessing breath sounds. The patient should be in a comfortable, relaxed position, ideally sitting upright or reclined at a 30- to 45-degree angle. This position allows for maximal chest expansion and minimizes muscle tension. For posterior lung fields, have the patient lean forward slightly or lie in a prone position. Ensure the patient is breathing normally and quietly, as forced breathing can alter sound characteristics. Instruct them to breathe through their mouth to reduce upper airway noise, which can obscure lung sounds. Proper positioning ensures access to all lung fields—anterior, posterior, lateral, and axillary—for a comprehensive evaluation.
Auscultation Techniques for Accurate Evaluation
Auscultation should be systematic and methodical to ensure no area is missed. Start at the lung apices and move downward to the bases, comparing corresponding lung fields bilaterally. Listen to each area for at least one full respiratory cycle, noting the inspiratory and expiratory phases. Use the diaphragm for high-frequency sounds and the bell for low-frequency sounds, ensuring a complete assessment of both. Pay attention to the intensity, pitch, duration, and quality of sounds. Normal breath sounds are soft and velvety (vesicular), while abnormal sounds include wheezes (high-pitched, whistling), rhonchi (low-pitched, rattling), crackles (brief, popping), and stridor (harsh, vibrating). Document findings immediately to avoid confusion between lung fields.
Minimizing Artifacts and Ensuring Clarity
Artifacts can significantly distort breath sound assessment, so take steps to minimize them. Ensure the stethoscope diaphragm or bell is in firm contact with the skin, avoiding clothing or jewelry. Ask the patient to remain still and quiet during auscultation, as movement or talking can introduce noise. Be mindful of environmental sounds, such as air conditioning or machinery, and position yourself to block these distractions. If using a stethoscope with dual heads, ensure the unused side is pointed downward to prevent sound interference. Finally, warm the stethoscope slightly before use, as cold metal can cause patient discomfort and muscle tension, altering breath sounds.
Systematic Approach to Lung Field Assessment
A systematic approach ensures thorough and accurate evaluation of all lung fields. Divide the chest into anatomical regions: upper and lower lobes, both anteriorly and posteriorly. Begin with the anterior fields, moving from the apex to the base, then proceed to the posterior fields, including the axillary regions. Compare findings between the left and right sides, noting asymmetry in sound quality or intensity. For example, decreased breath sounds may indicate consolidation or pneumothorax, while increased sounds can suggest airflow obstruction. Always reassess areas with abnormal findings to confirm consistency. This structured method ensures no critical information is overlooked and provides a clear, comprehensive assessment of breath sounds.
Unveiling the Magic: How Spatial Sounds Are Created in Audio
You may want to see also
Explore related products




![]()
Abnormal Patterns: Identifying diminished, absent, or asymmetrical breath sounds and their clinical significance
Abnormal breath sounds can provide critical insights into underlying respiratory conditions, making their identification and interpretation essential for clinical assessment. Diminished breath sounds occur when the intensity of air movement is reduced, often indicating a restriction in airflow or the presence of consolidated lung tissue. This can be observed in conditions such as pneumonia, where inflamed or fluid-filled alveoli impede air passage, or in cases of severe asthma or chronic obstructive pulmonary disease (COPD), where airway narrowing limits air movement. Clinically, diminished breath sounds suggest the need for further investigation, such as imaging studies, to identify the cause of the obstruction or consolidation.
Absent breath sounds are a more severe finding, where no air movement is audible during auscultation. This typically signifies a complete blockage or absence of air entry into a specific lung region. Common causes include pneumothorax, where air accumulates in the pleural space, collapsing the lung, or a large pleural effusion, which compresses the lung and prevents air entry. Absent breath sounds are also observed in cases of lung atelectasis, where the lung tissue collapses due to airway obstruction or surfactant deficiency. Identifying absent breath sounds is urgent, as these conditions often require immediate intervention, such as chest tube insertion or thoracentesis.
Asymmetrical breath sounds refer to differences in air movement between the left and right lungs or between different regions of the same lung. This asymmetry can result from localized pathology, such as a pulmonary embolism, which obstructs blood flow to a specific lung segment, or a foreign body lodged in one airway. Asymmetrical breath sounds may also be observed in patients with unilateral pneumonia or a lung mass. Clinically, asymmetry warrants a detailed history and further diagnostic tests, such as CT scans or bronchoscopy, to determine the underlying cause and guide appropriate management.
The clinical significance of these abnormal breath sounds lies in their ability to localize and characterize respiratory pathology. For instance, diminished or absent sounds in the lower lung fields may suggest a pneumonic consolidation or effusion, while asymmetrical sounds in the upper lobes could indicate a tumor or tuberculosis. Healthcare providers must correlate these findings with patient symptoms, medical history, and imaging results to formulate an accurate diagnosis. Early recognition of abnormal breath patterns can lead to timely interventions, improving patient outcomes and preventing complications.
In practice, auscultation should be performed systematically, comparing both lungs and noting any deviations from normal. The use of additional techniques, such as percussion to assess for dullness or hyper-resonance, can further enhance diagnostic accuracy. Understanding the clinical implications of diminished, absent, or asymmetrical breath sounds empowers clinicians to make informed decisions, ensuring targeted and effective patient care. Mastery of these auscultatory skills is fundamental for any healthcare professional involved in respiratory assessment.
Facetime: Unmute to Connect Better
You may want to see also
![]()
Documentation Tips: Clear, concise ways to record breath sound findings in medical notes
When documenting breath sounds in medical notes, clarity and precision are essential to ensure accurate communication among healthcare providers. Begin by noting the location where the breath sounds were auscultated, such as the lung fields (e.g., right upper lobe, left lower lobe). Use anatomical landmarks to specify the area, ensuring consistency and reproducibility for future assessments. For example, "Breath sounds auscultated over the posterior lung fields bilaterally." This provides a clear starting point for your documentation and sets the stage for detailed findings.
Next, describe the quality of the breath sounds using standardized terms. Common descriptors include vesicular (soft during inspiration, quiet during expiration), bronchial (louder during inspiration, similar to expiration), bronchovesicular (a blend of vesicular and bronchial), or absent/diminished if sounds are not heard. For abnormal findings, specify terms like rales (crackles), rhonchi (coarse rattling), wheezes (high-pitched whistling), or stridor (harsh, vibratory noise). For instance, "Vesicular breath sounds noted with occasional fine crackles at the right lung base." This approach ensures your documentation is both descriptive and clinically meaningful.
Quantify the intensity of breath sounds to provide additional context. Use terms such as normal, increased, decreased, or absent. For example, "Decreased breath sounds over the left lower lobe." If using a comparative scale, such as 1 to 3+ for intensity, include it for consistency. For instance, "Wheezes 2+ throughout all lung fields." This adds objectivity to your findings and aids in tracking changes over time.
Always document the symmetry and comparisons between lung fields. Note if breath sounds are equal bilaterally or if there are discrepancies, such as "Breath sounds diminished on the right compared to the left." This highlights asymmetry, which can be critical for diagnosing conditions like pneumothorax or consolidation. Additionally, mention any changes with patient position or respiratory phase if relevant, such as "Crackles more prominent during inspiration in the supine position."
Finally, include contextual information that may influence breath sound findings. Note the patient’s respiratory effort, such as labored breathing or use of accessory muscles, as this can impact auscultation. For example, "Breath sounds clear bilaterally, but patient exhibits tachypnea with mild retractions." Also, document any patient factors that could affect results, such as obesity, chest wall deformities, or poor cooperation. This ensures a comprehensive record that accounts for all variables influencing the assessment. By following these tips, your documentation will be clear, concise, and clinically valuable.
Unraveling the Mystery: How Sound Travels in the Vacuum of Space
You may want to see also
Frequently asked questions
Breath sounds are the noises produced by air moving through the respiratory tract during inhalation and exhalation. They are important to describe because they provide critical information about lung function, airflow, and potential respiratory conditions.
Normal breath sounds are soft, clear, and symmetrical between both lungs. Abnormal breath sounds may include wheezing, crackles, rhonchi, or stridor, which indicate issues like airway obstruction, fluid accumulation, or inflammation.
Wheezing is a high-pitched, whistling sound heard during inhalation or exhalation. It typically indicates narrowed or obstructed airways, often associated with conditions like asthma, COPD, or bronchitis.
Crackles are brief, popping sounds heard during inhalation. They suggest the presence of fluid, mucus, or inflammation in the small airways or alveoli, often seen in conditions like pneumonia or heart failure.
Rhonchi are low-pitched, rattling sounds heard during both inhalation and exhalation. They are associated with the presence of thick mucus or secretions in the larger airways, often seen in chronic bronchitis or cystic fibrosis.