Auscultation of breath sounds is a fundamental skill in clinical practice, allowing healthcare professionals to assess lung health and diagnose respiratory conditions. Using a stethoscope, practitioners listen to the sounds produced by air moving through the airways, which can reveal vital information about lung function. Proper technique involves placing the stethoscope’s diaphragm or bell on the patient’s chest or back, ensuring a quiet environment, and systematically listening to different lung fields. Normal breath sounds, such as vesicular and bronchial breathing, indicate healthy lung function, while abnormal sounds like wheezes, crackles, or stridor may suggest conditions like asthma, pneumonia, or obstructive airway diseases. Mastering auscultation requires practice, attention to detail, and an understanding of the anatomical and physiological principles underlying breath sounds.
Explore related products






What You'll Learn
- Preparation: Ensure patient comfort, expose chest, gather stethoscope, and confirm equipment functionality before starting auscultation
- Positioning: Place patient in optimal position (sitting, supine) for clear breath sound assessment
- Technique: Apply stethoscope lightly, move systematically across lung fields, listen for patterns
- Normal Sounds: Identify vesicular, bronchial, and tracheal breath sounds in healthy individuals
- Abnormal Sounds: Recognize crackles, wheezes, rhonchi, and stridor as indicators of respiratory issues
![]()
Preparation: Ensure patient comfort, expose chest, gather stethoscope, and confirm equipment functionality before starting auscultation
Before beginning the auscultation of breath sounds, it is essential to prioritize the patient's comfort to ensure a cooperative and relaxed environment. Start by explaining the procedure to the patient in simple terms, addressing any concerns or questions they may have. Position the patient in a comfortable posture, typically sitting upright or in a semi-recumbent position, as this facilitates easier breathing and access to the chest. Ensure the room is warm enough to prevent discomfort from exposure, and provide privacy by closing curtains or doors. A calm and reassuring demeanor from the healthcare provider can significantly ease patient anxiety, making the process smoother for both parties.
Next, gently expose the patient's chest to allow unobstructed access for auscultation. Ask the patient to remove any clothing or jewelry that might interfere with the examination, offering a gown or drape to maintain their dignity. For female patients, ensure the breasts are adequately exposed but covered when not being examined. Be mindful of cultural sensitivities and always maintain professionalism. Proper exposure of the chest is crucial as it enables comprehensive assessment of all lung fields without unnecessary interruptions during the procedure.
Gathering the necessary equipment, primarily a stethoscope, is the next critical step. Ensure the stethoscope is clean and in good working condition. Check the earpieces for debris and wipe the diaphragm and bell with an alcohol swab to maintain hygiene. Adjust the headset for a comfortable fit, ensuring the earpieces are angled correctly to seal out external noise. If using an electronic stethoscope, verify the battery life and power it on to confirm functionality. Having a functional stethoscope is fundamental to accurately detecting and interpreting breath sounds.
Before placing the stethoscope on the patient, confirm its functionality by testing it on a reliable sound source, such as a humming sound or a watch with a second hand. This quick check ensures the stethoscope is amplifying sounds correctly and that both earpieces are working. If any issues are detected, such as muffled sounds or a loose headset, address them immediately by adjusting or replacing the equipment. A properly functioning stethoscope is indispensable for obtaining clear and accurate auscultation results.
Finally, organize any additional materials that may be needed during the examination, such as a diagram of lung fields or a notepad for recording findings. Ensure the area is well-lit and free of clutter to maintain focus on the task. By systematically preparing the patient, exposing the chest, gathering and testing the stethoscope, and organizing ancillary tools, you create an efficient and professional environment for auscultating breath sounds. This thorough preparation not only enhances the accuracy of the examination but also demonstrates respect for the patient's comfort and time.
Exploring Underwater Sound Waves: A Simple Experiment to Try
You may want to see also
Explore related products






![]()
Positioning: Place patient in optimal position (sitting, supine) for clear breath sound assessment
When preparing to auscultate breath sounds, proper patient positioning is crucial for obtaining clear and accurate results. The optimal position depends on the patient’s comfort and the specific lung areas you need to assess. Sitting upright is generally the preferred position for most patients, as it allows for maximal lung expansion and minimizes the effort required for breathing. Instruct the patient to sit on the edge of the bed or in a chair with their back straight and shoulders relaxed. This position facilitates easy access to both the anterior and posterior chest walls, ensuring comprehensive auscultation. Encourage the patient to place their arms loosely at their sides or on their lap to avoid tension in the chest muscles, which could interfere with sound transmission.
For patients who are unable to sit upright due to weakness, pain, or other limitations, the supine position (lying flat on the back) is an alternative. In this position, the patient should lie on a flat surface with their head supported by a pillow to maintain a neutral neck position. Ensure the room is warm to prevent discomfort, as lying supine can expose more of the patient’s body. When auscultating in the supine position, begin with the anterior chest wall, moving methodically from the apex to the base. Note that breath sounds may be slightly diminished in this position due to the effects of gravity on lung tissue, particularly in the posterior lung fields.
In some cases, lateral positioning may be necessary to assess specific lung segments. For example, to auscultate the posterior basal segments, you can ask the patient to lie on their side with the area of interest facing upward. This position helps to isolate and amplify sounds from the dependent lung regions. Ensure the patient is comfortable and supported with pillows to maintain the position without strain. Clear communication is key; explain the purpose of the position and provide reassurance to encourage cooperation.
Regardless of the position chosen, ensure the patient is relaxed and breathing normally. Avoid positions that cause discomfort or restrict breathing, as this can alter breath sounds and lead to inaccurate assessments. Always prioritize the patient’s safety and comfort while maintaining the integrity of the auscultation process. Proper positioning not only enhances the clarity of breath sounds but also demonstrates respect for the patient’s well-being, fostering trust and cooperation during the examination.
Finally, consider the patient’s medical condition when selecting the optimal position. For instance, patients with orthopnea (difficulty breathing when lying flat) should not be placed supine, as this can exacerbate their symptoms. Similarly, patients with musculoskeletal issues may require additional support or modifications to achieve a comfortable and effective position. By tailoring the position to the patient’s needs, you ensure a thorough and patient-centered auscultation of breath sounds.
What Does Deafness Sound Like? Exploring the Silence Within
You may want to see also
Explore related products






![]()
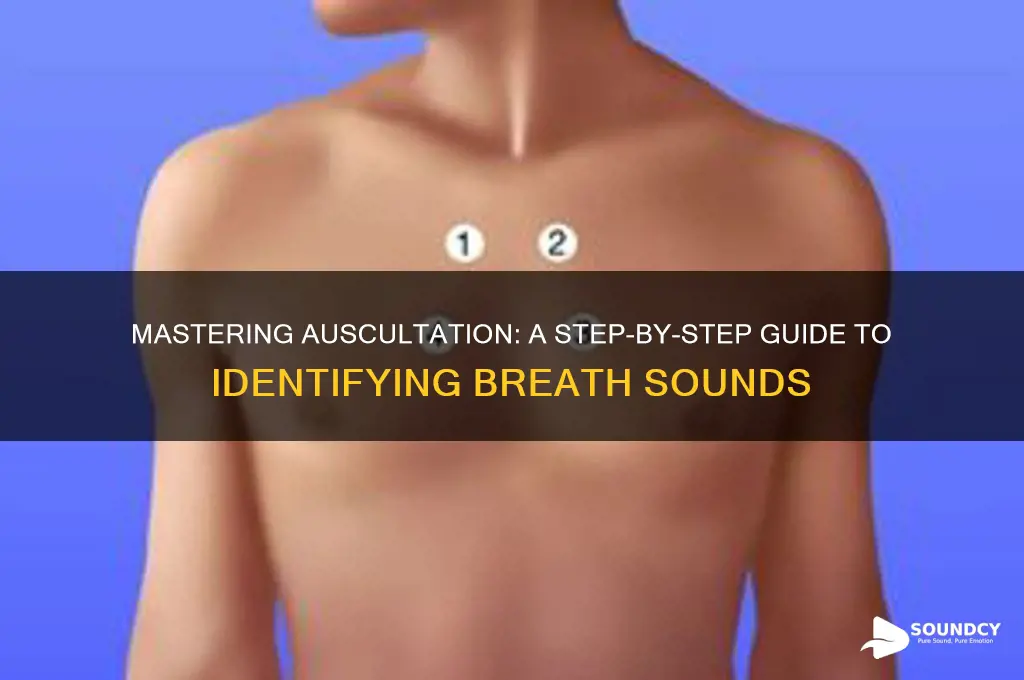
Technique: Apply stethoscope lightly, move systematically across lung fields, listen for patterns
To effectively auscultate breath sounds, begin by applying the stethoscope lightly to the patient’s skin. Excessive pressure can alter the sounds or create artifacts, so ensure the diaphragm or bell of the stethoscope rests gently on the chest wall. Start at the apex of the lung (the uppermost part) and maintain minimal contact to capture clear, unmuffled sounds. The goal is to create an airtight seal without causing discomfort to the patient. This light touch allows for accurate detection of both high-pitched and low-pitched breath sounds.
Next, move systematically across the lung fields to ensure comprehensive coverage. Divide the lungs into anatomical regions: the anterior, posterior, and lateral chest walls. Begin at the apex and move downward in a consistent pattern, such as from top to bottom and side to side. Spend 5–10 seconds at each location to listen carefully. Systematic movement ensures no area is missed and helps identify localized abnormalities. For example, start at the first intercostal space and progress through each intercostal space, moving from one lung field to the next.
As you auscultate, listen for patterns in the breath sounds. Normal breath sounds include vesicular (soft during inspiration, quieter during expiration) and tracheal (equal inspiration and expiration) sounds. Pay attention to their intensity, pitch, and duration. Abnormal sounds, such as wheezes, crackles, or stridor, indicate specific conditions like asthma, pneumonia, or airway obstruction. Note if the sounds are continuous, intermittent, or localized to a particular area. Comparing sounds across lung fields helps identify asymmetry or abnormalities.
Maintain a rhythmic and deliberate pace while moving the stethoscope. Rushing can lead to missing subtle changes, while moving too slowly may fatigue both you and the patient. Keep the patient in a comfortable position, such as sitting upright or supine, to optimize sound transmission. Encourage them to breathe naturally and deeply to capture both inspiratory and expiratory phases clearly. Coordination with the patient’s breathing cycle is key to accurate auscultation.
Finally, document your findings systematically. Note the location, quality, and characteristics of the breath sounds for each lung field. For example, record whether vesicular sounds are normal or if crackles are heard in the lung bases. This detailed documentation aids in diagnosis and monitoring of respiratory conditions. Consistent technique and attention to patterns ensure a thorough and reliable auscultation process.
How Birdsong Can Improve Your Mental Health
You may want to see also
Explore related products





![]()
Normal Sounds: Identify vesicular, bronchial, and tracheal breath sounds in healthy individuals
Auscultation of breath sounds is a fundamental skill in assessing respiratory health, and recognizing normal lung sounds is crucial for identifying abnormalities. In healthy individuals, three primary breath sounds are auscultated: vesicular, bronchial, and tracheal sounds. Each sound has distinct characteristics based on its location and the anatomy of the airways. Understanding these differences is essential for accurate interpretation during auscultation.
Vesicular breath sounds are the most common and are heard over most of the lung fields in healthy individuals. These sounds are soft, low-pitched, and rustling, resembling the sound of air moving through a forest. They are produced by air flowing through the alveoli and smaller bronchioles. Vesicular sounds are typically longer during inspiration than expiration and are best heard in the peripheral lung zones. To identify them, place the stethoscope over the anterior, lateral, or posterior chest wall, and listen for a gentle, continuous sound that increases slightly in intensity during inspiration.
Bronchial breath sounds, in contrast, are higher-pitched and more intense than vesicular sounds. They are normally heard only over the trachea and mainstem bronchi, specifically in the suprasternal notch and between the scapulae. Bronchial sounds are characterized by equal duration during inspiration and expiration, often described as "hollow" or "tubular." In healthy individuals, these sounds should not be heard in peripheral lung fields. To auscultate bronchial sounds, position the stethoscope over the designated areas and listen for a clear, high-pitched quality that remains consistent throughout the respiratory cycle.
Tracheal breath sounds are a subset of bronchial sounds, specifically auscultated over the trachea. They are the loudest and most high-pitched of the three normal sounds, with a distinct "barking" quality. Tracheal sounds are best heard over the suprasternal notch and are characterized by equal phases of inspiration and expiration. These sounds are normal when heard over the trachea but are abnormal if detected in other lung areas. Proper positioning of the stethoscope is critical to accurately identifying tracheal sounds.
In summary, identifying normal breath sounds requires careful attention to pitch, intensity, and duration. Vesicular sounds are soft and rustling, heard over most lung fields; bronchial sounds are higher-pitched and tubular, normally confined to central airways; and tracheal sounds are the loudest and most high-pitched, auscultated over the trachea. Mastery of these distinctions ensures accurate assessment of respiratory health and aids in detecting abnormalities during auscultation. Practice and familiarity with these sounds are key to becoming proficient in this essential clinical skill.
Exploring GoPro's Audio Quality: Capturing Clear Sound in Action Shots
You may want to see also
Explore related products






![]()
Abnormal Sounds: Recognize crackles, wheezes, rhonchi, and stridor as indicators of respiratory issues
When auscultating breath sounds, it's crucial to recognize abnormal sounds that may indicate underlying respiratory issues. Crackles are one of the most common abnormal sounds, often described as brief, popping, or bubbling noises that occur during inhalation. They are typically heard in patients with conditions such as pneumonia, heart failure, or pulmonary fibrosis. Crackles result from the opening of airways filled with fluid, mucus, or other secretions. To identify them, listen carefully during the inspiratory phase, especially in the lung bases, as they are more prominent in these areas.
Wheezes are another significant abnormal sound, characterized by high-pitched, whistling noises that occur during both inspiration and expiration. They are most commonly associated with asthma, chronic obstructive pulmonary disease (COPD), or bronchitis. Wheezes indicate narrowed or partially obstructed airways, often due to inflammation, mucus plugging, or bronchospasm. When auscultating, pay attention to their pitch, duration, and whether they are localized or widespread, as these features can help differentiate the underlying cause.
Rhonchi are low-pitched, rattling sounds that resemble snoring and are typically heard during expiration. They are caused by the movement of air through airways containing thick secretions or mucus. Rhonchi are often associated with conditions like chronic bronchitis, COPD, or cystic fibrosis. Unlike wheezes, rhonchi are usually louder and more continuous. To detect them, focus on the expiratory phase and note if the sound is localized or diffuse, as this can provide clues about the extent of airway involvement.
Stridor is a high-pitched, musical sound that occurs during inspiration and, less commonly, expiration. It is a critical finding that suggests severe upper airway obstruction, often due to conditions such as laryngeal edema, foreign body aspiration, or tumors. Stridor requires immediate attention, as it can rapidly progress to respiratory distress. When auscultating, stridor is typically heard over the neck or suprasternal notch, and its presence should prompt urgent evaluation and intervention.
Recognizing these abnormal sounds—crackles, wheezes, rhonchi, and stridor—is essential for accurate diagnosis and management of respiratory conditions. Each sound has distinct characteristics related to pitch, timing, and location, which help differentiate the underlying pathology. During auscultation, use a systematic approach, listening to both inspiratory and expiratory phases in all lung fields. Correlate your findings with the patient’s history and symptoms to guide appropriate treatment and referral. Mastery of these auscultation skills enhances clinical decision-making and improves patient outcomes.
Finding Peace: How Sweet the Sound of a Stable Center
You may want to see also
Frequently asked questions
Position the patient comfortably (sitting or lying down), ensure the stethoscope diaphragm or bell is properly sealed on the chest wall, and listen systematically across lung fields (anterior, posterior, and lateral). Avoid talking or moving during auscultation to minimize interference.
Normal breath sounds include vesicular (soft during inspiration, quieter during expiration) and bronchial (equal intensity in both phases). Abnormal sounds include wheezes (high-pitched whistles), crackles (rattling or popping), and stridor (harsh, vibrating noise), which indicate conditions like asthma, pneumonia, or airway obstruction.
Auscultate over the trachea (for stridor), lung fields (upper, mid, and lower zones), and areas where specific pathology is suspected (e.g., crackles in the bases for pneumonia). Compare bilateral sounds to identify asymmetry or abnormalities.