The cardiac cycle, which is the sequence of events that occurs as the heart beats, involves the contraction and relaxation of the heart chambers to pump blood throughout the body. During this cycle, specific heart sounds can be heard, which are crucial for assessing cardiac function. Typically, two primary heart sounds, often described as lub (S1) and dub (S2), occur during each cardiac cycle. S1 is produced by the closure of the mitral and tricuspid valves at the start of systole, while S2 results from the closure of the aortic and pulmonary valves at the beginning of diastole. These sounds are essential for diagnosing cardiovascular conditions and understanding the heart's mechanical performance.
| Characteristics | Values |
|---|---|
| Number of Heart Sounds per Cardiac Cycle | Typically 2 (S1 and S2) |
| First Heart Sound (S1) | Occurs at the beginning of systole, caused by closure of AV valves |
| Second Heart Sound (S2) | Occurs at the beginning of diastole, caused by closure of semilunar valves |
| Additional Sounds (Rare) | S3 (early diastolic) and S4 (late diastolic) may occur in certain conditions |
| Duration of Cardiac Cycle | Approximately 0.8 seconds at a resting heart rate of 75 beats per minute |
| Clinical Significance | Abnormalities in heart sounds can indicate valve disorders or cardiac dysfunction |
Explore related products


$29.59 $36.99




What You'll Learn
- First Heart Sound (S1): Marks mitral/tricuspid valve closure, beginning systole, loud lub sound
- Second Heart Sound (S2): Indicates aortic/pulmonic valve closure, end systole, softer dub sound
- Normal Heart Sounds: Two distinct sounds (S1, S2) per cardiac cycle, rhythmic and clear
- Extra Heart Sounds: Third/fourth heart sounds (S3, S4) may indicate pathology if present
- Absence of Sounds: Missing S1 or S2 suggests valve dysfunction or cardiac abnormalities
![]()
First Heart Sound (S1): Marks mitral/tricuspid valve closure, beginning systole, loud lub sound
The first heart sound, often referred to as S1, is a critical marker in the cardiac cycle, signaling the closure of the mitral and tricuspid valves. This event coincides with the beginning of systole, the phase when the heart contracts to pump blood out of the ventricles. S1 is characterized by its distinct "lub" sound, which is typically louder and lower in pitch compared to the second heart sound (S2). This sound is produced by the rapid increase in pressure within the ventricles, causing the atrioventricular (AV) valves to snap shut. Understanding S1 is essential for healthcare professionals, as it provides valuable insights into the heart's mechanical function and can help diagnose various cardiac conditions.
From an analytical perspective, S1 serves as a temporal anchor in the cardiac cycle, dividing it into systole and diastole. It occurs at the end of ventricular filling, when the pressure in the ventricles exceeds that in the atria, forcing the AV valves to close. This closure prevents backflow of blood into the atria and ensures efficient forward flow into the aorta and pulmonary artery. Clinicians often use the timing and quality of S1 to assess valve function and ventricular performance. For instance, a split S1 can indicate delayed closure of one of the AV valves, potentially pointing to issues like bundle branch block or valve dysfunction.
Instructively, auscultating S1 requires proper technique and attention to detail. Place the diaphragm of the stethoscope on the chest at the mitral (fifth left intercostal space at the midclavicular line) or tricuspid (left lower sternal border) areas. Listen for the abrupt, low-pitched "lub" sound, which should be clearly audible in healthy individuals. For pediatric patients, use a smaller stethoscope head and apply gentle pressure to ensure optimal sound transmission. Teaching medical students and trainees to differentiate S1 from S2 is crucial, as this skill forms the foundation of cardiac auscultation.
Persuasively, recognizing the significance of S1 can empower both healthcare providers and patients. For providers, it underscores the importance of routine cardiac auscultation in detecting early signs of heart disease. For patients, understanding this sound can demystify the cardiac cycle and encourage proactive engagement in their cardiovascular health. For example, individuals with conditions like mitral valve prolapse may notice changes in the quality of S1, prompting timely medical evaluation. This awareness can lead to earlier interventions and better outcomes.
Comparatively, while S1 marks the beginning of systole, the second heart sound (S2) signifies the end of systole and the onset of diastole. S2 is associated with the closure of the aortic and pulmonary valves and produces a higher-pitched "dub" sound. The relationship between S1 and S2 is crucial for assessing heart rhythm and valve timing. For instance, a widened split between S1 and S2 can indicate conditions like left bundle branch block or hypertension. By contrast, a paradoxically split S2 may suggest right bundle branch block or pulmonary hypertension. Mastery of these distinctions enhances diagnostic accuracy and clinical decision-making.
In conclusion, the first heart sound (S1) is a fundamental component of the cardiac cycle, marking the closure of the mitral and tricuspid valves and the onset of systole. Its distinct "lub" sound provides critical information about valve function and ventricular performance. By understanding S1, healthcare professionals can improve diagnostic precision, while patients can gain a deeper appreciation of their heart health. Whether through analytical assessment, instructional techniques, persuasive advocacy, or comparative analysis, S1 remains a cornerstone of cardiac auscultation and clinical practice.
Mastering MP3 Conversion: A Step-by-Step Guide to Formatting Sound
You may want to see also
Explore related products






![]()
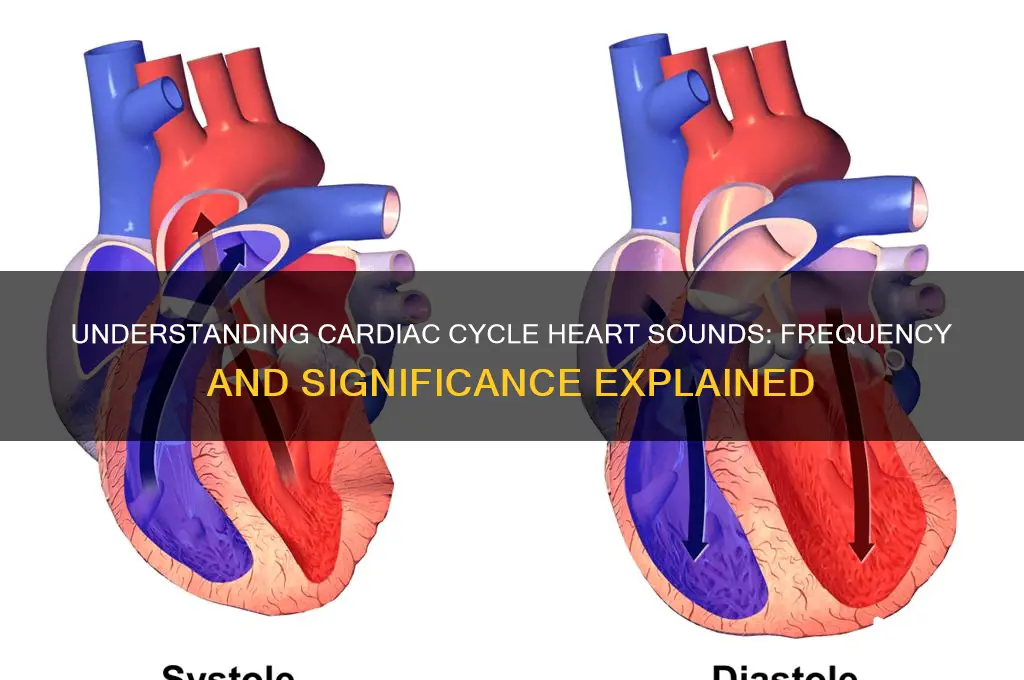
Second Heart Sound (S2): Indicates aortic/pulmonic valve closure, end systole, softer dub sound
The second heart sound, often abbreviated as S2, is a critical marker in the cardiac cycle, signaling the closure of the aortic and pulmonic valves. This event marks the end of systole, the phase when the heart contracts to pump blood into the aorta and pulmonary artery. Unlike the first heart sound (S1), which is characterized by a louder "lub," S2 produces a softer "dub" sound. This distinction is essential for clinicians using auscultation to assess heart function, as it provides insights into the timing and efficiency of valve closure.
Analyzing S2 in detail reveals its diagnostic significance. The sound is split into two components: the aortic valve closure (A2) and the pulmonic valve closure (P2). In a healthy heart, P2 slightly precedes A2, creating a single, blended sound. However, in certain conditions like pulmonary hypertension or right bundle branch block, the split between A2 and P2 becomes more pronounced, known as a "widened split." Recognizing these variations is crucial for identifying underlying cardiac issues. For instance, a paradoxical split (A2 before P2) may indicate left bundle branch block or severe left ventricular dysfunction.
From a practical standpoint, healthcare providers can enhance their auscultation skills by focusing on the intensity and quality of S2. Using a diaphragm stethoscope placed over the pulmonic area (second left intercostal space) and the aortic area (third right intercostal space) allows for clear detection of S2 components. Patients should be in a supine or sitting position, and the examiner should listen during both inspiration and expiration, as respiratory phase can affect the split. For example, during inspiration, the split widens due to increased blood return to the right heart, a phenomenon known as respiratory splitting.
Comparatively, while S1 is associated with the forceful closure of the mitral and tricuspid valves, S2 is more subtle yet equally informative. Its softer quality requires a keen ear and a systematic approach to auscultation. For medical students and practitioners, mastering the identification of S2 is a foundational skill. It not only confirms the end of systole but also serves as a window into the dynamics of valve function and cardiovascular health. Regular practice and correlation with other diagnostic tools, such as echocardiography, can refine this skill and improve patient outcomes.
In conclusion, the second heart sound (S2) is a vital indicator of aortic and pulmonic valve closure, marking the transition from systole to diastole. Its softer "dub" sound, though less pronounced than S1, carries significant diagnostic value. By understanding its components, variations, and clinical implications, healthcare providers can better assess cardiac function and identify potential abnormalities. Whether in a routine checkup or a complex cardiac evaluation, S2 remains an indispensable tool in the auscultation arsenal.
Unveiling the Silent Mystery: What Sound Has 0 Decibels?
You may want to see also
Explore related products






![]()
Normal Heart Sounds: Two distinct sounds (S1, S2) per cardiac cycle, rhythmic and clear
During a normal cardiac cycle, the heart produces two distinct sounds, often referred to as S1 and S2. These sounds are rhythmic, clear, and serve as vital indicators of cardiovascular health. S1, the first heart sound, occurs when the mitral and tricuspid valves close at the beginning of systole, marking the start of ventricular contraction. S2, the second heart sound, follows during early diastole, resulting from the closure of the aortic and pulmonary valves as the ventricles relax. Understanding these sounds is essential for healthcare professionals to assess heart function and identify potential abnormalities.
To appreciate the significance of S1 and S2, consider their timing and characteristics. S1 is typically low-pitched and longer in duration, often described as a "lub" sound. It coincides with the carotid pulse and is best heard at the mitral and tricuspid areas of the chest. S2, higher-pitched and shorter, is likened to a "dub" sound and is most audible at the aortic and pulmonary areas. The interval between S1 and S2 corresponds to systole, while the period between S2 and the next S1 represents diastole. Clinicians use this rhythm to evaluate heart rate, valve function, and overall cardiac efficiency.
For practical application, auscultation with a stethoscope is the primary method to detect these sounds. Place the stethoscope over the appropriate chest areas, ensuring minimal ambient noise. In adults, a normal heart rate ranges from 60 to 100 beats per minute, with each beat producing a clear S1 and S2. Deviations, such as splitting of S2 (a delay between aortic and pulmonary valve closure) or the presence of extra sounds, may indicate conditions like valve disorders or hypertension. Regular monitoring, especially in high-risk populations like the elderly or those with cardiovascular history, is crucial for early detection.
Comparatively, abnormal heart sounds, such as murmurs or gallops (S3, S4), differ in timing, pitch, and quality. While S1 and S2 are consistent and rhythmic, murmurs may be continuous or systolic/diastolic, often signaling valve leakage or stenosis. Gallops, though rare in healthy individuals, suggest increased ventricular volume or decreased compliance. Recognizing the distinction between normal and abnormal sounds is key to accurate diagnosis and timely intervention. For instance, a systolic murmur in a child could indicate a congenital heart defect, whereas an S3 gallop in an adult might point to heart failure.
In conclusion, the two distinct heart sounds, S1 and S2, are the cornerstone of cardiac auscultation. Their rhythmic and clear nature provides a baseline for assessing heart health. By mastering their identification and understanding their implications, healthcare providers can effectively screen for cardiovascular issues. For individuals, awareness of these sounds encourages proactive monitoring, particularly during routine check-ups. Whether in a clinical setting or personal health management, recognizing S1 and S2 is a fundamental skill that bridges observation and action in cardiovascular care.
Understanding Light and Sound Reflection
You may want to see also
Explore related products






![]()
Extra Heart Sounds: Third/fourth heart sounds (S3, S4) may indicate pathology if present
The typical cardiac cycle produces two heart sounds, often described as "lub-dub," which correspond to the closing of the atrioventricular (S1) and semilunar (S2) valves. However, the presence of additional sounds, such as S3 or S4, can signal underlying cardiac issues. These extra sounds are not part of a normal cycle and warrant careful evaluation.
Identifying S3 and S4: A Practical Approach
To detect these sounds, use a stethoscope with the bell placed over the cardiac apex. S3 occurs shortly after S2, often described as a soft, low-pitched "ventricular gallop," while S4 precedes S1 and sounds like a dull thud, sometimes termed an "atrial gallop." Both are best heard in the left lateral decubitus position with held breath. S3 is more common in children and young adults, where it may be benign, but in older individuals or those with heart failure, it suggests volume overload or reduced compliance. S4, in contrast, is rarely normal and often indicates diastolic dysfunction, such as hypertrophic cardiomyopathy or aortic stenosis.
Clinical Implications and Red Flags
The presence of S3 or S4 should prompt further investigation. For S3, consider echocardiography to assess left ventricular function and filling pressures, especially if accompanied by symptoms like fatigue or dyspnea. S4 requires evaluation for causes of elevated left ventricular stiffness, such as hypertension or ischemic heart disease. In both cases, a detailed history and physical exam are critical to differentiate pathological from physiological causes.
Management Strategies: Tailored to the Underlying Cause
Treatment focuses on addressing the root pathology. For S3 associated with heart failure, diuretics and ACE inhibitors may reduce volume overload. S4 often necessitates managing conditions like hypertension or aortic stenosis, potentially involving beta-blockers or surgical intervention. Regular monitoring of heart sounds and cardiac biomarkers is essential to track disease progression or response to therapy.
Prevention and Patient Education
Encourage patients to maintain a heart-healthy lifestyle, including regular exercise, a low-sodium diet, and blood pressure control, to minimize the risk of developing conditions that cause extra heart sounds. Educate them on symptoms like chest discomfort or shortness of breath, which should prompt immediate medical attention. Early detection and intervention can prevent complications and improve long-term outcomes.
Does Bronchitis Cause Crackling Sounds? Unraveling the Respiratory Mystery
You may want to see also
Explore related products






![]()
Absence of Sounds: Missing S1 or S2 suggests valve dysfunction or cardiac abnormalities
The absence of heart sounds S1 or S2 is a critical indicator of potential cardiac issues, particularly valve dysfunction. Normally, a healthy cardiac cycle produces two distinct sounds: S1, associated with the closure of the mitral and tricuspid valves, and S2, linked to the closure of the aortic and pulmonary valves. When either of these sounds is missing, it signals an abnormality that demands immediate medical attention. For instance, a missing S1 could suggest mitral valve prolapse or stenosis, while an absent S2 might indicate aortic stenosis or regurgitation. Recognizing these absences during auscultation is the first step in diagnosing underlying conditions that could compromise heart function.
To assess the absence of S1 or S2, healthcare providers use a systematic approach. Begin by positioning the patient in a supine or left lateral decubitus position to optimize sound detection. Use a stethoscope with the bell for low-pitched sounds and the diaphragm for high-pitched sounds. Listen carefully at the appropriate auscultation points: the mitral area for S1 and the aortic area for S2. If either sound is absent, document the finding and correlate it with other symptoms such as murmurs, shortness of breath, or chest pain. For example, a missing S1 accompanied by a systolic murmur may point to mitral valve disease, while an absent S2 with a diastolic murmur could indicate aortic valve dysfunction.
The implications of missing heart sounds extend beyond diagnosis; they guide treatment decisions. For instance, a missing S1 in a young adult might warrant an echocardiogram to evaluate mitral valve structure and function. In older adults, an absent S2 could prompt further investigation into aortic valve calcification or stenosis, particularly if risk factors like hypertension or smoking are present. Practical tips for patients include maintaining regular follow-ups, monitoring symptoms like fatigue or dizziness, and adopting heart-healthy habits such as a low-sodium diet and regular exercise. Early detection and intervention are key to preventing complications like heart failure or arrhythmias.
Comparatively, the absence of S1 or S2 stands in stark contrast to the presence of extra heart sounds, such as S3 or S4, which indicate different pathologies. While extra sounds often signify ventricular overload or dysfunction, missing sounds directly implicate valve abnormalities. This distinction underscores the importance of precise auscultation skills. For medical professionals, mastering the art of identifying absent sounds is as crucial as recognizing additional ones. Training should include simulated auscultation exercises and real-world practice to enhance diagnostic accuracy. For patients, understanding the significance of these sounds empowers them to seek timely care when abnormalities are detected.
In conclusion, the absence of S1 or S2 is a red flag for valve dysfunction or cardiac abnormalities, requiring prompt evaluation and intervention. By combining careful auscultation with diagnostic tools and patient education, healthcare providers can address these issues effectively. Whether in a clinical setting or during routine check-ups, recognizing missing heart sounds is a vital skill that can significantly impact patient outcomes. Practical steps, from proper positioning to symptom monitoring, ensure that these subtle yet critical indicators are not overlooked.
Unveiling the Mridangam's Magic: How Its Structure Creates Sound
You may want to see also
Frequently asked questions
A typical cardiac cycle includes two heart sounds: S1 (first heart sound) and S2 (second heart sound).
S1 is caused by the closure of the mitral and tricuspid valves at the start of systole, while S2 is caused by the closure of the aortic and pulmonary valves at the start of diastole.
In a normal cardiac cycle, only S1 and S2 are present. Additional sounds like S3 or S4 may indicate pathological conditions or specific physiological states.