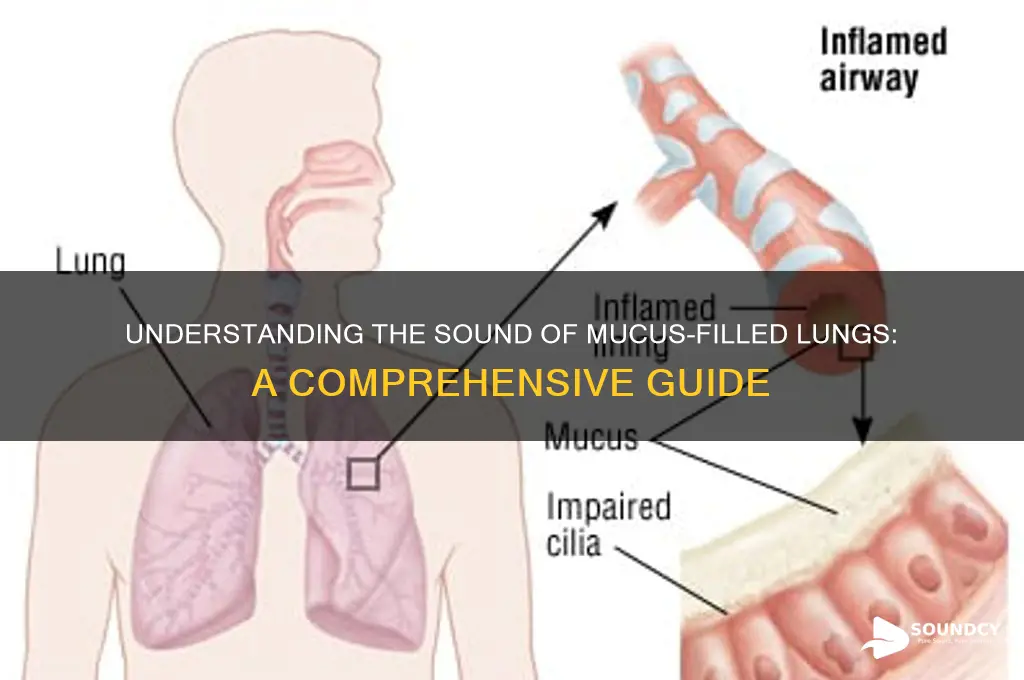
When mucus accumulates in the vocal cords, it can significantly alter the sound of the voice, often resulting in a muffled, congested, or gurgly tone. This occurs because the mucus creates a barrier between the vocal folds, disrupting their ability to vibrate freely and produce clear sounds. The presence of mucus can also lead to a sensation of heaviness or strain in the throat, further affecting speech quality. Understanding how mucus impacts vocal production is essential for identifying and addressing underlying issues, such as respiratory infections, allergies, or sinusitis, which may contribute to this phenomenon.
Explore related products






What You'll Learn
- Mucus Consistency Impact: Thick mucus creates deeper, gurgling sounds; thin mucus produces softer, wetter noises
- Airflow Obstruction: Mucus blocks airways, causing whistling, rattling, or bubbling sounds during breathing
- Cough Variations: Wet coughs expel mucus with loud, phlegmy sounds; dry coughs are sharper, less resonant
- Lung Region Effects: Upper airway mucus sounds higher-pitched; lower lung mucus sounds deeper and more resonant
- Infection Influence: Infected mucus often produces louder, more persistent gurgling or crackling sounds
![]()
Mucus Consistency Impact: Thick mucus creates deeper, gurgling sounds; thin mucus produces softer, wetter noises
The consistency of mucus in the lungs plays a significant role in the types of sounds produced during breathing. Thick mucus, often associated with conditions like chronic bronchitis or cystic fibrosis, tends to create deeper, gurgling sounds. This occurs because the denser mucus requires more force to move through the airways, resulting in audible vibrations as it shifts. These sounds are typically more pronounced during exhalation, as the air tries to push past the sticky, viscous material. Healthcare providers often describe these noises as "rattling" or "gurgling," which can be a clear indicator of mucus buildup in the lower respiratory tract.
In contrast, thin mucus produces softer, wetter noises due to its lower viscosity. This type of mucus is more easily mobilized and tends to flow more freely through the airways. The sounds associated with thin mucus are often described as "wet" or "muffled," resembling a gentle bubbling or splashing. These noises are usually less intense than those caused by thick mucus, as the thinner consistency allows air to pass with less resistance. Thin mucus is commonly observed in early stages of respiratory infections or allergies, where the body is actively trying to clear irritants.
Understanding the mucus consistency impact is crucial for both patients and healthcare providers. For instance, a patient with thick mucus may require interventions like chest physiotherapy or mucolytic medications to help loosen and expel the mucus, thereby reducing the deep gurgling sounds. On the other hand, thin mucus may resolve with hydration and mild expectorants, as the softer, wetter noises often indicate a less severe obstruction. Recognizing these distinctions can guide appropriate treatment and management strategies.
The impact of mucus consistency on lung sounds also highlights the importance of listening carefully during auscultation. Medical professionals use stethoscopes to differentiate between the deeper, gurgling sounds of thick mucus and the softer, wetter noises of thin mucus. This auditory assessment, combined with patient history and other diagnostic tools, helps in accurately identifying the underlying cause of respiratory symptoms. For example, persistent gurgling may suggest a chronic condition, while transient wet sounds could indicate an acute issue.
In summary, the mucus consistency impact directly influences the sounds produced by the lungs. Thick mucus generates deeper, gurgling sounds due to its resistance to airflow, while thin mucus results in softer, wetter noises as it moves more freely. Recognizing these auditory cues is essential for diagnosing and managing respiratory conditions effectively. Patients and healthcare providers alike can benefit from understanding how mucus consistency affects lung sounds, enabling timely and targeted interventions.
Adjusting Spotify Sound: Tips and Tricks
You may want to see also
Explore related products






![]()
Airflow Obstruction: Mucus blocks airways, causing whistling, rattling, or bubbling sounds during breathing
When mucus accumulates in the airways, it can lead to significant airflow obstruction, resulting in distinctive sounds during breathing. These sounds are often described as whistling, rattling, or bubbling, and they occur due to the turbulent airflow as it tries to pass through the narrowed or partially blocked passages. The whistling sound, known as wheezing, is typically high-pitched and occurs when air is forced through a constricted area. This is commonly heard in conditions like asthma or chronic obstructive pulmonary disease (COPD), where mucus exacerbates the narrowing of the airways. Understanding these sounds is crucial for identifying the presence of mucus-related obstruction and determining the appropriate intervention.
Rattling sounds, often referred to as rhonchi, are another manifestation of mucus-induced airflow obstruction. These low-pitched, snore-like noises are produced when air moves past mucus or other secretions in the larger airways, such as the bronchi. Unlike wheezing, rhonchi are often heard during both inhalation and exhalation, though they may be more prominent during exhalation. Patients with conditions like bronchitis or pneumonia frequently exhibit rhonchi due to the increased production of mucus in the airways. Clearing this mucus through techniques like chest physiotherapy or coughing can help alleviate these sounds and improve breathing.
Bubbling sounds, or gurgling, are often associated with mucus in the lower airways or the presence of fluid in the lungs. This sound occurs when air passes through mucus-filled passages or when there is a mix of air and fluid in the respiratory tract. Gurgling is particularly concerning as it may indicate a more severe obstruction or the presence of infection. Patients with conditions like cystic fibrosis or those recovering from surgery may experience bubbling sounds due to excessive mucus production or inadequate clearance. Prompt assessment and management, including mucus-clearing techniques and medications, are essential to prevent complications.
The intensity and frequency of these sounds can vary depending on the amount and location of mucus in the airways. For instance, wheezing may be intermittent and mild in the early stages of mucus buildup but can become continuous and severe as the obstruction worsens. Similarly, rhonchi and bubbling sounds may be localized to one area of the lung or widespread, depending on the distribution of mucus. Healthcare providers often use auscultation with a stethoscope to assess these sounds, as their characteristics can provide valuable insights into the underlying condition and guide treatment decisions.
Managing airflow obstruction caused by mucus involves a combination of strategies to reduce mucus production and enhance its clearance. Bronchodilators and corticosteroids may be prescribed to open the airways and reduce inflammation, while mucolytics can help thin the mucus, making it easier to expel. Techniques such as postural drainage, percussion, and breathing exercises are also effective in mobilizing and clearing mucus from the airways. Patients are often educated on proper coughing techniques to expel mucus efficiently without causing additional strain on the respiratory system. Early recognition of whistling, rattling, or bubbling sounds and timely intervention are key to preventing further complications and improving respiratory function.
Mastering the Art of Typing the 'Woo' Sound: Tips and Tricks
You may want to see also
Explore related products






![]()
Cough Variations: Wet coughs expel mucus with loud, phlegmy sounds; dry coughs are sharper, less resonant
Coughing is a reflexive action that serves to clear irritants from the respiratory tract, and the sound it produces can provide valuable insights into the underlying cause. When it comes to Cough Variations: Wet coughs expel mucus with loud, phlegmy sounds; dry coughs are sharper, less resonant, understanding these distinctions is crucial. Wet coughs, often referred to as productive coughs, are characterized by the expulsion of mucus. This type of cough is typically louder and more guttural, with a distinct phlegmy quality. The sound arises because the mucus creates resistance as it moves through the airways, resulting in a bubbling or gurgling noise. This is often indicative of conditions like bronchitis, pneumonia, or chronic obstructive pulmonary disease (COPD), where excess mucus production is a common symptom.
In contrast, dry coughs are non-productive, meaning they do not expel mucus. These coughs are sharper and less resonant, often described as barking, hacking, or tickling. The absence of mucus means there is less dampening of the sound, resulting in a more abrupt and high-pitched noise. Dry coughs are frequently associated with irritants like dust, smoke, or allergies, as well as viral infections such as the common cold or COVID-19 in its early stages. The sharpness of the sound is due to the rapid movement of air through dry, irritated airways without the lubricating presence of mucus.
The distinction between wet and dry coughs is not just auditory but also mechanical. Wet coughs involve the contraction of respiratory muscles to push mucus up from the lungs and out of the body, which requires more effort and produces a prolonged, wet sound. Dry coughs, on the other hand, are often triggered by irritation in the upper respiratory tract, such as the throat or larynx, leading to a quicker, more sudden expulsion of air. This difference in mechanism directly influences the sound produced, making it a key diagnostic clue for healthcare providers.
Listening to the sounds of the lungs with mucus can further elucidate these variations. During auscultation, a wet cough may be accompanied by crackles or rales, which are caused by air moving through mucus-filled airways. These sounds are often described as popping or bubbling and are more pronounced during inhalation. In contrast, a dry cough may be associated with wheezing, a high-pitched whistling sound caused by narrowed airways, or stridor, a harsh, vibrating noise indicating upper airway obstruction. These additional sounds complement the cough itself, providing a fuller picture of respiratory health.
Finally, recognizing these cough variations is essential for both self-assessment and medical evaluation. Wet coughs with loud, phlegmy sounds often require treatment to address the underlying mucus production, such as expectorants or antibiotics for infection. Dry coughs, with their sharper, less resonant tones, may benefit from cough suppressants or addressing the irritant causing the cough. By paying attention to the specific qualities of a cough, individuals can better communicate their symptoms to healthcare providers, leading to more accurate diagnoses and effective treatment plans. Understanding how lungs sound with mucus through these cough variations is a valuable skill for anyone seeking to maintain respiratory health.
How White Noise Masks Unwanted Sounds for Better Sleep and Focus
You may want to see also
Explore related products






![]()
Lung Region Effects: Upper airway mucus sounds higher-pitched; lower lung mucus sounds deeper and more resonant
When assessing lung sounds in the presence of mucus, it's crucial to understand how the location of mucus within the respiratory tract influences the auditory characteristics. The upper airway, including the trachea and larger bronchi, tends to produce higher-pitched sounds when mucus is present. This is because the narrower and more rigid structures in this region amplify higher-frequency sounds. As air moves through mucus-laden upper airways, it creates turbulence, resulting in a distinct, musical, or whistling quality. These sounds are often described as adventitious breath sounds, such as rhonchi, which are continuous, low-pitched, and snoring-like but can also present with a higher pitch when mucus is more superficial or in smaller airways.
In contrast, mucus in the lower lung regions, such as the smaller bronchioles and alveoli, produces deeper and more resonant sounds. The increased diameter and compliance of these airways allow for lower-frequency sounds to dominate. When mucus accumulates in these areas, it can lead to a gurgling or rattling noise, often referred to as crackles or rales. These sounds are typically heard during inspiration and are caused by the sudden popping open of mucus-filled airways. The depth and resonance of these sounds are a direct result of the larger air columns and slower air movement in the lower lung regions.
The difference in sound between upper and lower airway mucus can be attributed to the varying acoustic properties of the respiratory tract. The upper airway acts as a high-frequency filter, amplifying sounds above 1000 Hz, while the lower airways emphasize frequencies below 500 Hz. This distinction is essential for healthcare professionals when using auscultation to diagnose respiratory conditions. For instance, high-pitched mucus sounds in the upper airway may indicate conditions like acute bronchitis or asthma, whereas deeper, resonant sounds in the lower lungs could suggest pneumonia or chronic obstructive pulmonary disease (COPD) with mucus plugging.
To effectively differentiate between these sounds, proper auscultation techniques are vital. Using a stethoscope, clinicians should listen carefully during both inspiration and expiration, noting the pitch, intensity, and quality of the sounds. Higher-pitched mucus sounds in the upper airway are often more prominent during expiration, while lower lung mucus sounds may be more audible during inspiration. By correlating these auditory findings with patient history and other clinical signs, healthcare providers can make more accurate diagnoses and develop targeted treatment plans.
Understanding the relationship between lung region and mucus sound characteristics also aids in monitoring patient progress. For example, as mucus is cleared from the upper airway, the higher-pitched sounds may diminish, indicating improvement. Conversely, the persistence or development of deeper, resonant sounds in the lower lungs might signal worsening conditions or the need for more aggressive interventions, such as chest physiotherapy or bronchodilators. This knowledge empowers healthcare professionals to provide more effective and personalized care for patients with respiratory issues.
In summary, the presence of mucus in different lung regions significantly affects the auditory characteristics of lung sounds. Upper airway mucus produces higher-pitched sounds due to the narrower and more rigid structures, while lower lung mucus results in deeper, more resonant sounds because of the larger and more compliant airways. Recognizing these distinctions is essential for accurate diagnosis, treatment planning, and patient monitoring. By mastering the auscultation of these sounds, healthcare providers can enhance their ability to manage a wide range of respiratory conditions effectively.
Unveiling the Impact: How Sound Frequencies Influence Human Mind and Body
You may want to see also
Explore related products





![]()
Infection Influence: Infected mucus often produces louder, more persistent gurgling or crackling sounds
When mucus becomes infected, typically due to bacterial or viral pathogens, it undergoes changes in consistency and volume, which directly affect the sounds produced in the lungs. Infected mucus tends to be thicker and more abundant than normal mucus, leading to louder and more persistent gurgling or crackling sounds during breathing. These sounds, often described as rales or rhonchi, occur as air moves through airways narrowed or partially obstructed by the infected mucus. The increased viscosity and volume of the mucus create greater resistance to airflow, amplifying the noise as it vibrates against the airway walls.
The persistence of these sounds is a key indicator of infection. Healthy lungs with minimal mucus produce minimal or no audible sounds during breathing. However, infected mucus accumulates and adheres to the airway lining, causing continuous turbulence as air passes through. This results in crackling sounds that are often heard during inhalation and sometimes exhalation. The crackles may be fine or coarse, depending on the mucus distribution and thickness, with coarser sounds typically associated with larger airways affected by heavier mucus buildup.
Infection-related gurgling sounds are particularly noticeable during deep breaths or when lying down, as gravity causes the mucus to pool in the lower airways. These sounds are not only louder but also more consistent compared to those caused by non-infected mucus. For example, a mild cold with thin mucus might produce occasional crackles, while a bacterial pneumonia with thick, infected mucus will generate continuous, pronounced gurgling or rattling noises. This distinction is crucial for healthcare providers when diagnosing respiratory infections.
The mechanism behind these sounds involves the interaction between air, mucus, and the airway walls. Infected mucus often contains inflammatory cells, debris, and pathogens, which further increase its density and stickiness. As air attempts to move past these obstructions, it creates small bubbles or pockets within the mucus, leading to the characteristic crackling or popping sounds. Over time, if the infection persists, these sounds may become more widespread and intense, reflecting the progression of the infection and the increasing burden on the lungs.
To address these sounds, treatment focuses on clearing the infected mucus and resolving the underlying infection. Techniques such as chest physiotherapy, inhalation of hypertonic saline, or the use of mucolytic medications can help thin the mucus, making it easier to expel. Antibiotics or antiviral drugs may be prescribed to target the infection directly. By reducing mucus volume and restoring normal airway function, the loud, persistent gurgling or crackling sounds typically subside, indicating improvement in lung health. Recognizing these sounds early can lead to timely intervention and better outcomes for individuals with respiratory infections.
HDMI's Impact on Sound Quality: Enhancing Audio Experience or Myth?
You may want to see also
Frequently asked questions
Mucus in the airways can alter lung sounds by causing rattling, gurgling, or crackling noises due to air moving through the thickened or obstructed passages.
Yes, mucus can amplify breathing sounds, making them louder or more noticeable, especially during inhalation or exhalation.
Wet or "rhonchi" sounds indicate the presence of mucus or fluid in the airways, often associated with conditions like bronchitis, pneumonia, or asthma.