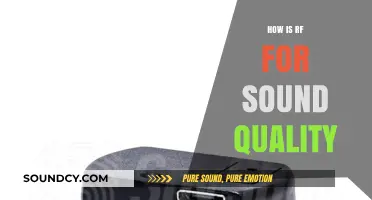
The S1 heart sound, often described as the lub in the lub-dub of the heartbeat, is primarily produced by the closure of the atrioventricular (AV) valves—the mitral valve on the left side and the tricuspid valve on the right side of the heart. This occurs at the beginning of systole, when the ventricles contract and the pressure in the ventricles exceeds that in the atria, causing the AV valves to snap shut. The sound is a result of the sudden stopping of blood flow, the vibration of the valve leaflets, and the associated structures such as the chordae tendineae and papillary muscles. Factors like heart rate, contractility, and valve condition influence the intensity and quality of S1, making it a crucial component in cardiac auscultation for assessing heart function.
| Characteristics | Values |
|---|---|
| Source | Closure of atrioventricular (AV) valves (mitral and tricuspid valves) |
| Timing | Beginning of ventricular contraction (isovolumetric contraction phase) |
| Frequency | 20-60 Hz |
| Duration | 0.1-0.14 seconds |
| Intensity | Louder than S2, best heard at the apex (mitral) and left sternal border (tricuspid) |
| Quality | Dull, low-pitched, and short |
| Mechanism | Rapid increase in ventricular pressure causes AV valves to shut, creating a vibration in the valve leaflets and surrounding structures |
| Associated Factors | Increased ventricular preload or contractility can intensify S1 |
| Pathological Changes | Softening or splitting of S1 may indicate mitral or tricuspid valve pathology |
| Diagnostic Significance | Essential for assessing heart valve function and identifying abnormalities |
Explore related products






What You'll Learn
- Atrioventricular Valve Closure: Tricuspid and mitral valves close, marking end of diastole and start of systole
- Ventricular Contraction: Rapid ventricular muscle contraction creates pressure, generating the S1 sound
- Blood Flow Turbulence: Sudden cessation of blood flow through valves causes vibration and audible sound
- Valve Leaflet Movement: Leaflets snap shut, producing low-frequency vibrations heard as S1
- Sound Transmission: Vibrations travel through blood, tissues, and chest wall to be auscultated
![]()
Atrioventricular Valve Closure: Tricuspid and mitral valves close, marking end of diastole and start of systole
The first heart sound, S1, is primarily produced by the closure of the atrioventricular (AV) valves—the tricuspid and mitral valves. This event marks the end of diastole and the beginning of systole, a critical transition in the cardiac cycle. As the ventricles begin to contract, the pressure in the ventricles exceeds the pressure in the atria, causing the AV valves to snap shut. This sudden closure prevents backflow of blood from the ventricles into the atria, ensuring unidirectional flow of blood through the heart. The tricuspid valve, located between the right atrium and right ventricle, and the mitral (bicuspid) valve, located between the left atrium and left ventricle, are composed of leaflets that coapt tightly when closed, creating the audible sound known as S1.
The mechanism of S1 production involves both the movement of the valve leaflets and the vibration of surrounding structures. When the ventricles contract, the increased pressure forces the AV valves to close rapidly. This rapid closure causes the leaflets to come together with significant force, generating a vibration. The vibration is then transmitted to the surrounding tissues, including the blood, myocardium, and pericardium, which act as resonators. These structures amplify the vibration, converting it into an audible sound wave that can be heard through a stethoscope. The pitch and intensity of S1 are influenced by factors such as the speed of valve closure, the tension in the valve leaflets, and the compliance of the surrounding tissues.
The tricuspid and mitral valves close nearly simultaneously, but the mitral component of S1 is typically louder and higher pitched due to the higher pressure in the left ventricle compared to the right ventricle. This difference in pressure results from the left ventricle's need to pump oxygenated blood to the entire body, whereas the right ventricle pumps deoxygenated blood only to the lungs. The higher pressure in the left ventricle causes the mitral valve to close more forcefully and quickly, producing a more pronounced sound. Clinicians often describe S1 as a "lub" sound, with the mitral component being more dominant in most individuals.
The timing of AV valve closure is crucial for proper cardiac function. It ensures that the ventricles can generate sufficient pressure to eject blood into the aorta and pulmonary artery without wasting energy. If the AV valves fail to close properly, regurgitation can occur, allowing blood to flow backward into the atria during systole. This condition, known as mitral or tricuspid regurgitation, can lead to volume overload in the atria and reduced cardiac output. Thus, the precise closure of the AV valves is essential for maintaining the efficiency and effectiveness of the cardiac cycle.
In summary, the production of the first heart sound, S1, is directly linked to the closure of the tricuspid and mitral valves at the end of diastole and the beginning of systole. This event is characterized by the rapid coaptation of the valve leaflets, which generates vibrations that are amplified by surrounding structures. The mitral component of S1 is typically louder due to the higher pressure in the left ventricle, while the tricuspid component contributes to the overall sound. Proper AV valve closure is vital for preventing regurgitation and ensuring optimal cardiac function, making S1 a key auscultatory marker in assessing heart health.
Exploring the Unique Pronunciation and Usage of the Lon U Sound
You may want to see also
Explore related products






![]()
Ventricular Contraction: Rapid ventricular muscle contraction creates pressure, generating the S1 sound
The first heart sound, S1, is primarily produced during the rapid contraction of the ventricles, marking the beginning of systole. This phase of the cardiac cycle is crucial for understanding the origin of S1. When the electrical signal from the atrioventricular (AV) node reaches the ventricles, it triggers a rapid and synchronized contraction of the ventricular muscle fibers. This contraction is not merely a passive event but a powerful, coordinated action that sets the stage for the production of the S1 sound. The force generated by the ventricular muscles is essential, as it creates the necessary pressure changes within the heart.
As the ventricles contract, the pressure inside them rises rapidly. This increase in pressure is a direct result of the forceful shortening of the ventricular muscle cells. The pressure wave generated during this contraction is not confined to the ventricles; it propagates through the blood and the heart structures. When this pressure wave reaches the atrioventricular valves (tricuspid and mitral valves), it causes them to close abruptly. The closure of these valves is a critical event in the production of S1, as it creates a distinct, audible sound.
The rapid ventricular contraction and subsequent valve closure are key to understanding the S1 sound's characteristics. The speed and force of the contraction ensure that the valves close quickly, producing a sharp, high-pitched sound. This sound is often described as a "lub" and is the first component of the familiar "lub-dub" heart sounds. The intensity and quality of S1 can provide valuable clinical information, as any deviations from the normal sound may indicate underlying cardiac issues, such as valve problems or ventricular dysfunction.
Furthermore, the S1 sound is a result of the complex interaction between the contracting ventricles and the blood within the heart chambers. As the ventricles squeeze, they not only increase the pressure but also create a turbulent flow of blood. This turbulence, combined with the sudden valve closure, contributes to the unique acoustic signature of S1. The sound waves generated by these events travel through the chest wall and can be heard using a stethoscope, allowing healthcare professionals to assess cardiac function non-invasively.
In summary, the production of the S1 heart sound is intrinsically linked to the rapid and powerful contraction of the ventricular muscles. This contraction generates a pressure wave that leads to the abrupt closure of the atrioventricular valves, creating the characteristic sound. Understanding this process is fundamental in cardiology, as it provides insights into the heart's mechanical function and allows for the detection of various cardiac abnormalities through auscultation. The S1 sound is a testament to the intricate relationship between the heart's electrical, mechanical, and acoustic properties.
Davinci Resolve: Exploring the Audio Library
You may want to see also
Explore related products






![]()
Blood Flow Turbulence: Sudden cessation of blood flow through valves causes vibration and audible sound
The production of the S1 heart sound is intricately linked to the dynamics of blood flow turbulence, particularly during the sudden cessation of blood flow through the heart valves. When the atria contract, blood is forced into the ventricles, and as the ventricular pressure exceeds atrial pressure, the atrioventricular (AV) valves—the mitral and tricuspid valves—snap shut. This abrupt closure is not a silent event; it is a critical moment that generates the S1 sound. The sudden cessation of blood flow causes turbulence, as the momentum of the moving blood column is rapidly arrested by the valve leaflets coming together. This turbulence creates vibrations in the valve structures, surrounding tissues, and blood itself, which are then transmitted to the chest wall and can be heard through a stethoscope.
The mechanism of turbulence during valve closure is rooted in fluid dynamics. As blood flows through the open AV valves, it maintains laminar flow, moving in parallel layers with minimal resistance. However, when the valves close, the flow is abruptly halted, leading to chaotic, turbulent flow patterns. This turbulence generates kinetic energy, which is converted into acoustic energy—sound waves. The mitral valve, being larger and positioned on the left side of the heart, contributes more significantly to the S1 sound than the tricuspid valve. The vibrations produced by this turbulence are low-frequency and rich in harmonic content, giving the S1 sound its characteristic "lub" quality.
The anatomy and function of the valve leaflets play a crucial role in this process. The leaflets are thin, flexible structures that coapt tightly during closure, minimizing regurgitation. However, their rapid movement and the resulting turbulence are essential for sound production. The stiffness and thickness of the leaflets, as well as the speed of their closure, influence the intensity and frequency of the vibrations. For example, in conditions like mitral stenosis, where the leaflets are thickened and rigid, the S1 sound may be louder due to increased turbulence during closure.
Additionally, the surrounding structures of the heart amplify and transmit these vibrations. The chordae tendineae, papillary muscles, and ventricular walls act as resonating chambers, enhancing the acoustic energy produced by valve closure. This amplification ensures that the sound is detectable during auscultation. The timing of the S1 sound corresponds precisely to the moment of AV valve closure, which occurs at the beginning of ventricular systole. This synchronization is critical for clinicians to correlate the sound with the cardiac cycle and assess heart function.
Understanding blood flow turbulence as the underlying cause of the S1 heart sound highlights the importance of valve dynamics in cardiac auscultation. Any abnormalities in valve structure or function, such as stenosis, regurgitation, or prolapse, can alter the turbulence patterns and, consequently, the characteristics of the S1 sound. For instance, a delayed or split S1 may indicate conduction abnormalities or valve dysfunction. Thus, the study of turbulence during valve closure not only explains the origin of the S1 sound but also provides valuable insights into diagnosing cardiovascular disorders through careful auscultation.
The Accuracy of Ultrasound Imaging: How Reliable Is It?
You may want to see also
Explore related products






![]()
Valve Leaflet Movement: Leaflets snap shut, producing low-frequency vibrations heard as S1
The production of the first heart sound, S1, is primarily attributed to the rapid movement of the atrioventricular (AV) valve leaflets—specifically the mitral and tricuspid valves. As the heart transitions from atrial systole to ventricular systole, the AV valves close abruptly to prevent backflow of blood from the ventricles into the atria. This closure is not a smooth process but rather a dynamic event where the leaflets snap shut. The force and speed of this closure generate vibrations within the valve structures, which are then transmitted through the surrounding tissues and blood. These vibrations occur at low frequencies, typically between 20 to 60 Hz, and are perceived as the S1 sound during auscultation.
The mechanism of leaflet closure involves a combination of pressure changes and anatomical forces. During ventricular contraction, the pressure in the ventricles rapidly exceeds that in the atria, causing the AV valve leaflets to be pushed upward toward the atria. Once the pressure gradient is sufficient, the leaflets coapt (come together) and close. The sudden deceleration of the leaflets as they meet creates a turbulent flow of blood and generates mechanical stress on the valve tissues. This stress is converted into vibrational energy, which propagates as sound waves. The low-frequency nature of these vibrations is due to the larger, more massive structure of the AV valves compared to the semilunar valves, which produce the higher-frequency S2 sound.
The snapping shut of the leaflets is further influenced by the elasticity and tension of the valve apparatus, including the chordae tendineae and papillary muscles. These structures act as a supportive framework, ensuring that the leaflets close efficiently and completely. Any abnormalities in this system, such as stretched chordae or prolapsed leaflets, can alter the dynamics of closure and, consequently, the characteristics of the S1 sound. For example, a more gradual closure may produce a softer or muffled S1, while a more forceful closure can result in a louder, sharper sound.
The transmission of these low-frequency vibrations from the valves to the chest wall, where they are detected by a stethoscope, involves several steps. The vibrations initially travel through the blood and surrounding tissues, including the myocardium and pericardium. The chest wall acts as a resonating chamber, amplifying certain frequencies and allowing them to be audible. The location of S1 auscultation—best heard at the mitral and tricuspid areas—corresponds to the anatomical positions of the AV valves, further emphasizing the role of leaflet movement in sound production.
In summary, the S1 heart sound is directly produced by the rapid snapping shut of the AV valve leaflets during ventricular systole. This movement generates low-frequency vibrations due to the abrupt deceleration and coaptation of the leaflets, which are then transmitted and amplified through the cardiovascular and thoracic structures. Understanding this valve leaflet movement is essential for interpreting the physiological and pathological characteristics of the S1 sound in clinical practice.
Identifying Bad Axle Sounds: Symptoms, Causes, and Repair Tips
You may want to see also
Explore related products






![]()
Sound Transmission: Vibrations travel through blood, tissues, and chest wall to be auscultated
The production of the S1 heart sound is a complex process that involves the generation and transmission of vibrations through various mediums within the body. It begins with the closure of the atrioventricular (AV) valves, namely the mitral and tricuspid valves, at the onset of ventricular systole. As the ventricles contract, the pressure within them rises, causing the AV valves to snap shut, which creates a sudden rush of blood and generates a vibration. This initial vibration is the primary source of the S1 sound. The force and speed of the valve closure, coupled with the tension in the valve leaflets and chordae tendineae, determine the frequency and intensity of the sound produced.
Once generated, these vibrations travel through the blood within the ventricles and atria. Blood acts as a medium that efficiently conducts the sound waves due to its fluid nature and the proximity of the vibrating structures. As the vibrations move through the blood, they encounter the walls of the heart chambers, which are composed of myocardial tissue. This tissue, being denser than blood, further transmits the vibrations with minimal loss of energy. The myocardial walls amplify and direct the sound waves toward the outer surface of the heart, where they interface with the surrounding tissues.
From the heart, the vibrations continue their journey through the layers of tissues in the chest, including fat, muscle, and connective tissue. Each layer contributes to the transmission of sound, though some attenuation occurs due to the varying densities and elastic properties of these tissues. The sound waves are gradually funneled toward the chest wall, where they encounter the skin and subcutaneous tissues. These outer layers act as the final medium through which the vibrations travel before they can be detected by an auscultation device, such as a stethoscope.
The chest wall plays a crucial role in sound transmission, as it must be sufficiently thin and compliant to allow the vibrations to reach the surface without significant damping. Factors such as chest wall thickness, the presence of subcutaneous fat, and the tension in the overlying skin can influence the clarity and intensity of the transmitted sound. When the vibrations reach the chest wall, they create minute fluctuations in pressure that can be captured by the diaphragm or bell of a stethoscope. This conversion of mechanical vibrations into audible sound waves allows healthcare providers to auscultate the S1 heart sound and assess cardiac function.
Finally, the stethoscope acts as the interface between the patient’s body and the listener’s ear, amplifying and transmitting the captured vibrations. The design of the stethoscope, including the material and size of the diaphragm or bell, affects the frequency range and quality of the sound heard. Proper placement of the stethoscope over the optimal auscultation sites, such as the mitral or tricuspid areas, ensures that the S1 sound is clearly audible. Thus, the transmission of vibrations from the heart valves, through blood, tissues, and the chest wall, to the auscultation device, is a multifaceted process that underpins the detection and interpretation of the S1 heart sound.
Alligators in Currituck Sound: Fact or Fiction?
You may want to see also
Frequently asked questions
The S1 heart sound is primarily caused by the closure of the mitral and tricuspid valves at the beginning of systole, marking the start of ventricular contraction.
As the ventricles contract, the pressure in the ventricles exceeds the pressure in the atria, causing the mitral and tricuspid valves to close. This closure prevents backflow of blood into the atria and creates the low-pitched, dull S1 sound due to the vibration of the valve leaflets and surrounding structures.
The intensity and quality of the S1 sound can be influenced by factors such as heart rate, contractility of the myocardium, valve structure, and the presence of pathologies like mitral stenosis or regurgitation, which can alter the normal vibration patterns of the valves.