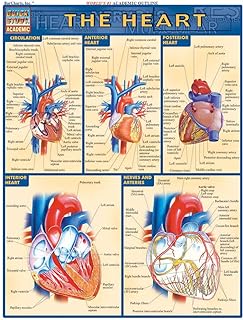
The lub sound, a fundamental component of the heartbeat, is produced by the closing of the atrioventricular (AV) valves—the mitral and tricuspid valves—during the cardiac cycle. This occurs at the beginning of systole, when the ventricles contract and the AV valves snap shut to prevent blood from flowing back into the atria. The abrupt closure of these valves creates a distinct vibration that resonates through the chest wall, resulting in the audible lub sound, also known as the first heart sound (S1). This sound is a critical indicator of proper valve function and is routinely assessed during auscultation to evaluate cardiovascular health. Understanding the mechanics behind the lub sound provides valuable insights into the intricate processes of the heart's rhythmic contractions and blood flow dynamics.
| Characteristics | Values |
|---|---|
| Source | The "lub" sound, also known as the first heart sound (S1), is primarily caused by the closure of the mitral valve (between the left atrium and left ventricle) and the tricuspid valve (between the right atrium and right ventricle). |
| Timing | Occurs at the beginning of ventricular systole (contraction of the ventricles). |
| Mechanism | The sudden increase in pressure within the ventricles causes the valve leaflets to snap shut, creating a low-pitched, dull sound. |
| Frequency | Typically heard at a lower frequency range, around 20-60 Hz. |
| Duration | Lasts approximately 0.1 to 0.15 seconds. |
| Associated Factors | Influenced by factors like heart rate, blood pressure, valve structure, and cardiac muscle strength. |
| Clinical Significance | Abnormalities in the "lub" sound (e.g., splitting, muffling, or absence) can indicate valve disorders, heart failure, or other cardiac conditions. |
Explore related products






What You'll Learn
- Ventricular Contraction: Blood rushes into aorta/pulmonary artery, creating first heart sound (S1)
- Semilunar Closure: Aortic/pulmonary valves shut, producing the sharp lub component of S1
- Atrial Contraction: Atrial blood fills ventricles, enhancing S1’s intensity and clarity
- Valve Anatomy: Healthy leaflets ensure crisp closure, contributing to distinct lub sound
- Blood Flow Dynamics: Velocity and volume of blood impact S1’s acoustic quality
![]()
Ventricular Contraction: Blood rushes into aorta/pulmonary artery, creating first heart sound (S1)
The first heart sound, often referred to as the "lub" sound, is a fundamental component of the cardiac cycle and is directly linked to ventricular contraction. When the ventricles contract, a process known as systole begins. This powerful contraction generates a significant force, causing blood to be rapidly ejected from the ventricles. The blood rushes out of the ventricles and into the major arteries—specifically, the aorta and the pulmonary artery. This sudden, forceful movement of blood is a critical event in the creation of the first heart sound.
As the ventricles contract, the atrioventricular (AV) valves, which are the tricuspid and mitral valves, play a crucial role. These valves are forced shut due to the increased pressure in the ventricles, preventing blood from flowing back into the atria. The closure of these valves is not silent; instead, it produces a distinct sound. This sound is a result of several factors, including the rapid deceleration of blood, the vibration of the valve leaflets, and the resonance within the cardiovascular structures. The AV valves snapping shut is the primary mechanism behind the generation of the first heart sound, S1.
The rush of blood into the aorta and pulmonary artery is immediate and under high pressure. This rapid flow causes turbulence, which contributes to the acoustic phenomenon. The sound is then transmitted through the walls of the arteries and surrounding tissues, allowing it to be heard through a stethoscope. The intensity and quality of S1 can provide valuable insights into the health of the heart valves and the overall cardiac function. For instance, a loud S1 may indicate increased blood flow or high blood pressure, while a soft or muffled sound could suggest valve problems or reduced cardiac output.
It is important to note that the timing of this event is precise and coordinated. The ventricular contraction must be synchronized with the closure of the AV valves to ensure efficient blood flow. Any delay or dysfunction in this process can lead to abnormal heart sounds or murmurs, which may indicate underlying cardiac issues. Understanding this mechanism is essential for medical professionals to diagnose and assess cardiovascular health.
In summary, the "lub" sound, or S1, is a direct consequence of ventricular contraction and the subsequent rush of blood into the aorta and pulmonary artery. This process involves the rapid closure of the AV valves, creating a unique acoustic signature. The study of these heart sounds provides a non-invasive method to evaluate the heart's performance and identify potential abnormalities, making it a vital aspect of cardiovascular diagnostics.
Fixing Chrome's Silent Treatment: No Sound Issues
You may want to see also
Explore related products






![]()
Semilunar Closure: Aortic/pulmonary valves shut, producing the sharp lub component of S1
The "lub" sound, the first component of the heart’s S1 heart sound, is primarily produced by the closure of the semilunar valves—specifically the aortic and pulmonary valves. This event occurs at the end of ventricular contraction, or systole, when the ventricles have ejected blood into the aorta and pulmonary artery. As the ventricles begin to relax and enter diastole, the pressure in these chambers drops below the pressure in the aorta and pulmonary artery. This pressure differential causes the aortic and pulmonary valves to snap shut, preventing backflow of blood into the ventricles. The abrupt closure of these valves creates a sharp, high-pitched sound, which is the "lub" component of the S1 heart sound.
The mechanism behind the semilunar valve closure is rooted in the anatomy and function of these valves. Both the aortic and pulmonary valves are composed of three cusps or leaflets, which are attached to the aortic and pulmonary roots, respectively. During systole, these leaflets are pushed open by the force of blood ejection. As systole ends and ventricular pressure decreases, the leaflets are forced back toward the ventricles by the higher pressure in the aorta and pulmonary artery. When the leaflets coapt (come together), they abruptly close, creating a vibration in the surrounding tissues and structures, such as the aorta, pulmonary artery, and ventricular walls. This vibration is transmitted to the chest wall and is audible as the "lub" sound through a stethoscope.
The sharpness and distinctness of the "lub" sound are influenced by several factors, including the speed and force of valve closure, the integrity of the valve leaflets, and the compliance of the adjacent structures. Healthy semilunar valves close rapidly and completely, producing a crisp sound. Any abnormalities, such as valve stiffness, calcification, or regurgitation, can alter the quality of the sound. For example, a bicuspid aortic valve or aortic stenosis may result in a softer or delayed "lub" due to impaired leaflet function. Understanding these factors is crucial for clinicians interpreting heart sounds and diagnosing valvular disorders.
The timing of semilunar valve closure is also critical to the production of the "lub" sound. It occurs at the very beginning of ventricular diastole, coinciding with the onset of the electrocardiogram (ECG) T wave. This precise timing ensures that the "lub" sound is synchronized with the end of the QRS complex, which represents ventricular depolarization and contraction. The coordination between electrical and mechanical events in the heart is essential for the clear delineation of S1, with the "lub" sound marking the transition from systole to diastole. This synchronization is a key feature of a normal cardiac cycle and is used in clinical assessments to evaluate heart function.
In summary, the "lub" sound of the S1 heart sound is generated by the abrupt closure of the aortic and pulmonary semilunar valves at the end of ventricular systole. This closure is driven by the pressure differential between the ventricles and the aorta/pulmonary artery, causing the valve leaflets to coapt and produce a sharp vibration. The sound’s characteristics depend on valve health, closure dynamics, and timing within the cardiac cycle. Understanding this process is fundamental to interpreting heart sounds and diagnosing cardiovascular conditions related to semilunar valve function.
Decoding Sound: How Computers Encode Audio Signals Digitally
You may want to see also
Explore related products






![]()
Atrial Contraction: Atrial blood fills ventricles, enhancing S1’s intensity and clarity
The 'lub' sound, known as S1, is primarily generated by the closure of the atrioventricular (AV) valves—the tricuspid and mitral valves—at the beginning of ventricular systole. This process is intricately linked with atrial contraction, which plays a crucial role in enhancing the intensity and clarity of S1. During atrial contraction, also called atrial systole, the atria forcefully push blood into the ventricles, ensuring they are maximally filled before ventricular contraction begins. This additional volume of blood increases the pressure differential across the AV valves, causing them to close more abruptly and forcefully, thereby amplifying the S1 sound.
Atrial contraction is particularly important when the ventricles are not fully filled by passive blood flow alone, such as during rest or in certain physiological states. By actively contributing to ventricular filling, atrial contraction ensures that the AV valves snap shut with greater velocity and force. This rapid closure creates turbulence in the blood flow, which vibrates the valve leaflets, surrounding structures, and the blood itself. These vibrations are transmitted through the chest wall and detected as the 'lub' sound during auscultation. Without atrial contraction, the ventricles would receive less blood, leading to a softer, less distinct S1.
The mechanism behind this enhancement lies in the Frank-Starling mechanism, which states that the force of ventricular contraction is directly proportional to the initial stretch of the cardiac muscle fibers. Atrial contraction increases preload—the volume of blood in the ventricles at the end of diastole—which stretches the ventricular walls further. This increased stretch results in a more powerful ventricular contraction, generating a stronger pressure wave that slams the AV valves shut. The greater the force of closure, the louder and clearer the S1 sound becomes.
Additionally, atrial contraction ensures synchrony in the filling process, allowing both ventricles to receive an adequate and equal volume of blood. This synchronized filling optimizes the hemodynamic conditions for AV valve closure, minimizing any delays or inconsistencies that could diminish the S1 sound. In conditions where atrial contraction is impaired, such as atrial fibrillation, the S1 intensity often decreases due to reduced atrial contribution to ventricular filling.
In summary, atrial contraction is essential for maximizing ventricular filling, which in turn enhances the intensity and clarity of the S1 heart sound. By increasing preload and ensuring synchronized filling, atrial contraction creates the optimal conditions for the forceful closure of the AV valves, generating the distinct 'lub' sound. Understanding this relationship highlights the critical role of atrial function in the cardiac cycle and the auscultatory findings associated with it.
Unveiling the Unique Vocalizations: How Does a Koala Bear Sound?
You may want to see also
Explore related products






![]()
Valve Anatomy: Healthy leaflets ensure crisp closure, contributing to distinct lub sound
The lub sound, the first component of the iconic heartbeat, is primarily attributed to the precise closure of the heart’s atrioventricular valves—the mitral valve on the left and the tricuspid valve on the right. These valves are composed of flexible, yet resilient leaflets (two for the mitral, three for the tricuspid) that ensure unidirectional blood flow. During the cardiac cycle, as the atria contract to push blood into the ventricles, the leaflets remain open. However, when the ventricles begin to contract (systole), the sudden increase in pressure causes these leaflets to snap shut, preventing backflow into the atria. This crisp closure of healthy leaflets is the mechanical event that generates the lub sound.
The anatomy of the valve leaflets is critical to this process. Healthy leaflets are thin, pliable, and free from calcification, scarring, or deformities, allowing them to coapt (meet) perfectly at the end of diastole. This seamless coaptation ensures that the closure is abrupt and complete, creating a distinct vibration that resonates through the chest wall and is audible via stethoscope. Any deviation in leaflet structure or function, such as prolapse or stenosis, can result in incomplete or delayed closure, altering the quality of the sound.
The lub sound corresponds to the transition from diastole to systole, specifically the moment when the atrioventricular valves close (mitral and tricuspid valve closure). This closure is synchronized with the electrical signal from the atrioventricular node, ensuring that the mechanical and electrical events of the heart are tightly coordinated. The force of ventricular contraction, combined with the sudden cessation of blood flow due to leaflet closure, creates a pressure wave that vibrates the surrounding tissues, producing the low-pitched, dull lub sound.
Healthy valve leaflets play a pivotal role in the clarity and distinctness of this sound. Their elasticity and smooth surfaces minimize turbulence during closure, ensuring that the sound is sharp and well-defined. In contrast, diseased leaflets may allow regurgitation or close sluggishly, leading to murmurs or muffled sounds that overlap with the expected lub. For example, mitral valve prolapse can cause a clicking sound preceding the lub, while stenosis may produce a delayed or split closure sound.
Understanding the relationship between valve anatomy and the lub sound is essential for clinical assessment. Auscultation of the heart relies on the consistency and quality of these sounds to identify abnormalities. Healthy leaflets not only ensure efficient blood flow but also act as acoustic markers of cardiac health. Thus, the lub sound is a direct reflection of the anatomical integrity and functional precision of the atrioventricular valves, making it a fundamental component of cardiovascular diagnosis.
Bose SoundSport Review: Crisp Audio, Comfortable Fit, and Durability Tested
You may want to see also
Explore related products




![]()
Blood Flow Dynamics: Velocity and volume of blood impact S1’s acoustic quality
The first heart sound, often referred to as the "lub" sound (S1), is a critical component of the cardiac cycle, and its acoustic quality is directly influenced by the dynamics of blood flow within the heart. This sound is primarily generated by the closure of the atriovental valves—the mitral valve on the left side and the tricuspid valve on the right side of the heart. The velocity and volume of blood flow play pivotal roles in determining the characteristics of S1. When the ventricles begin to contract during systole, blood is rapidly accelerated, creating a high-velocity flow. This sudden increase in velocity causes the atrioventricular valves to slam shut, producing the audible "lub" sound. The faster the blood accelerates, the more abrupt and forceful the valve closure, resulting in a sharper and louder S1.
The volume of blood entering the ventricles during diastole, known as the preload, also significantly impacts the acoustic quality of S1. A higher preload means more blood is available to be ejected during systole, increasing the force required to close the atrioventricular valves. This greater force amplifies the sound intensity of S1, making it more pronounced. Conversely, a lower preload results in less blood volume and reduced force, leading to a softer and less distinct "lub" sound. Clinicians often assess the volume status of a patient by evaluating the quality of S1, as it provides valuable insights into the heart's filling dynamics.
Blood velocity, driven by ventricular contraction, is another critical factor in S1's acoustic characteristics. During a vigorous contraction, the ventricles generate a rapid and forceful ejection of blood, causing the atrioventricular valves to close with greater speed and impact. This results in a crisp and well-defined S1. In contrast, a weaker contraction leads to slower blood velocity and a less forceful valve closure, producing a muted or diminished "lub" sound. Conditions such as myocardial ischemia or heart failure, which impair ventricular contractility, can thus alter the acoustic quality of S1.
The interplay between blood velocity and volume is further highlighted in pathological conditions. For instance, in mitral stenosis, the narrowed valve restricts blood flow from the left atrium to the left ventricle, reducing both velocity and volume. This results in a softer and often delayed S1. Similarly, in conditions like aortic stenosis, where blood flow from the left ventricle to the aorta is obstructed, the increased afterload can lead to a more forceful but potentially abnormal S1 due to the heightened pressure required for ejection. Understanding these dynamics is essential for diagnosing and managing cardiovascular disorders.
In summary, the velocity and volume of blood flow are fundamental determinants of the acoustic quality of the first heart sound (S1). High-velocity flow and increased blood volume during systole lead to a sharp and loud "lub" sound, while reduced velocity and volume result in a softer or diminished sound. Clinicians rely on these acoustic cues to assess cardiac function and identify underlying pathologies. By analyzing the dynamics of blood flow, healthcare professionals can gain valuable insights into the heart's mechanical performance and overall health.
The Evolution of Sound in 1930s Cinema
You may want to see also
Frequently asked questions
The lub sound, also known as S1, is caused by the closure of the atrioventricular (AV) valves—the tricuspid and mitral valves—at the beginning of ventricular contraction (systole).
The lub sound occurs first because it marks the start of systole, when the ventricles contract and the AV valves close. The dub sound (S2) follows later, marking the closure of the semilunar valves (aortic and pulmonary) at the end of systole.
Yes, the lub sound is a normal component of the heart’s rhythmic cycle. It indicates the beginning of ventricular contraction and proper functioning of the AV valves. Abnormalities in the lub sound may suggest valve issues or other cardiac problems.